
Abstract
Objectives
Demographic and epidemiological shifts have led to people living with coexisting health issues, known as ‘multimorbidity’. Given India’s aging population, rising noncommunicable disease burden, chronic infections, fragmented healthcare, and reliance on specialist care, a scoping review is needed to understand the extent and nature of research on multimorbidity in India.
Methods
A comprehensive search was conducted across PubMed, Cochrane, and Embase for studies focused on multimorbidity, with information specifically from India. Two reviewers independently screened the results and extracted information on definitions, including use of cut-offs or a minimum number of conditions, data and methods, patterns, risk factors and outcomes. Results were synthesized using descriptive statistics and narrative synthesis.
Results
Of 9954 identified studies, 100 were included in the final synthesis. Of these, 62 were secondary analyses, 35 collected primary data, and 3 used administrative data. Most studies defined multimorbidity as two or more chronic or long-term conditions but did not specify whether long-term infections or mental health conditions were included. The number of conditions varied between 4 and 22. Circulatory, endocrine-nutritional-metabolic, and respiratory diseases were most frequently included. Beyond simple disease counts, combinations were reported in 15 studies. Healthcare utilization, out-of-pocket expenditure, and quality of life were commonly studied, mostly using cross-sectional designs.
Conclusion
A standardised panel of conditions with clear definitions is needed for measuring multimorbidity. Conditions should be ascertained through a combination of self-report, physical examinations, and laboratory investigations. Additionally, longitudinal studies focused on multimorbidity, and its outcomes are needed to strengthen evidence base in India.
Keywords
Introduction
India is undergoing an epidemiological transition, with a rising burden of non-communicable diseases (NCDs) and mental health disorders adding to the existing burdens of infectious diseases and malnutrition.1,2 This transition has led to an increasing prevalence of multimorbidity - the simultaneous occurrence of two or more long-term (chronic) conditions in the same individual. Although sometimes used interchangeably, it is important to distinguish multimorbidity from comorbidity, which refers to conditions additional to an index disease, while in multimorbidity no condition is prioritised over any other.3,4 These co-occurring conditions often require complex and regular care. 5 In India, the burden of multimorbidity is estimated to be around 20% among adults. 6 Multimorbidity is influenced by a range of demographic, social, economic, and environmental factors that collectively impact health.7,8
India’s population is aging due to declining fertility rates and increasing life expectancy, leading to rise in major NCDs like cardiovascular diseases, cancers, and diabetes. 9 Simultaneously, unhealthy lifestyle behaviours such as physical inactivity, poor dietary habits, tobacco use, and alcohol consumption are becoming increasingly common, further contributing to the rising NCD burden.10,11 Rapid urbanization and its accompanying issues, such as air pollution, occupational hazards, and environmental exposures, also significantly contribute to the risk of developing multiple chronic conditions.12,13 Moreover, the persistent problems of undernutrition, overnutrition, and micronutrient deficiencies augment an individual’s susceptibility to multiple long-term conditions.14,15 Mental health conditions like depression and anxiety often co-occur with other chronic diseases, adding to the challenges. 16 Lastly, the interactions between NCDs and chronic infections, such as human immunodeficiency virus and tuberculosis, are complex and bi-directional and have health system implications. 17 While disease burden has historically been viewed as an issue primarily affecting older adults, existing evidence indicates its growing prevalence across all age groups in India, including younger populations.18,19 This imposes an enormous burden in terms of health and economic impacts, 20 including reduced quality of life,21,22 increased healthcare utilization23–26 and out-of-pocket costs, 20 loss of productivity due to frailty, 27 functional limitations 22 and higher mortality risks. 28 With India’s limited resources and strained healthcare system, 29 the rising multimorbidity presents a formidable public health challenge that demands urgent attention and effective prevention and management strategies.
Despite the increasing recognition of multimorbidity as a major health priority, research in this area, although rapidly expanding, is still in a relatively nascent stage, particularly within the Indian context. A key challenge hindering progress is the lack of standardization and consensus on definition, measurement approaches, and analysis methods employed across different studies. This heterogeneity considerably complicates efforts to synthesize findings, estimate the true burden accurately, and develop a comprehensive understanding of multimorbidity.
While international reviews on multimorbidity have provided some insights,8,30 and some reviews have focussed on low-and-middle income countries (LMICs). The unique challenges posed by India’s disease burden and healthcare context warrant a dedicated review addressing these issues. The range of diseases in India differs from those in high-income countries due to the coexistence of chronic infections and NCDs. India’s fragmented healthcare system increases care challenges for multimorbid individuals, and uneven access to care compounds the problem. The type of routine data used in most multimorbidity studies in other countries does not exist in India, emphasizing the need to identify other available data sources. Though these challenges may be common among LMICs, extent of the problem will vary depending on the stage of multimorbidity research and data maturity in the country. Also, the systematic reviews that have examined multimorbidity in LMICs30–36 have focused on burden estimates and patterns of occurrence. However, they do not include details about types of conditions included the rationale behind inclusion and exclusion of conditions, how conditions were defined or measured, and data sources used. Some studies have examined the burden, risk factors, and consequences of multimorbidity in India.6,37 However, a comprehensive review of how multimorbidity is defined, measured, and analysed in research in India remains lacking. Furthermore, none of these studies report potential limitations and gaps in multimorbidity research within the context of India.
