
Abstract
Background
Multimorbidity, defined as the coexistence of two or more chronic diseases in a single individual, is a growing public health challenge globally and particularly in Saudi Arabia.
Aims
This narrative review aims to synthesize existing literature on multimorbidity in Saudi Arabia by examining its prevalence, identifying gender-based differences, and highlighting the most commonly associated chronic diseases.
Methods
A structured search was conducted using PubMed, Google Scholar, and institutional databases, including Scopus and Web of Science, for English-language studies on multimorbidity in Saudi Arabia published between 2015 and 2025. Boolean operators were applied, and reference lists were screened to ensure comprehensive coverage while minimizing duplication. A total of 17 studies were included, and data were extracted on study design, population, sample size, multimorbidity prevalence, and gender-specific findings. These were analyzed thematically to identify patterns, disparities in gender, and disease clusters.
Results
Multimorbidity prevalence in Saudi Arabia ranged from 7.1% to 77.6%, with notably higher rates among women, especially in older age groups. Among the five studies that reported disease-specific patterns, diabetes mellitus was the most frequently cited chronic condition, ranking first in three studies. Other frequently reported conditions included hypertension and dyslipidemia, though their ranking varied across studies.
Conclusion
This review highlights the evolving landscape of multimorbidity in Saudi Arabia. Findings call for gender-sensitive, integrated care models that address the clustering of chronic conditions. To address persistent gaps, future research should prioritize mental health integration, early-onset multimorbidity, and ensuring better representation of rural populations. Policymakers should invest in national screening programs, strengthen data systems, and embed equity into care delivery in line with Vision 2030 reforms.
Introduction
The prevalence of multimorbidity in Saudi Arabia and globally is estimated at 23.3% and 37.2%, respectively.1,2 Multimorbidity is defined as living with two or more chronic conditions 3 and has become an increasingly important public health concern due to its impact on healthcare systems and patients’ quality of life. Studies have shown that multimorbidity is significantly associated with increased disability among older adults, 4 and is influenced by factors such as age, gender, lower socioeconomic status, and mental health conditions. 5 It has also been linked to lower quality of life, 6 increased risk of mortality, 7 and a greater likelihood of progressive functional decline (increasing difficulty with daily activities) over time. 8
In Saudi Arabia, the burden of multimorbidity is particularly pronounced, reflecting the high prevalence and co-occurrence of non-communicable diseases (NCDs). NCDs account for 67.6% of all deaths in the country, with ischemic heart disease being the leading cause at 47.2 deaths per 100,000 population, followed by kidney diseases (21.1), hypertensive heart disease (20.7), and diabetes mellitus (13.7). 9 These conditions frequently coexist in individuals, forming common multimorbidity clusters that place significant strain on healthcare services.
Recent systematic reviews have consistently shown that multimorbidity is more prevalent among women than men in the Middle East. A review of 282 studies found a strong association between female gender, age, and multimorbidity, with women reporting higher psychological distress and lower functional score. 10 Another meta-analysis of studies from 2009– 2020 confirmed significantly higher odds of multimorbidity among women in low- and middle-income countries (LMICs), including the Middle East. 11 These disparities may be partly due to behavioral characteristics, as women are more likely to seek care and use General practitioner (GP) services more than men, leading to greater detection.12,13
Beyond its rising prevalence, multimorbidity poses critical challenges both globally and within Saudi Arabia’s healthcare system. It is associated with increased healthcare utilization and a high prevalence of polypharmacy, reported at 46% among older adults. 14 Additionally, care fragmentation remains a major barrier to effective management, particularly for individuals having multiple conditions. 15
To the best of our knowledge, no studies in Saudi Arabia have conducted a comprehensive narrative review specifically focused on multimorbidity. Existing research has largely concentrated on individual chronic diseases such as diabetes, hypertension, or cardiovascular conditions or on comorbidity patterns within specific subgroups, such as the elderly. However, a broader understanding of multimorbidity patterns across the general population remains lacking. This paper aims to address this gap by reviewing the published literature on the prevalence of multimorbidity in Saudi Arabia, examining gender differences, and identifying the most common disease combinations. These insights are essential for informing public health planning, optimizing resource allocation, and adapting clinical care models to better serve patients with multiple chronic conditions.
Materials and methods
Search strategy
A structured literature search was conducted using the terms: (“multimorbidity” OR “multiple chronic conditions” OR “chronic diseases”) AND (“Saudi Arabia”). Boolean operators were applied to combine search terms appropriately. Filters were used to limit results to human studies published in English between 2015 and 2025. The search was performed using PubMed, Google Scholar, and institutional access to full-text databases, including Scopus, Web of Science, CINAHL and EBSCO. Although not all databases were searched independently, many of the included studies were indexed across multiple platforms such as Scopus, CINAHL and Web of Science. Additionally, reference lists of relevant articles were screened to identify further eligible studies. This approach was intended to ensure comprehensive coverage of the literature while minimizing duplication across overlapping sources.
Inclusion and exclusion criteria
The selection process followed a structured approach based on predefined eligibility criteria. Studies were included if they were published between 2015 and 2025, written in English, conducted in Saudi Arabia, and reported the prevalence of multimorbidity. Only observational study designs specifically cross-sectional, retrospective, or cohort studies, were considered. Studies were excluded if they were conducted outside Saudi Arabia (unless used for contextual comparison), did not focus on prevalence data, or were non-original publications such as reviews, editorials, and case reports.
