
Abstract
Background
Multimorbidity is a growing global concern, affecting patient outcomes and healthcare costs. In low- and middle-income countries, data on multimorbidity in primary care beyond prevalence is limited. Our study explored the demographic and clinical characteristics of multimorbidity among older people attending primary health care in Malawi.
Methods
We conducted a cross-sectional analysis on medical records from 15,009 older patients aged ≥50 years across three hospitals in Malawi (one tertiary, two district). Data from 2019-2021 was analyzed using R statistical software to examine patterns of multimorbidity (two or more chronic conditions). Outcome estimates were adjusted for sex, age, location, and year of clinic visit.
Results
The overall prevalence of multimorbidity, defined across 17 recorded chronic conditions, was 19.6%. Among the 2,941 cases of multimorbidity, 2,708 (92.0%) involved two chronic conditions, while 233 (8.0%) involved three. While most conditions increased steadily in prevalence with age, diabetes followed a different pattern, with higher prevalence among individuals aged 50–59 years (53.9%) and 60–69 years (52.4%) compared to those 70 years and older (40.3%). After adjusting for clinic visit year, gender, and study location, individuals aged 70 years and older were significantly less likely to have multimorbidity compared to those aged 50–59 years (AOR = 0.57, 95% CI: 0.52–0.62, p < 0.001).
Conclusion
The study revealed a wide range of multimorbidity combinations among older people attending primary health care. Strategies to address multimorbidity in older people should include efforts to identify other, less common clusters of chronic conditions.
Keywords
Introduction
Many people are now living to old age globally, despite the numerous public health challenges that continue to impact individuals and health systems.1,2 Current evidence shows that with rising life expectancy and improved living conditions, the prevalence of multimorbidity, the simultaneous occurrence of multiple chronic conditions, is also increasing.3,4 This phenomenon becomes more pronounced as individuals age.3,5
Multimorbidity has several consequences, including a reduced quality of life due to the increased clinical complexity of managing multiple conditions, leading to a higher risk of adverse health outcomes. 6 As global populations continue to grow and age, the overall mortality rate and Disability Adjusted Life Years (DALYs) from all causes are expected to rise. 7 However, much of the existing knowledge on multimorbidity primarily stems from studies conducted in the developed Western world reporting higher prevalence in older people compared to the younger generation. 8 Paradoxically, current care models and clinical guidelines for chronically ill patients often prioritize the management of individual conditions in isolation, despite the fact that diseases rarely occur in isolation.3,9 This underscores a limited focus on integrated patient-centered care, which is essential for effectively managing patients with multimorbidity. 10 Highlighting healthcare systems in Low- and Middle-Income Countries (LMICs) has become increasingly vital, especially given the substantial external funding directed towards disease-specific programs, particularly for medications and medical supplies. 11 This emphasis is vital due to the comparatively insufficient funding allocated to broader healthcare infrastructures, which should encompass the management of multimorbidity in such resource-limited settings.
Detailed clinical information regarding older individuals with multimorbidity in Africa remains critically sparse. More so, the epidemiology of multiple chronic conditions remains inadequately understood due to the predominant focus of studies on individual diseases or comorbid pairs linked to a single index disease. 3 However, more evidence in this regard is essential for optimizing resource allocation and improving clinical care for the aging populations. A systematic review on primary health care (PHC) service delivery for older people with progressive multimorbidity in low- and middle-income countries (LMICs), conducted prior to this study and covering articles published between 2012 and 2022, 12 identified only one study from Africa (Nigeria) among a total of seven included studies. This study reported diverse combinations of chronic progressive conditions. 13 This underscores not only the dearth of PHC research focusing on multimorbidity in older people in LMICs but also the fragmented nature of the existing studies. 14
Despite multimorbidity remaining an underexplored area in LMICs, there is an increasing prevalence of Non-Communicable Diseases (NCDs) in these countries. 8 Similarly, there is a paucity of reported data on the prevalence of multimorbidity in Malawi, making it challenging to generalize findings that could inform national-level policy and practice. In this study, we specifically set out to investigate the demographic and clinical characteristics of multimorbidity in older people accessing PHC in Malawi.
Methods
Study design and setting
We conducted a retrospective cross-sectional study extracting routinely recorded clinical data on all older patients aged ≥50 years attending PHC with single and multimorbidity conditions across three distinct public health facilities in Malawi. Malawi, a low-income country in Eastern Africa with an estimated population of 20 million people, is divided into 28 districts across three major administrative regions: Southern, Central, and Northern.15,16 We purposefully selected one health facility from each of these three regions. The selection of these study sites was stratified to ensure representation from each region of Malawi, encompassing a range of settlement types, including rural, peri-urban, and urban areas. The PHC structure in Malawi aims to enhance access to care across all levels of the health system. 17 However, it is common for PHC services to be delivered at higher-level facilities, such as secondary and tertiary health institutions, primarily due to shortages of skilled human resources, essential medicines, and supplies.