Through this scoping review, we aim to map the current landscape of multimorbidity research in India. Specifically, we aim to understand a) how multimorbidity has been defined and operationalized, including the conditions included and the rationale, b) the data sources and sample sizes used, c) the populations studied, d) the methods employed to quantify or describe multimorbidity, and e) how individuals with multimorbidity have been characterized in terms of burden, risk factors, and outcomes. This can guide future research efforts, which can lead to the adoption of a standardized methodology for the classification of multimorbidity. While the scoping review is based on India, the findings may be applicable for other LMICs and for subpopulations in high-income countries.
Methods
Protocol and standards
A methodological framework adapted from the guidelines developed by Arksey and O'Malley, 38 and further refined by Levac et al. 39 and Peters et al. 40 was followed. Details of methods followed for the scoping review are available in the published protocol. 41 The study was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (Supplemental Table S1).
Identifying relevant studies
Eligibility criteria.

A comprehensive and systematic literature search was conducted across three major databases - PubMed/Medline, EMBASE (Ovid), and Cochrane Library (Ovid) on September 12, 2023. The search strategy incorporated both Medical Subject Headings (MeSH) terms as well as free-text keywords to ensure a thorough search process. A secondary identification of relevant literature was done from the reference list of the selected full text articles using Citationchaser. 43 Supplemental Table S2 presents the search strategy for each database.
Screening and selecting evidence
The identified records were consolidated and managed using the citation management software EndNote 20. 44 Duplicate records were removed through a meticulous de-duplication process within EndNote. The remaining unique records were then imported into Covidence, 45 a web-based platform designed for systematic literature reviews. Covidence facilitated independent screening by multiple reviewers and provided a mechanism for resolving any disagreements during the screening process. 45
The screening process involved two stages. In the first stage, the titles and abstracts of the records were reviewed against the predefined inclusion and exclusion criteria (Table 1). In the second stage, the full texts of the articles included after the first stage were reviewed against the same criteria. Two reviewers (SG and PP) independently assessed each record in both stages, and any disagreements were resolved through discussion with a third reviewer (AG). The entire screening strategy, including the number of articles included or excluded at each stage are presented as a PRISMA flow diagram (Figure 1). A list of studies excluded after full text screening is presented in Supplemental Table S3. PRISMA flow diagram of the study selection process.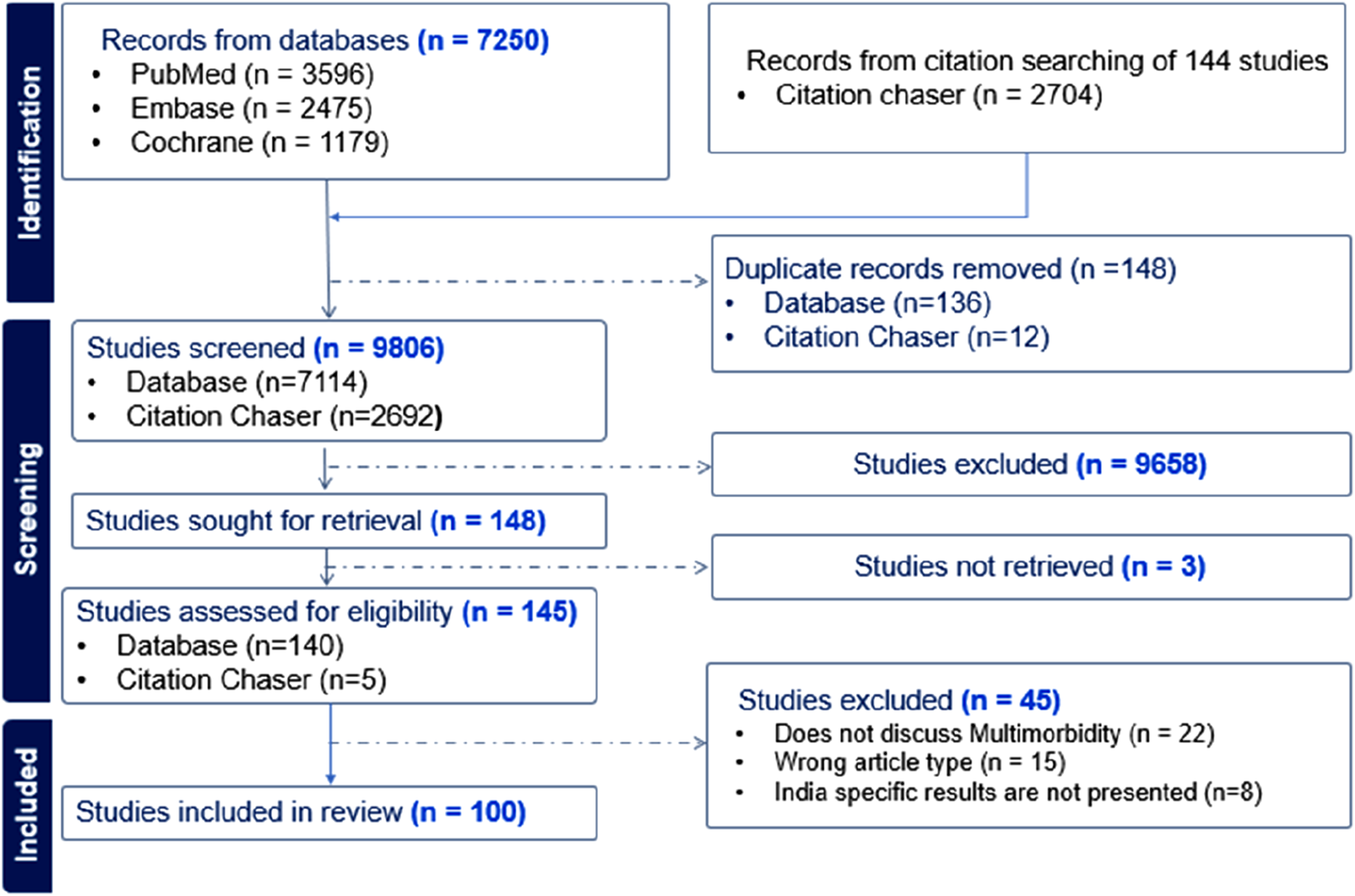