The inclusion period of 2015 to 2025 was selected to capture multimorbidity prevalence trends over the past decade, providing a contemporary view of disease patterns relevant to current healthcare priorities and policy planning in Saudi Arabia. Two studies with data collection periods partially preceding 2015 (2000–2018 and 2012–2020) were included due to their large sample sizes, nationwide scope, and unique contributions to gender-specific, chronic, and communicable disease pattern analysis. These studies provided insights not available in more recent literature and were deemed highly relevant to the review objectives
Titles and abstracts were screened first, followed by full-text reviews to confirm eligibility. While the primary inclusion criterion was a definition of multimorbidity as ≥2 chronic conditions, studies that reported participants having ≥3 chronic diseases in their results were also included, as they aligned with the review’s focus on disease clustering and burden.
Study selection and data extraction
A total of 17 studies were included in this review based on the defined criteria. Data from each included study were extracted into structured tables including author(s) and publication year, study design and period, study population, location, sample size, reported prevalence of multimorbidity, diseases and gender-specific findings.
Data extraction was conducted collaboratively, with all authors contributing to the process. A shared online spreadsheet was used to organize and record key study characteristics. Each entry was reviewed and cross-checked by other team members to ensure accuracy and consistency. Discrepancies were resolved through group discussion and consensus.
Thematic analysis approach
A thematic narrative synthesis approach was adopted to organize and interpret findings across the included studies. This method was selected to enable structured comparison across heterogeneous study designs, populations, and measurement tools. The themes were pre-specified based on the study objectives and refined iteratively during the data extraction phase. This ensured consistency in identifying patterns while allowing flexibility to incorporate emerging insights.
Three major themes guided the synthesis:
(1) Prevalence of multimorbidity, which captured the variability in reported rates across different populations and regions; (2) Gender-based differences, which highlighted disparities between men and women in disease burden and patterns; and (3) Common chronic disease clusters, focusing on frequently co-occurring conditions.
Each study was reviewed and assigned thematically, with findings organized into comparative tables/figures. Within each theme, we examined consistencies, contradictions, and contextual explanations. This structured synthesis allowed us to identify national trends while accounting for study-level variation and to draw meaningful conclusions relevant to both practice and policy.
Quality appraisal
Critical appraisal of included cross-sectional studies using the JBI checklist.

Note. N/A: Not Applicable.
Critical appraisal of the included cohort study using the JBI checklist.

Note. N/A: Not Applicable.
Results
Figure 1 illustrates a Heatmap showing the presence of the reported chronic diseases across five studies conducted in Saudi Arabia focusing on individuals with multimorbidity. Diabetes and hypertension were the most widely reported conditions (in all five studies), while diseases such as depression and dementia were rarely mentioned. Heatmap of the most common chronic diseases among individuals with multimorbidity in Saudi Arabia.
Figure 2 illustrates a line graph comparing the prevalence of multimorbidity between males and females across different study periods in Saudi Arabia. Prevalence of multimorbidity by gender across study periods. Note. Percentages have been rounded to the nearest whole number for clarity.
Figure 3 shows the forest plot showing the prevalence estimates of multimorbidity across studies conducted in Saudi Arabia. The red dashed line represents the mean prevalence across all studies. Multimorbidity prevalence across studies in Saudi Arabia.
Figure 4 Forest plot comparing multimorbidity prevalence by gender across seven studies. Blue dots indicate male participants, and red dots indicate female participants. Horizontal lines connect prevalence estimates for male and female participants within each study. Gender-based differences in multimorbidity prevalence across studies.
Discussion
Methodological quality appraisal of included studies
A critical appraisal was conducted using the JBI checklists for cross-sectional and cohort studies to assess methodological quality. Among the 16 cross-sectional studies, overall quality scores ranged from 3 to 8 out of 8, with an average score of 6. Five studies were rated as high quality (scores 7–8), ten as moderate quality (scores 5–6), and one as low quality (score <5). The sole cohort study scored 7 out of 11, indicating moderate quality. Overall, the included studies demonstrated variable methodological rigor.
Descriptive profile of included studies in Table 3
Prevalence of multimorbidity in Saudi Arabia.