Data charting
A structured data charting tool was developed in Microsoft Excel to ensure a systematic and organized data extraction process. The form was designed to capture various study details, such as year, geographical location, characteristics of populations studied, the definitions and measures used for multimorbidity, methods employed to quantify or describe multimorbidity, observed disease profiles, and risk factors and outcomes in relation to multimorbidity. Details of the data charting tool and identified domains, along with the data items, are presented in the published study protocol. 41
Data synthesis
A descriptive summary of the findings is presented. Diseases included in the identified studies were mapped to body systems using the 11th revision of the International Classification of Diseases (ICD-11) coding (mapping is presented in Supplemental Table S4). 46 Narrative synthesis was used to summarize information on frequently occurring disease profiles, risk factors, and outcomes linked to multimorbidity and potential limitations reported in the studies. 47
Patient and public involvement
Patients or the public were not involved in the design, conduct, or reporting of this study.
Results
Search results
Figure 1 shows the PRISMA flow diagram summarizing the study selection process. Our search identified 9954 studies from databases (n=7250) and citation searching (n=2704). After removing duplicates (n=148), 9806 studies were screened. After screening the title and abstract, 148 studies were sought for retrieval and 145 were assessed for full text screening. Based on full-text screening, 100 studies were included for final synthesis.
Characteristics of the included studies
Characteristics of the included studies.

Note. 1) ASIAN-HF: Asian Sudden Cardiac Death in Heart Failure; LASI: Longitudinal Ageing Study in India; NFHS: National Family Health Survey; NSS: National Sample Survey; RHTC: Rural Health Training Centre; WHO SAGE: World Health Organization- Study on Global AGEing and Adult Health; WHS: World Health Survey 2) NS: Not Specified.
Definition, measurement, and description of multimorbidity
Definition
Definitions of multimorbidity used in the selected studies.
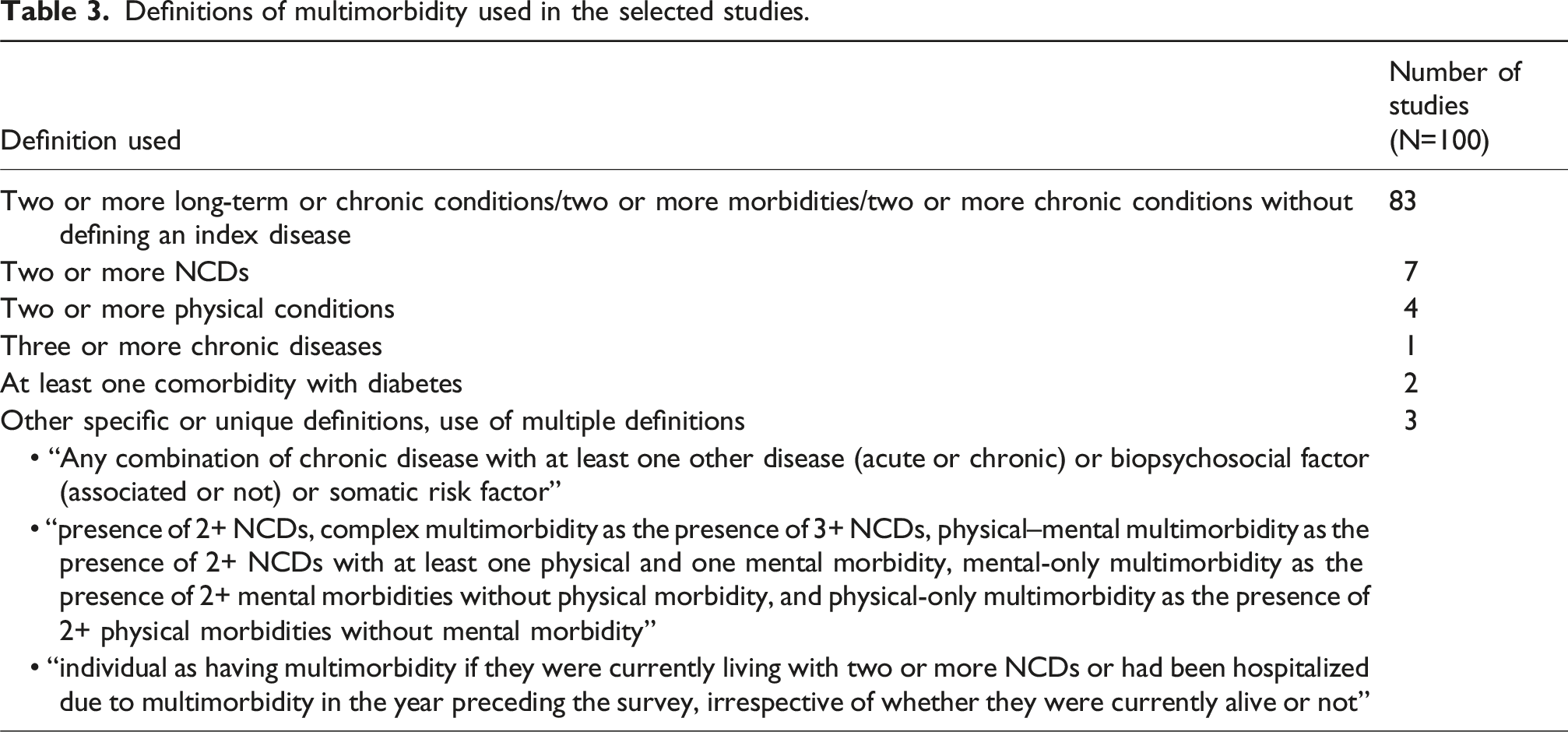
Two studies defined multimorbidity as one or more comorbidities with a specified index condition, diabetes.67,89 Three studies employed specific or unique definitions or used multiple definitions of multimorbidity.
Measurement
The number of conditions used to measure multimorbidity in each study is presented in Table 1. On an average, 12 conditions were used, with a minimum of 4 133 and a maximum of 22 131 conditions across different body systems. Diseases included in each study are listed in Supplemental Table S5. Only three studies used validated tools for assessment of multimorbidity – multimorbidity assessment questionnaire for primary care (MAQ-PC)74,83 and multimorbidity assessment questionnaire for psychiatric care (MAQ-PsyC), 86 where physical morbidities were self-reported doctor-diagnoses that were validated using patient prescriptions and medicine wrappers and psychiatric morbidities were diagnosed by psychiatrist.
Figure 2 shows how often a body system (mapping of diseases to body systems is presented Supplemental Table S4) was included while measuring multimorbidity in these studies. Circulatory diseases, endocrine, nutritional, or metabolic diseases and respiratory diseases were present in more than 80% of the studies. Musculoskeletal or connective tissue disorders, neoplasms, and diseases of the nervous system were less common, occurring in 60-80% of the studies. Mental, behavioural, or neurodevelopmental disorders were included in more than half of the studies, and infectious or parasitic diseases in 21% of them. Conditions related to the eye, ear and skin were present in 50%, 30% and 23% of the studies, respectively. Body systems captured in the selected studies.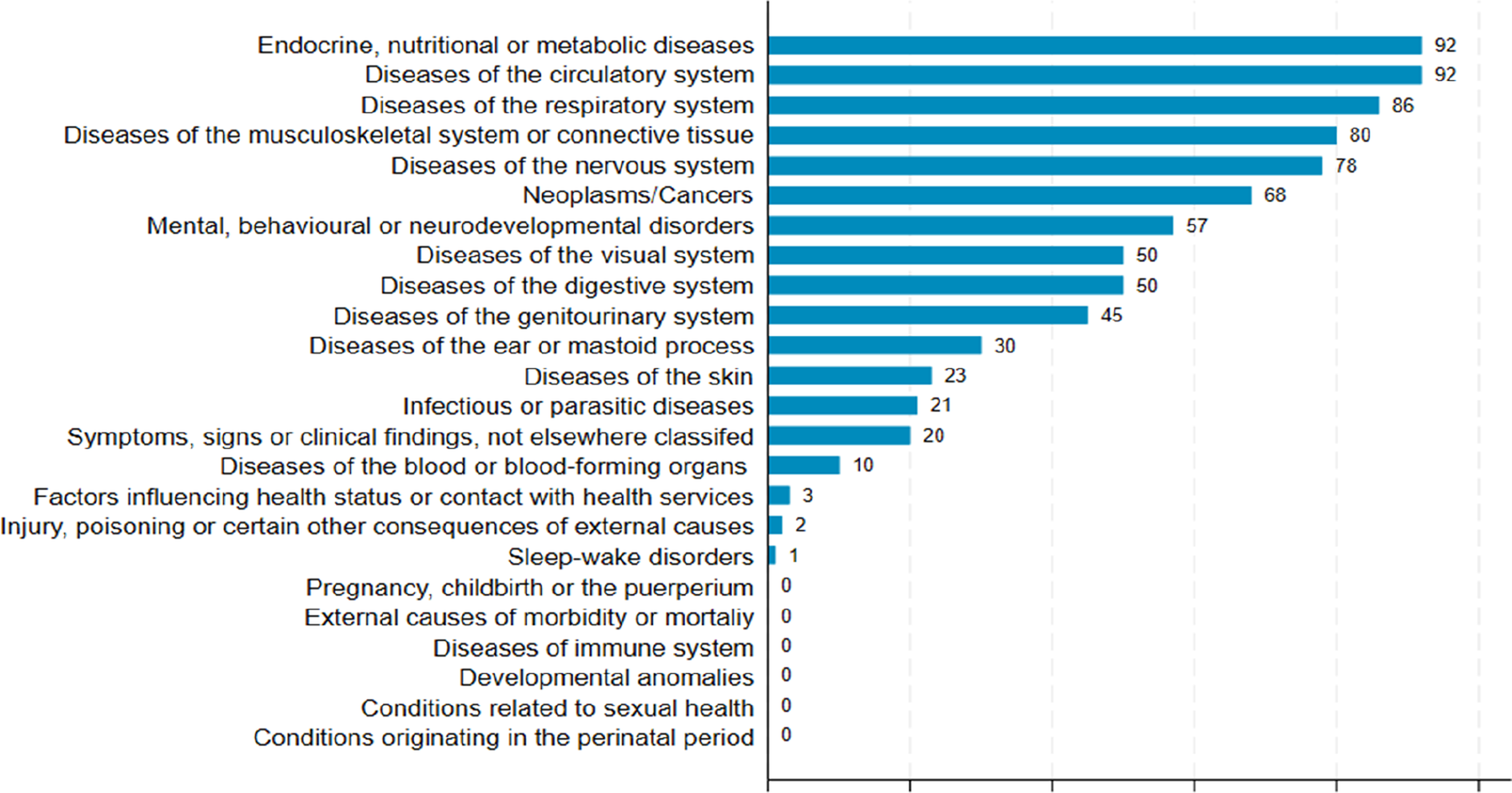
Description
Multimorbidity was quantified using a simple count measure in 85 studies, either as a binary variable (present/absent) or as a categorical variable (none, exactly one condition and two or more). Notably, Gupta et al. (2022) also employed a multimorbidity-weighted index along with a disease count in their study.101,140