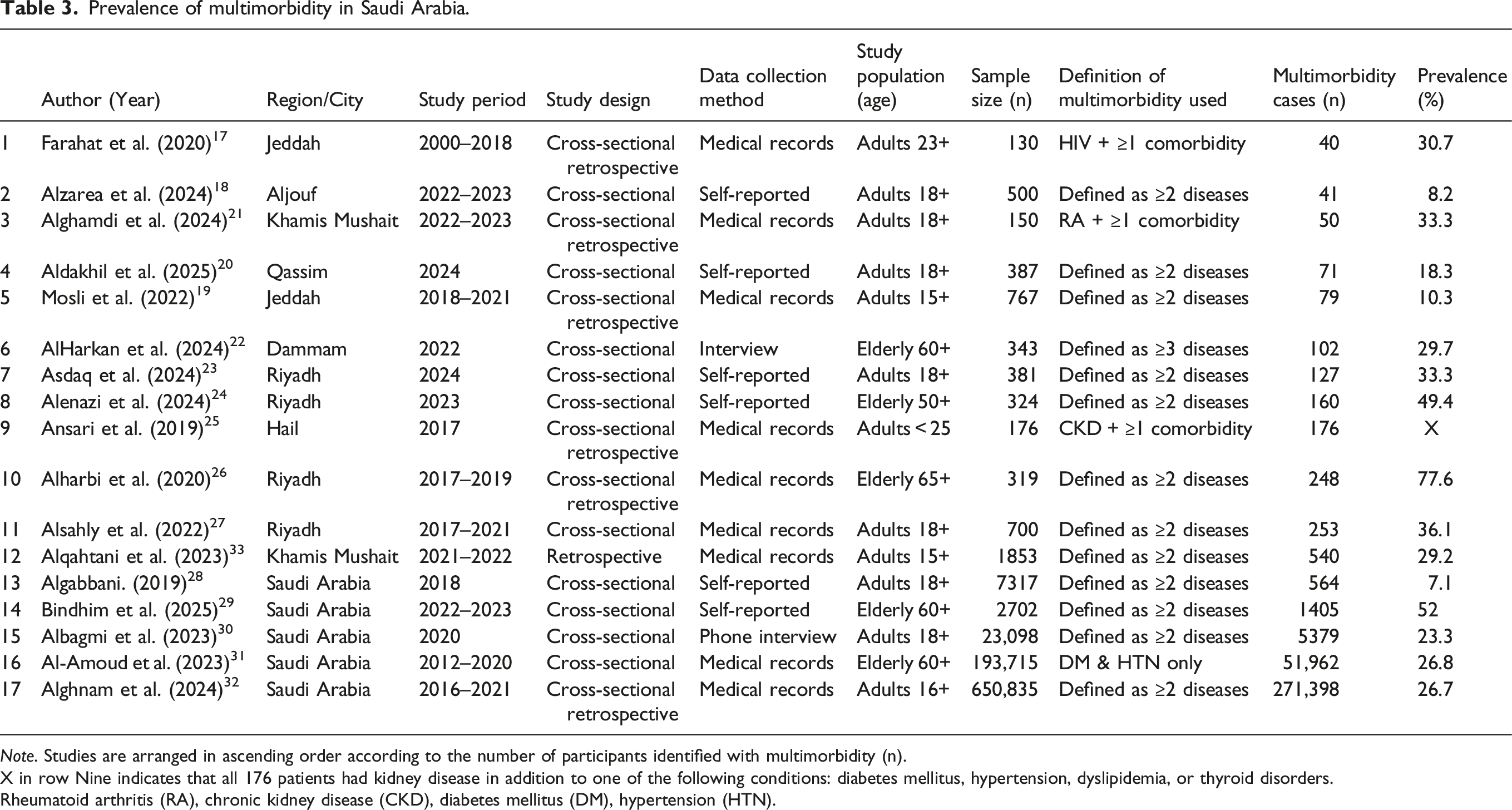
Note. Studies are arranged in ascending order according to the number of participants identified with multimorbidity (n).
X in row Nine indicates that all 176 patients had kidney disease in addition to one of the following conditions: diabetes mellitus, hypertension, dyslipidemia, or thyroid disorders.
Rheumatoid arthritis (RA), chronic kidney disease (CKD), diabetes mellitus (DM), hypertension (HTN).
Figure 3 shows a forest plot of multimorbidity prevalence across studies, the red dashed vertical line represents the mean prevalence (≈30.2%), 25 was excluded from the forest plot since all included patients had chronic kidney disease with at least one additional chronic condition, resulting in 100% multimorbidity prevalence by definition. While several studies clustered near this average, others reported markedly higher or lower estimates. For example, 26 reported a prevalence of 77.6%, whereas 28 found only 7.1%.
The wide range in reported prevalence of multimorbidity (7.1% to 77.6%) across studies likely reflects substantial heterogeneity in study populations and methodologies. Differences in participant age across studies, for example, some focused exclusively on adults aged 60 and older, where multimorbidity is more common, while others included participants as young as 16, may account for variation in the findings. Additionally, differences in data collection, self- reported or medical records, and the number and type of chronic conditions included in each study’s definition, may have further influenced prevalence estimates.
Prevalence of multimorbidity in Saudi Arabia and global comparisons
This section synthesizes prevalence estimates of multimorbidity reported across the included studies. Using a narrative synthesis approach, findings are compared across diverse population groups, age ranges, and healthcare settings within Saudi Arabia. Global data are also referenced to contextualize national patterns. Figure 5 maps the geographic distribution of multimorbidity studies across Saudi Arabia. It reveals a concentration of research in urban areas like Riyadh, Jeddah, and Mecca, while smaller cities and rural areas remain largely under-represented. Geographic Distribution of Multimorbidity Studies Across Saudi Arabia Regions. Note: the map shows that 12 studies were conducted in specific cities, while an additional 5 studies covered the entire country.
The prevalence of multimorbidity in Saudi Arabia varies widely across studies. The lowest number of identified multimorbidity cases was reported by 17 who found 40/130 cases (30.7%) among human immunodeficiency virus (HIV) positive patients in Jeddah. Slightly higher, 18 identified 41/500 cases (8.2%) among adults in Al-Jouf. In another study 19 found 79/767 cases (10.3%) having two or more diseases along with inflammatory bowel disease (IBD). However, 184/767 cases (23.9%) of these patients had one chronic disease along with IBD in Jeddah.