In addition to simple counts, disease combinations were described in 15 studies. Two studies presented the commonly occurring two-disease (dyad) combinations,95,137 six studies reported both two-disease and three-disease (triad) combinations,65,70,95,118,128,129 3 studies used latent class analysis48,72,132 to partition participants into groups of multimorbid people with different disease profiles and one study used non-hierarchical clustering to identify disease clusters 136 and 3 studies used a combination of these methods.74,101,113
In the 15 studies reporting disease combinations, various disease combinations and clusters were reported. The most recurrent patterns were ‘hypertension-diabetes’ (9 studies)’,72,95,101,107,113,118,128,129,137 and ‘hypertension-musculoskeletal disorder’, including arthritis and back pain (7 studies).65,101,107,113,128,129,141 Other patterns identified were cardiometabolic-mental disorders136,137 and neurotic-cardiometabolic disorders. 136
Few studies have explored age- and sex-specific differences in multimorbidity burden.65,96,134 Multimorbidity studies covering vulnerable subgroups are limited, but some have examined multimorbidity burden and patterns in population subgroups, including individuals affected with HIV, 64 those with psychiatric problems, 136 pregnant women attending antenatal clinics, 108 aboriginal population 20 and the urban poor. 118
Factors associated with multimorbidity
Summary of risk factors and outcomes studied in identified studies.
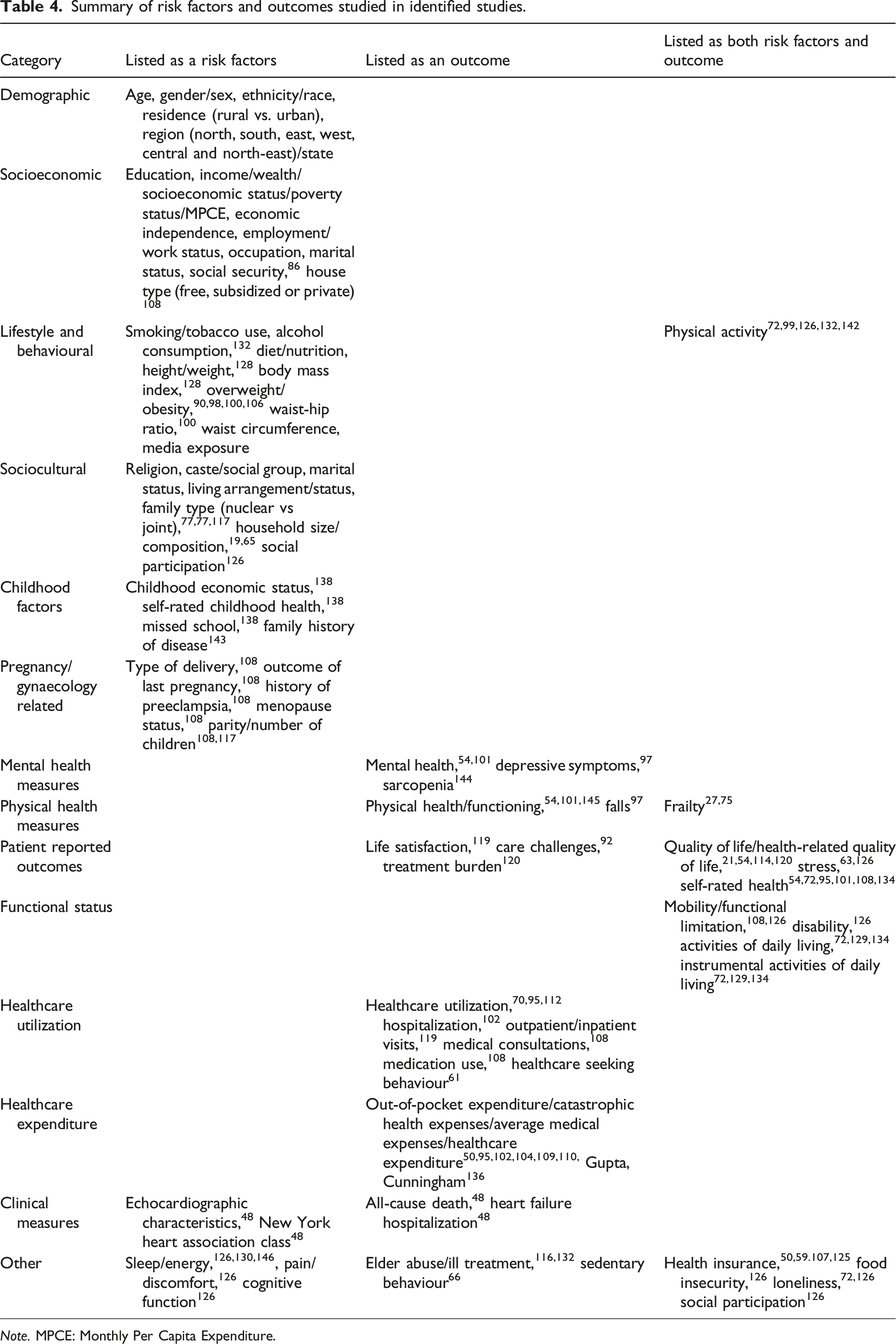
Note. MPCE: Monthly Per Capita Expenditure.
Several factors such as frailty, quality of life, stress, self-rated health, mobility/functional limitation, disability, activities of daily living, instrumental activities of daily living, functional limitations, health insurance, food insecurity and loneliness have been studied both as correlates and outcomes due to their bidirectional relationship with multimorbidity.
Limitations and potential research gaps
First, all but one of the 100 studies were cross-sectional, preventing the study of multimorbidity trajectories and its effect. Second, multimorbidity measurement was limited to a handful of conditions, often leaving out chronic infections. Although two studies developed much-needed tools for multimorbidity measurement, these tools may have limited generalizability across different populations and may not fully capture the complexity of multimorbidity in various settings. Third, data on diseases were predominantly self-reported and therefore prone to recall bias. Studies rarely utilized medical reports, prescriptions, and laboratory investigations to substantiate reported diagnoses. Routinely collected data such as hospital medical records, insurance data and disease registries were seldom used.
Fourth, there was limited detail available on sequence, duration, and severity of conditions and these were not accounted for in the measurement of multimorbidity. Fifth, multimorbid individuals were often studied as a single group and described using a simple disease count. Only a few studies have explored the heterogeneity among them in terms of different disease profiles. Sixth, most studies lacked a conceptual framework for multimorbidity and its correlates, relying solely on available data to explore these relationships. Consequently, important outcomes such as care challenges, polypharmacy, and treatment burden remain understudied. Seventh, the primary studies were often restricted to specific states or regions, with limited generalizability. Furthermore, selection biases were a concern, particularly in facility-based studies. Patients seeking care at these facilities often have complex conditions, which may lead to an overestimation of the multimorbidity burden. This can result in an inaccurate representation of the prevalence and patterns of multimorbidity in the community. Finally, the identification and interpretation of multimorbidity profiles based on data-driven techniques like latent class analysis could have led to misclassification biases and subjectivity in labelling disease patterns.
Discussion
Summary of evidence
This scoping review, based on 100 studies, comprehensively synthesizes existing research on multimorbidity in India. It focuses on how multimorbidity has been defined, measured, analysed and described. Additionally, it seeks to identify potential gaps in the current evidence base, contributing to a more nuanced understanding of the complexities associated with conducting multimorbidity research in India.
This study highlights variations in the way multimorbidity is defined, operationalised and studied in the existing literature. These variations include definitions, the type and number of conditions used in measurement, data sources, study settings, sample sizes, populations studied, methods employed to quantify or describe multimorbidity, and factors studied in relation to it.
While most studies used “two or more long-term or chronic conditions” to define multimorbidity, few of them did not specify ‘long-term’ or ‘chronic’ and most did not explicitly state whether long-term infections or mental health conditions were included. Similar inconsistencies have been reported by other review studies.147,148,30 Ho et al. noted in their review that more than a third of the studies did not report a definition. 30 Other reviews pointed out that while most studies adopted the “two or more conditions” criterion, some specified use of “two or more non-communicable diseases” or “two or more physical conditions,” clearly excluding infectious diseases and mental health conditions from the measurement of multimorbidity.32,34
The number of conditions included in multimorbidity measurement varied widely, averaging 12, with a range of 4 to 22. Varanasi et al. noted in their review that that primary studies designed to examine multimorbidity included more conditions than those using secondary data, which opportunistically used the data to glean information about multimorbidity. 6 Ofori-Asenso et al. suggested that 11 to 74 conditions are needed to reliably estimate multimorbidity prevalence in a population, 148 while Pati et al. recommended including at least 20 conditions. 149 Ho et al. reported that the number of conditions included in multimorbidity measures showed large variation, ranging from 2 to 285, with a median of 17 and an interquartile range of 11-23. 30
There is no consensus on which diseases should be included in multimorbidity assessment. In the Indian context, there are no validated tools for assessing multimorbidity, except for the MAQ-PC. Without standardized tools, studies use different disease lists and definitions, leading to considerable variation in the measurement approaches and resulting in widely varying multimorbidity prevalence estimates. This makes comparisons across populations or over time difficult. Furthermore, current tools may overlook conditions relevant to the Indian population. We found that conditions related to sexual and reproductive health, developmental anomalies and conditions related to the immune system did not appear in any of the reviewed studies. Similar findings were reported by Ho et al. 30 and Varanasi et al., 6 who also noted limited inclusion of reproductive or developmental conditions.