Moderate case counts were reported in several studies. 20 identified 71/387 (18.3%) individuals with multimorbidity among adults in Qassim. Moreover, 22 reported 102/343 (29.7%) cases among elderly participants in Dammam city, based on identifying individuals with “three or more chronic conditions”. In Riyadh, 23 found 127/381 (33.3%) individuals with multimorbidity among adults, while 21 in Khamis Mushait, reported that 50/150 (33.33%) patients with rheumatoid arthritis had two or more additional chronic diseases. On the other hand, the highest proportion was observed in a smaller hospital-based study by 26 in which 248/319 (77.6%) elderly (65+) participants in Riyadh had multimorbidity. 24 reported 160/324 (49.4%) adults aged 50 years and older in Riyadh have multimorbidity. Lastly, a study by 25 reported all samples of 176 patients had kidney disease in addition to either diabetes mellitus, hypertension, dyslipidemia, or thyroid disorders.
Larger numbers of individuals with multimorbidity were observed in broader community-based and national samples. 27 identified 253/700 (36.1%) adults in Riyadh with multi morbidity and 33 reported 540/1853 (29.2%) hospitalized adult patients with COVID-19 in Khamis Mushait had multi morbidity. At the national level,, 28 using pooled national survey data, 564/7317 (7.1%) adults had multimorbidity. 29 in a nationwide sample of elderly individuals aged 60 and above, recorded 1405/2702 (52%). Among the largest datasets, 30 identified 5379/23,098 (23.3%) participants had multimorbidity, while 31 in a descriptive record-based study of adults aged 60 and older, found 51,962/193,715 (26.8%) individuals who had both diabetes mellitus and hypertension. The highest absolute number of cases was reported in the national study by, 32 which included a massive sample of 271,398/650,835 (26.7%) adults representing a large number of the total sample.
International comparisons also reveal wide similarities. A study in Kuwait, 34 indicates the prevalence of multimorbidity reported as 979/3572 (27.4%), similar to most studies in Saudi Arabia, with some studies like 30 with (23.3%). Similarly, Qatar’s 35 prevalence of multimorbidity at 175,032/796,427 (22.1%) is slightly lower than Saudi Arabia’s national-level estimate of 26.7% reported by 32 (n=650,835). In contrast, India 36 reported a much lower prevalence of 51,322/712,822 (7.2%) among individuals aged 15 to 49. This finding underscores the need for a comparative investigation into the shared risk factors contributing to multimorbidity in both Saudi Arabia and Qatar. Moreover, Australia, 37 with a reported prevalence of 2839/8707 (32.6%), and Canada 38 with 18,319/82,508 (22.2%) among adults aged 35+, also rates that align with several mid-range Saudi studies such as 31 (26.8%) and 30 (23.3%). In The United States, 39 reporting 27.2% prevalence in 2018 (approx. 68 million people), and Germany, 40 reporting 7638/19,294 (39.6%), are comparable to findings in large-scale Saudi samples such as 30 (23.3%) and 32 (26.7%).
Across Asia, multimorbidity remains an issue. For instance, Indonesia 41 3369/9438 (35.7%) and Malaysia 42 5157/18,101 (28.5%) report prevalence levels comparable to many Saudi studies. Thailand 43 2927/14,353 (20.4%) and Bangladesh 44 319/566 (56.4%) among elderly. Notably, Japan 45 1121/2525 (44.4%) in older adults, and South Korea 46 233/1704 (13.7%) among shift workers also align with several mid-range Saudi studies. Vietnam, 47 with only 756/19,380 (3.9%) prevalence in adults aged 25–64, somewhere aligned with the lowest Saudi estimate 28 of 7.1%.
Despite the rising burden of multimorbidity in many countries worldwide, there remains a lack of comprehensive global public health interventions. This growing challenge underscores the urgent need for effective action. The variation in multimorbidity prevalence across Saudi Arabia and globally suggests that the burden of chronic diseases is on the rise. These findings underscore that Saudi Arabia is not an outlier, but part of a broader global shift in this public health concern.
Common chronic disease clusters among individuals with multimorbidity
This section synthesizes findings from the included studies regarding the most frequently reported chronic conditions among individuals with multimorbidity in Saudi Arabia. A narrative synthesis approach was used to compare patterns across studies and highlight recurring disease combinations. Global evidence is also included to compare Saudi-specific findings with international trends and provide broader context. Figure 1 visualizes the reporting frequency of specific chronic diseases across the included studies. It highlights that diabetes and hypertension were the most widely reported conditions in all five studies, while other conditions such as cancer, dementia, and thyroid disorders were only moderately or rarely addressed. Understanding multimorbidity patterns in Saudi Arabia is crucial, as it helps identify which chronic diseases tend to occur together and offers insight into the healthcare providers with these clusters.