Studies rarely provided a rationale for including or excluding conditions. Rajoo et al. noted that the eight articles they reviewed varied in the way the chronic diseases were selected and that only two had reported the selection criteria for the chronic diseases. 32 To assess the selection of conditions in studies, Ho et al. examined how often conditions from the Global Burden of Disease Study 2019 with high disability-adjusted life years and years of life lost were included in multimorbidity measurement. While they argued that there is no reason in principle to exclude any condition, rare or otherwise, they acknowledged the practical challenge of gathering information on rare conditions. 30 In contrast, Zhang et al. suggested that the inclusion of conditions should be based on their prevalence in the study population, while Pati et al. recommended using prevalence and/or clinical relevance as the criteria for selection.31,149 Additionally, it is unclear whether to count conditions separately (eg, myocardial infarction or angina) or to group them together (eg, coronary artery disease) in multimorbidity measurement. 149 In self-report studies, broad categories are often preferred as respondents may find them easier to report. 30 Busija et al. recommended the use of three- or four-digit ICD-11 codes. 36
The method of ascertaining the presence or absence of conditions also contributed to the variation in multimorbidity measurement. Most studies relied on self-reported physician’s diagnoses. 30 Rarely studies included physician’s assessments, clinical examination, and laboratory and imaging investigations to ascertain the presence or absence of conditions. Reliance on self-reported diagnoses alone may result in biased estimates of disease burden 32 — particularly underestimating conditions that are asymptomatic or not well recognized by individuals,34,148 and overestimating conditions with vague or overlapping symptoms. 32 This is especially pronounced for conditions like depression and anxiety that are stigmatised and therefore underdiagnosed and underreported. Such biases are likely to vary systematically across socioeconomic and educational subgroups due to varying levels of healthcare access, health literacy, and diagnostic awareness. 34 These issues may be further compounded by geographical and contextual variations, 148 including rural-urban differences and disparities across age groups, finally affecting the reported prevalence and patterns of multimorbidity. To improve ascertainment, few studies included measurements, and some studies used a symptom-based questionnaire for conditions such as angina and depression. A panel of potential chronic conditions with standardised definitions to guide ascertainment will help address this issue.
Routinely collected data such as hospital medical records and insurance data are not readily available in India; therefore, multimorbidity studies either used survey data or collected primary research data. Of the 100 studies, 62 were secondary analyses based on only 6 surveys, suggesting the paucity of data on multimorbidity in India. Other reviews have noted the lack of nationwide data pertaining to multimorbidity. 6 They have further commented that the primary studies were mostly conducted either in the community setting or among patients attending out-patient department of primary care and have highlighted that very few studies have documented the prevalence of multimorbidity among hospitalized patients. 133
Given the modest sample size and the small number of conditions in most studies, multimorbidity has mostly been described as a disease count. Few studies have identified commonly occurring two- and three-disease combinations, but disease clusters or clusters of multimorbid people have rarely been studied. Varanasi et al. made a similar observation, while noting that that there is at least a shift in the conceptualization of multimorbidity from purely disease count to specific disease combinations or clusters. 6 Use of indices was uncommon among the reviewed studies, with only one study using a multimorbidity-weighted index. In contrast, Ho et al. in their review found that 30% of the studies measured multimorbidity using weighted indices, especially for predicting outcomes. 30 The two patterns, hypertension-diabetes and hypertension-musculoskeletal disorders, were frequently reported. Similar patterns were also reported by Pati et al. 149 and Rajoo et al. 32 This implies that while some replicable disease patterns are reported, geographical contexts and methodological differences, including different statistical approaches to identifying the patterns of associative multimorbidity, can lead to different findings. 32
There is a notable lack of longitudinal studies on multimorbidity in India – of the 100 studies included in the review, only one had follow-up data. Longitudinal data enable us to explore and verify temporal and causal relationships between multimorbidity, its drivers and associated outcomes. It also facilitates the study of disease progression, including the identification of conditions that act as precursors or catalysts in the progressive accumulation of chronic diseases. Longitudinal data enables us to assess the role of early life, age and life events in influencing long-term risk of developing multimorbidity and other related health outcomes. Longitudinal data helps evaluate the effectiveness of interventions and policies over time. This data is essential for informing targeted preventive and management approaches and guiding policy decisions to address the rising burden of multimorbidity in the country.
Although a few studies have examined multimorbidity in vulnerable and underserved populations – such as individuals affected by HIV, those with psychiatric problems, pregnant women, indigenous communities and the urban poor – such studies remain scarce and sporadic. There are several other marginalized populations, including homeless people, sex workers, transgender individuals, and migrants, that are severely underserved by multimorbidity research. They are often excluded entirely or are a tiny fraction of the total sample, limiting the ability to conduct any meaningful, focussed analysis. These vulnerable populations bear a disproportionate burden, both in terms of prevalence and adverse outcomes, because of higher socioeconomic disadvantages, and limited access to quality healthcare. Factors such as stigma, discrimination, adverse childhood experiences, and unstable living conditions further compound their barriers to care, making their health needs more complex. Their exclusion from the existing literature contributes to an evidence gap, hindering effective policy decision-making and resource allocation. Failing to include them in multimorbidity research extends existing health inequities.