Among the 17 studies included in this review, only five specifically addressed the most common chronic conditions among individuals with multimorbidity or comorbidity in Saudi Arabia.17,19,21,24,33 Notably, all five studies obtained their data from cross-sectional, retrospective study, and/or medical records, enhancing the credibility of the findings related to chronic disease patterns among individuals with multimorbidity. Diabetes mellitus (DM) was mentioned in all five of the Saudi studies and was ranked as the most common chronic condition in three of the studies. For instance, among HIV patients in Jeddah DM where the most common comorbidity effects 20/130 (15.4%) of cases, 17 among hospitalized COVID-19 patients in Khamis Mushait with a rate of 899/1853 (48.5%), 33 among IBD patients in Jeddah, DM was reported in 26/79 (32.9%) patients identified as multimorbid of that subgroup. 19 These findings are consistent with global patterns. In Qatar, diabetes was part of the most common multimorbidity dyad [DM + hypertension at 6525/1,75,170 (3.7%)] and triad [DM + hypertension + dyslipidemia at 9704/1,75,170 (5.5%)]. 35 Similarly, a Bangladesh study revealed that 147/156 (95.2%) of people with diabetes had multimorbidity, underscoring its central role in chronic disease clusters. 44 Following diabetes, hypertension (HTN) was frequently reported. One Saudi study from Hail identified HTN as the most prevalent condition among patients with chronic kidney disease 101/176 (57.4%), exceeding diabetes at 66/176 (37.5%). 25 Moreover, hypertension ranked as the second most prevalent condition among multimorbid patients in Jeddah 17 14/130 (10.8%) and 15 19/79 (24.1%), as well as in Khamis Mushait 24 232/1853 (12.5%) and 19 49/150 (32.7%), respectively.
This trend reflects international observations, for instance, in India, HTN was involved in the most common dyads (HTN + obesity at 2.9%) and triads (DM + HTN + obesity at 0.4%). 36 In Indonesia, HTN was a key component in clusters with cardiac disease, hypercholesterolemia, for both men and women. 41 In Australia, the most common disease combination was HTN + hyperlipidemia 720/8707 (8.3%), followed by HTN + hyperlipidemia + osteoarthritis 287/8707 (3.3%). 37 Anemia emerged as the most reported condition in one Saudi study among rheumatoid arthritis patients in Khamis Mushait, with a prevalence of 73/150 (48.7%). 21 This finding aligns with India, where anemia was also part of a common dyad with hypertension (HTN + anemia at 2.2%). 36 Dyslipidemia, while not the most dominant condition in Saudi data, still appeared frequently. It ranked second in Jeddah 14/130 (10.8%), 17 third in Khamis Mushait 40/150 (27.3%), 21 and was reported at a lower rate in Hail 5/176 (2.8%). 25 This mirrors global findings, such as in Australia, where hyperlipidemia was among the most common comorbidities, particularly in combination with HTN and osteoarthritis. 37 Other chronic conditions such as osteoporosis, chronic kidney disease, and respiratory or neurological disorders were noted in Saudi studies but occurred less frequently.
One noteworthy gap in Saudi research was the underrepresentation of mental health conditions. Only one study reported depression 7/130 (5.4%) among HIV patients in Jeddah. 17 This underreporting aligns with the global literature, where psychological comorbidities are often overlooked in multimorbidity research, despite their significant impact on overall health outcomes. These findings reinforce the global consistency of diabetes, hypertension, and dyslipidemia as core components of multimorbidity. Their repeated appearance across different populations underscores the importance of investigating the underlying reasons for this clustering and developing integrated approaches to address them collectively. These comparative insights offer a foundation for designing context-specific interventions aimed at managing multimorbidity more effectively.
Descriptive profile of included studies in Table 4
Gender differences in multimorbidity prevalence.

Note. Studies are arranged in ascending order according to the number of participants identified with multimorbidity (n).
Gender differences in multimorbidity patterns in Saudi Arabia and global contexts
This section presents a narrative synthesis of gender-related differences in multimorbidity prevalence reported across the included studies. The findings highlight how multimorbidity manifests differently in men and women within the Saudi population, with international literature used to support comparative insights. As shown in Figure 2, females consistently exhibited higher prevalence rates of multimorbidity across most study years. Figure 4 illustrates gender-based variations in multimorbidity prevalence. Most studies reported a higher prevalence among females, with notable differences in 19 and. 24 However, exceptions exist, such as, 17 where male prevalence exceeded female prevalence.
Gender disparities in multimorbidity have been widely documented across diverse populations. In Saudi Arabia, multiple studies indicate that women tend to report higher multimorbidity prevalence than men, particularly in older age groups. For instance, elderly adults aged ≥50 years in Riyadh (n= 324), 95/160 cases (59.4%) were women and 65/160 cases (40.6%) were men who experienced multimorbidity; here, the denominator (160) represents the total number of participants identified with multimorbidity, including both genders, rather than gender-specific subgroup sizes or the overall. 24 Another study observed that among elderly adults aged ≥65 years in Riyadh (n = 319), 121/152 cases (79.6%) were women and 127/167 cases (76.0%) were men who had multimorbidity; here, the denominators (152 for women and 167 for men) represent the total number of participants in each gender subgroup within the study sample. 26 Also, a study conducted (n = 767) found that among the 79 patients with multimorbidity, 51/79 cases (64.6%) were female and 28/79 cases (35.4%) were male; here, the denominator (79) represents the total number of participants diagnosed with morbidity, including both genders, rather than gender-specific sizes and the overall sample size. 19
National data covering a large elderly population aged ≥60 years (n = 193,715) showed a narrower difference, yet still reflected a greater burden among females, with 27,602/99,829 cases (27.6%) compared to 24,360/93,886 cases (25.9%) among males; here, denominators (99,829 for women and 93,886 for men) represent the total number of individuals in each gender group within the overall study sample. 31 Lastly, a regional study from the Qassim region (n = 387) revealed that women exhibited a higher prevalence of multimorbidity, with 33/387 cases (8.5%) compared to 27/387 cases (7.0%) among men; here, the denominator (387) represents the total study sample, and not gender-specific subgroup sizes. 20
This pattern aligns with global evidence showing that women consistently experience a higher burden of multimorbidity than men. In China, pooled data from 28 studies among older adults aged ≥60 years reported a prevalence of 37.6% among women and 33.4% among men. 48 In South Korea (n = 30,138), the prevalence of multimorbidity accompanied by depressive symptoms was 3824/17,840 cases (21.4%) among women and 1425/12,298 cases (11.6%) among men; here, denominators (17,840 for women and 12,298 for men) represent the total number of participants in each gender group within the overall sample. 49
Supporting evidence from Europe further reinforces these trends. A population-based study conducted in Spain among older adults (n = 72,815) demonstrated notable gender differences in multimorbidity patterns. Women were more likely to exhibit mechanical patterns (33.3%) and psychogeriatric patterns, while men predominantly presented with cardiometabolic patterns (21.2%). 50 Similarly, in Denmark, women were found to have a higher overall prevalence of multimorbidity, with 171,165/720,885 cases (24%), compared to 130,592/676,288 cases (19%) in men; here, denominators (720,885 for women and 676,288 for men) represent the total number of individuals in each gender group within the overall sample. 51 A nationally representative study in Saudi Arabia (n = 23,098) found that the prevalence of multimorbidity was nearly similar between men, with 2716/11,433 cases (23.8%), and women, with 2663/11,665 cases (22.8%), among adults aged ≥18 years; here, denominators (11,433 for men and 11,665 for women) represent the total number of participants in each gender group within the overall sample. 30 Comparable findings were reported in a French population-based study (two large nationwide surveys) HSM (n=23,348) and ESPS (n=14,875) surveys, which observed minimal gender differences in multimorbidity among younger age groups. These differences became more evident with advancing age, particularly beyond the age of 60. 52 Despite differences in gender-specific prevalence, both the Saudi Arabian and French studies used large, nationally representative surveys to assess multimorbidity prevalence among adults, and they revealed a high prevalence of multimorbidity among both men and women.
On the other hand, some Saudi-based findings among HIV patients (n = 130) demonstrated a higher prevalence of multimorbidity among males, with 48/93 cases (51.6%), and among females, with 15/37 cases (40.5%), having at least one chronic comorbidity in a tertiary care setting; here, denominators (93 for males and 37 for females) represent the total number of individuals in each gender group within the overall sample. 17 This is likely due to the influence of HIV-related factors, as HIV infection can accelerate the onset of chronic conditions through mechanisms such as persistent inflammation, immune system dysregulation, and treatment- related complications. 53 While this observation contrasts with the broader global trend, where females, particularly in older age groups, are generally more likely to experience multiple chronic conditions, it highlights the importance of interpreting gender-based differences in multimorbidity within the specific clinical and demographic characteristics of each setting.
Syndemic theory (ST)
The clustering of multiple chronic conditions observed in this review can be meaningfully interpreted through the lens of syndemic theory (ST), a framework that reshapes how we understand co-occurring health problems. As described by Singer in 1996 “In other words, a syndemic is a set of closely intertwined and mutual enhancing health problems that significantly affect the overall health status of a population within the context of a perpetuating configuration of noxious social conditions.”. 54 In light of syndemic theory, the frequent clustering of conditions such as diabetes, hypertension, and dyslipidemia particularly among women in this review aligns with the theory’s core premise: that diseases do not occur independently but co-occur and interact within adverse social and environmental conditions.
The elevated prevalence of multimorbidity among females is not solely biological, while hormonal changes during peri- and post menopause may increase the risk of metabolic conditions, 55 exposures to behavioral and environmental factors play a critical role in this matter. Behavioral risk factors are highly prevalent among Saudi women, women in Saudi Arabia, especially those working in office-based jobs, experience higher rates of obesity and physical inactivity. 56 Moreover, the prevalence of overweight and obesity among women is 54%, with 82% not meeting physical activity recommendations, and only 7% consuming the recommended servings of fruits and vegetables. 57 These behavioral risks are further compounded by socioeconomic inequalities. A recent national analysis showed that the prevalence of NCDs is highest among women with lower income and education levels, with significant regional variations. Gender analysis revealed that both income and education-based concentration were significantly negative among women, indicating that NCDs are concentrated among women with lower income and education levels. 58 Low socioeconomic status (SES) also shapes perceptions and behaviors related to health. Individuals in low-SES groups are more concerned about the cost of healthy behaviors and are often more motivated to change only after the onset of disease, rather than as a preventive measure. 59 Mental health represents another critical axis of health burden in women. In Saudi Arabia, anxiety and mood disorders are disproportionately higher among females, and these conditions are influenced by both chronic disease and gendered stressors such as domestic violence and polygamy (having several spouses). 60 The interaction of these factors may raise the likelihood of developing metabolic diseases.