Our review identified age, gender, and socioeconomic status (SES) as key determinants of multimorbidity, along with lifestyle, behavioural, and sociocultural factors. These findings align with existing review studies, which show a positive association between age and multimorbidity. For instance, Zhang et al., Ho at al., and Busija et al. have reported that both the number and complexity of multimorbidity profiles increase with age.30,31,36
Gender differences have also been widely reported. Zhang et al. noted that 86% of studies from China and India reported a higher prevalence of multimorbidity among females. 31 In a scoping review on the epidemiology of multimorbidity in LMICs, 41 out of 43 studies identified female sex as a significant risk factor, 34 perhaps due to women’s longer lifespan, increased healthcare utilization and higher probability of reporting conditions. Similar patterns were observed in high-income countries.
SES is another important determinant. A systematic review by Violan et al. found a consistent inverse relationship between multimorbidity and SES, measured through education, deprivation indices, and coverage of health insurance. 147 Multimorbidity is often socially influenced, with a higher burden among socioeconomically disadvantaged groups. 34 However, findings from LMICs are not always consistent. For example, studies from India, South Africa, and Malawi reported higher multimorbidity among the affluent, while the opposite was true for Iran, China, and Brazil. These discrepancies may be due to differences in healthcare access and utilization patterns, leading to higher diagnosis rates among the affluent, or variation in the conditions included in different studies. 34
Implications for research and practice
There is urgent need for standardization in how multimorbidity is measured – how many and which conditions are included and how information on them is gathered. A combination of data-driven and consensus-building approaches may be helpful. These approaches can be used to develop a list of conditions. Such a list can guide both research and clinical practice to identify multimorbid people. Existing tools and lists of conditions can be examined and adapted to align with local context and purpose. Different data sources for studying multimorbidity and the possibility of linkage between datasets need to be explored. Hospital medical records including laboratory investigations, prescriptions, procedures, health insurance and billing data present opportunities for collecting information on multimorbidity. The possibility of accessing and analysing them, along with the technical and regulatory challenges involved, should be explored. The importance of longitudinal data for multimorbidity research cannot be overemphasized. Studying of disease combinations, going beyond counts and indices, can help identify combinations of diseases associated with especially poor outcomes. Finally, guidelines for reporting of studies on multimorbidity will help with study comparability and reproducibility.
Strengths and limitations
The review provides a comprehensive summary of concepts, data and methods used in multimorbidity research in India. The search strategy was validated through multiple rounds to ensure that expected results were obtained. This validated and tailored search strategy was applied across three databases to compile an exhaustive list of all available articles in the domain. Additionally, citation screening was employed to capture relevant studies that may not have been identified in the initial searches, ensuring a thorough and inclusive review of the existing literature. Further, screening, data extraction, and analysis were performed following a study protocol prepared in accordance with the Joanna Briggs Institute recommendations. The data charting tool was piloted and reviewed multiple times by the research team before the actual data extraction. Study screening and narrative synthesis were performed in consultation with all team members to avoid ambiguities and manual errors.
Given the broad scope of the questions we aimed to address in this review, a scoping review methodology was deemed appropriate for this study. Consequently, neither a meta-analysis nor risk of bias assessment was conducted. The literature search could have utilized other databases such as Scopus, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Global Health, IndMED, Google Scholar, and ProQuest Dissertations and Theses (PQDT). However, it was confined to three major databases – PubMed, Cochrane, and Embase – which was deemed sufficient given access constraints and the scope of this review. Grey literature was not included in the search to maintain focus. Only articles published in English were included. There was considerable variation in how different conditions were named or grouped in different studies. To synthesize information on how often conditions were represented across studies, the conditions had to combined or grouped based on body systems following ICD-11 coding, making it impossible to keep them distinct. These choices may be considered potential limitations of the present study.
Conclusions
This review builds on the findings of existing studies by providing a comprehensive overview of multimorbidity research in India. The findings underscore the importance of developing standardized definitions and measurement tools, justified by purpose and context, to enhance the comparability and reliability of multimorbidity research within India and globally. More longitudinal studies with a focus on multimorbidity and its outcomes will help in the design of interventions for better care for multimorbid people.
Supplemental Material
Supplemental Material - Overview of multimorbidity research in India: A scoping review
Supplemental Material for Overview of multimorbidity research in India: A scoping review by Parul Puri, Siaa Girotra and Arpita Ghosh in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We thank Dr. Abdul Salam, Dr. Rashmi Pant, Rupasvi Dhurjati, and Dr. Sandhya Kanaka Yatirajula from the George Institute for Global Health, India, for their support in testing the search strategy and assisting with data synthesis. We thank Prof. Chris Salisbury and Dr Madhuri Dutta for their help with revising and editing the manuscript. Additionally, we extend our gratitude to the University of South Wales, Sydney, Australia, for providing access to the necessary databases.
Ethical considerations
This review is based on published literature and therefore has no ethical concerns. We have not used individual patient data, thus eliminating privacy concerns.
Authors contributions
Concept and design: AG and PP. Acquisition, analysis, or interpretation of data: AG, PP and SG. Drafting of the manuscript: AG, PP, and SG. Critical revision of the manuscript for important intellectual content: AG, PP, and SG. Analysis: PP and SG. Administrative and technical support: AG and PP. Supervision: AG. All authors have agreed on publishing the final version of manuscript.
Funding
This work was supported by the DBT/Wellcome Trust India Alliance Fellowship IA/CPHI/21/1/505965 awarded to Dr. Arpita Ghosh. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data underlying this research will be made available upon reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.