Moreover, life expectancy plays an important role among women. World Health Organization life-table data for Saudi Arabia shows a clear longevity edge for women: females born today are expected to live slightly beyond 76 years, whereas their male counterparts are projected to live just under 74 years. 9 Women with chronic conditions report significantly lower health-related quality of life (HRQoL), both physically and mentally. This burden is especially pronounced among women with lower education levels. 61 In parallel, a study conducted in 2023 among low-income women in Saudi Arabia found that women’s definition of a healthy lifestyle included not only diet and exercise but also mental well-being. However, maintaining such a lifestyle was not always feasible due to high costs, lack of availability, and time constraints. Family support and the desire to prevent or manage disease were identified as key motivators, while ideal interventions were described as structured, supportive, and sensitive to women’s lived realities. 62
These conditions do not merely co-occur with disease, they intensify it. By interpreting our findings through a syndemic lens, we move beyond reductionist, disease-by-disease models toward a more holistic understanding of multimorbidity as a socially embedded phenomenon. This perspective strengthens the interpretation of how chronic conditions emerge and persist within specific social, gendered, and environmental contexts. This approach also informs public health practice by emphasizing the need for multi-level, integrated strategies that address not only clinical care but also social determinants such as income, education, and gender norms. Syndemic-informed research and intervention planning can better target high-risk groups and develop more effective, equitable health solutions in Saudi Arabia.
Strengths and limitations
This review has several strengths. As the first narrative synthesis focused on multimorbidity in Saudi Arabia, it provides valuable insights into prevalence rates, gender-specific differences, and common chronic conditions. The included studies represent a broad range of population groups, including general adults, older individuals, and patients with specific chronic or infectious conditions. This diversity allows for a more nuanced understanding of multimorbidity patterns across different subgroups. A key methodological strength of this review is the use of the JBI critical appraisal tool to assess the quality of all included studies. This allowed for a structured evaluation of potential biases and enhanced the credibility of the synthesized findings. Moreover, among the five studies that reported specific chronic disease patterns, all relied on medical record data, which enhances the accuracy and credibility of the findings related to disease clustering in individuals with multimorbidity. Additionally, while the review focused exclusively on national studies, comparisons with international literature provide valuable context and underscore both common trends and country-specific patterns in multimorbidity prevalence and disease clustering. Another strength lies in the use of syndemic theory to interpret the clustering of conditions in relation to social and gendered determinants, offering a more holistic understanding of multimorbidity beyond biomedical factors.
Although the findings are promising, several important limitations must be considered. First, the overall number of studies on multimorbidity in Saudi Arabia remains limited, with only 17 studies meeting the inclusion criteria, The overall volume of available research remains limited. This relatively small body of evidence reduces the ability to conduct in-depth synthesis and limits the strength of the conclusions that can be drawn from the review. In addition to the limited number, the included studies varied considerably in scope and design, with inconsistent definitions of multimorbidity across studies, which presents challenges to synthesis. The differences were observed in the targeted population, data collection methods (e.g., self- reported vs. medical records), and limited geographic focus. While such diversity offers a broad perspective, the lack of harmonization across studies compromises comparability and weakens the generalizability of findings. Conceptual gaps were also evident across the included studies. In many cases, multimorbidity was treated as a secondary focus, rather than the primary focus of investigation. As a result, synthesis was often limited in scope, with minimal attention to disease clustering, which in turn constrained the depth of analysis regarding patterns of co-occurring conditions within multimorbid populations. Furthermore, only one study explicitly addressed mental health conditions in the context of multimorbidity. The understudies of mental health significantly limits the comprehensiveness of the current evidence and underestimates the true burden of multimorbidity in the Saudi population. Population and methodological factors also introduced limitations. Although the total sample exceeded 800,000 participants, the majority of studies were based in urban centers such as Riyadh and Jeddah, leading to underrepresentation of rural populations. Additionally, all studies focused on older adults, with no inclusion of individuals younger than 15, potentially skewing prevalence estimates upward and missing early-onset multimorbidity trends. This omission is significant, as it contributes to an overrepresentation of older age groups where multimorbidity is more common, leading to inaccurate estimates of overall prevalence. Methodologically, the majority of studies employed a cross-sectional design, which prevents causal inference and limits the ability to track the temporal progression of disease. A formal screening tool such as PRISMA was not employed in the study selection process. Instead, inclusion and exclusion of studies were guided by a structured approach using predefined eligibility criteria, which may have introduced subjectivity and limited reproducibility. Moreover, a technical limitation lies in the inconsistent reporting of confidence intervals (CIs). Almost none of the studies in this review provided CIs for prevalence estimates, limiting the ability to assess statistical precision or compare findings across subgroups. This absence reduces analytical clarity and makes it difficult to evaluate the robustness of reported estimates. Several studies, particularly those reporting prevalence estimates, relied on self-reported data, which is prone to recall bias, underreporting, and misclassification. This introduces uncertainty in the accuracy of reported multimorbidity rates. A further limitation relates to the international comparisons included in this review. While they offer contextual value, these comparisons were not adjusted for differences in age distributions, multimorbidity definitions (e.g., ≥2 vs. ≥3 conditions), or the number and types of diseases considered. Additionally, variations in healthcare infrastructure, diagnostic criteria, and data collection methods across countries may contribute to differences in reported prevalence. Addressing these limitations in future studies will be critical to informing more effective, evidence-based public health policies targeting multimorbidity prevention and management in Saudi Arabia.
Recommendations
Research priorities
Future research on multimorbidity in Saudi Arabia should move beyond general prevalence estimates and address key evidence gaps. This includes focusing on younger age groups, integrating mental health conditions, and ensuring national representativeness by deliberately sampling from rural villages, peripheral governorates. Priority areas include exploring disease clustering patterns, conducting longitudinal studies to understand causal pathways, and utilizing advanced analytical methods such as latent class analysis applied to large national datasets like the Saudi Health Interview Survey. Future research should clearly define multimorbidity criteria, ensuring consistent measurement of disease count. Incorporating family medical history and investigating personalized medicine approaches may further enhance risk stratification and early detection strategies.
Clinical and practice implications
In clinical practice, findings support transitioning from fragmented, disease-specific care toward integrated, multidisciplinary models tailored to patients with multimorbidity. Particular emphasis should be placed on improving care coordination and continuity, as fragmented services can undermine the quality of care. Multimorbidity’s negative impact on patients’ quality of life reinforces the need for proactive management strategies, especially in primary care settings. Training healthcare providers to manage co-occurring conditions holistically and embedding mental health services within routine care are also critical next steps. Additionally, integrating health educators into clinical teams can play a pivotal role in raising awareness, supporting behavior change, and improving disease self-management among the Saudi population, particularly through culturally relevant education on risk factors, prevention, and early detection.
Policy and system-level recommendations
At the health policy level, there is a need to invest in community-based screening programs to improve early detection, particularly in underserved and rural areas. These programs should be designed to capture both physical and psychological risk factors and linked with follow-up care pathways. Efforts should also include strengthening national health data infrastructure, standardizing disease coding practices, and improving surveillance mechanisms for multimorbidity indicators. These priorities align with Saudi Arabia’s Vision 2030, especially in areas related to expanding primary care services, optimizing resource allocation, and reducing health disparities. 63 Implementation Strategies to ensure real-world applicability, future interventions should adopt structured implementation frameworks such as CFIR and RE-AIM.64,65 These models offer practical tools to navigate the complexities of real-world settings. Embedding these models into program design and evaluation will enhance intervention uptake, scalability, and impact.
Equity and gender-responsive approaches
All future efforts should integrate gender-sensitive and equity-driven strategies across research, planning, and service delivery. This includes acknowledging the disproportionate burden of multimorbidity among women. Equity-oriented interventions must also address structural barriers faced by low-income groups and rural populations, ensuring inclusive care delivery and fair access to preventive and treatment services.
Conclusion
This review offers the first focused narrative synthesis of multimorbidity research in Saudi Arabia and highlights key structural and conceptual gaps in the national evidence base. While previous studies have documented prevalence trends, this review uniquely integrates a gender-informed lens and applies syndemic theory to interpret multimorbidity as a socially embedded phenomenon, rather than a coincidental accumulation of diseases in Saudi Arabia.
The findings of this review reveal that multimorbidity in Saudi Arabia has a wide prevalence range (7.1% to 77.6%) depending on study design and population characteristics, and disproportionately affects women and older adults. These insights carry actionable implications. In clinical practice, there is a pressing need to move beyond siloed, disease-specific approaches toward coordinated, multidisciplinary care models tailored to the complex needs of patients with multimorbidity. From a public health policy perspective, the results emphasize the importance of investing in community-based screening initiatives, addressing geographic and gender-based disparities in access to care, and developing robust national data systems. These strategies align with the objectives of Saudi Arabia’s Vision 2030 health reform, particularly the strengthening of primary care, optimization of resource allocation, and enhancement of care continuity. Lastly, a formal quality appraisal was conducted using the JBI tool, which revealed variability in study quality and highlighted the need for more rigorous, standardized methodologies in future research.
Despite these contributions, there were several methodological and conceptual limitations in the current evidence base. Multimorbidity remains underexplored among younger age groups and mental health populations. The majority of included studies were cross-sectional, with only one Cohort-retrospective design. Many studies relied on self-reported data and lacked representation from rural areas. Additionally, confidence intervals for prevalence estimates were not reported in almost all included studies, which restricts statistical interpretation and comparability. These limitations reduce the precision and generalizability of findings and restrict our understanding of how multimorbidity patterns evolve over time, how conditions interact biologically and socially, and how early-onset multimorbidity manifests in underserved populations. Priority research areas include multimorbidity among youth, mental health comorbidities, disease clustering, and harmonization of definitions across studies.
For the research community, the findings highlight the urgent need for longitudinal, theory-driven studies that examine disease clustering, incorporate mental health, and broaden the demographic scope to younger adults. This review provides a timely foundation for advancing both knowledge and policy and calls for a national strategy centered on integrated care, targeted research investment, gender-sensitive interventions that recognize the unique burden of multimorbidity among women.
Footnotes
Ethical considerations
This study is a review based on previously published data and does not involve human participants or new data collection. Therefore, ethical approval is not applicable.
Funding
This research received no funding.
Declaration of conflicting interests
The authors declare no conflict of interest related to this study.
Data Availability Statement
All data included in this review are from publicly available published studies, as cited in the reference list.