In the Southern region, our investigation centred on Mangochi District Hospital, a secondary-level public health facility boasting 500 beds. Mangochi, classified as peri-urban, has an estimated population of 1,346,740 as of 2023. 15 In the Central region, our research was carried out at Kamuzu Central Hospital (KCH), a tertiary-level government referral facility situated in Lilongwe, Malawi’s capital. KCH accommodates up to 1,250 beds and serves approximately 5 million people annually. 18 Our third study site, Mzimba District Hospital, is located in the rural district of Mzimba in the Northern region of Malawi. This secondary-level public health facility comprises approximately 274 beds and caters to a population of around 940,184. 19 In LMICs, a significant number of PHC contacts occur at secondary and tertiary-level facilities due to various challenges, including the lack of diagnostic tools, essential medicines, and a critical shortage of skilled healthcare providers. 12
Data collection
Data was initially collected for multimorbidity, followed by the extraction of additional single chronic conditions from the Outpatient Department (OPD) registers. Recognizing that multimorbidity presents as diverse combinations of progressive conditions in older people, 12 a total of 17 individual conditions—namely Diabetes, Hypertension, HIV, Congestive Cardiac Failure, Cancer, Heart Failure, Asthma, Sickle Cell Disease, Ascites, Chronic Obstructive Pulmonary Disease, Stroke, Peripheral Neuropathy, Arthritis, Retinopathy, Cardiovascular Accident, Epilepsy, and Chronic Kidney Disease—were identified and integrated into the existing multimorbidity dataset. These conditions were used as controls to establish comparable demographic cohorts of older people with multimorbidity.
Data was extracted employing a customized tool (S1) developed in response to the lack of a gold standard for assessing multimorbidity among older people in Malawi. This tool, tailored to the key domains of the OPD registers used across various PHC clinics in Malawi, encompassed socio-demographic information such as serial number, year of visit, clinic type, date of birth/age, gender, and location. In the multimorbidity assessment section, the tool sought documentation of presence of any of the chronic diseases (diagnoses), including HIV status, and visit type (new, follow-up, or referral).
Since no studies from Malawi have specifically examined the prevalence of multimorbidity among older people, the only relevant study involving Malawi, along with Uganda and Gambia, focused on multimorbidity in LMICs of sub-Saharan Africa and recruited participants with a median age of 29. 20 We employed a nonprobability purposive sampling technique. 21 This involved collecting data from medical records of patients accessing PHC services at all three study sites between January 2019 and December 2021. Specifically, records were extracted for patients aged 50 years or older, consistent with the World Health Organization’s (WHO) definition of older people for research purposes in Africa. 22 We collected data over a three-year period to increase the likelihood of capturing a broader range of chronic conditions and identifying potential variations in multimorbidity prevalence, which would be more difficult to detect with data from a single year.
Patient counts for each health facility were determined based on outpatient attendance, using unique serial numbers to ensure that each patient was counted only once per year, with their records not analyzed multiple times. Four field research assistants, stationed at the study sites as data clerks (one each at Mangochi and Mzimba district hospitals, and two at KCH), conducted data extraction. These research assistants underwent a study-specific training to ensure comprehensive understanding of the data extraction process prior to commencement.
Data analysis
The collected data was coded, entered into Microsoft Excel, and then uploaded into R statistical software for analysis. Descriptive statistics were used to present categorical variables as frequencies, percentages, means, and standard deviations. The dependent variable was chronic conditions, while the independent variables included age, gender, year of visit, and location. We defined ‘multimorbidity’ as the coexistence of two or more chronic conditions within an individual.5,23 Inferential statistics were conducted using multivariable logistic regression to calculate and adjust the odds ratios for the factors associated with multimorbidity. We identified patterns of co-occurrence (dyads and triads) of multimorbidity and thoroughly analyzed all possible combinations of two or three comorbid conditions. Chronic conditions were assessed using outpatient encounter diagnoses recorded in the PHC registers. Statistical significance was determined with a 95% confidence interval (CI), and a p-value of less than 0.05 was considered statistically significant.
Ethical considerations
The study adhered to the principles outlined in the Declaration of Helsinki and received approval from the College of Medicine Research and Ethics Committee (COMREC) in Blantyre, Malawi, with the assigned application number P.05/22/3646. Prior to data collection, permission was obtained from the respective study sites. Since the data was anonymized, individual consent for participation was not sought.
Results
Socio-demographic characteristics of older patients accessing PHC.
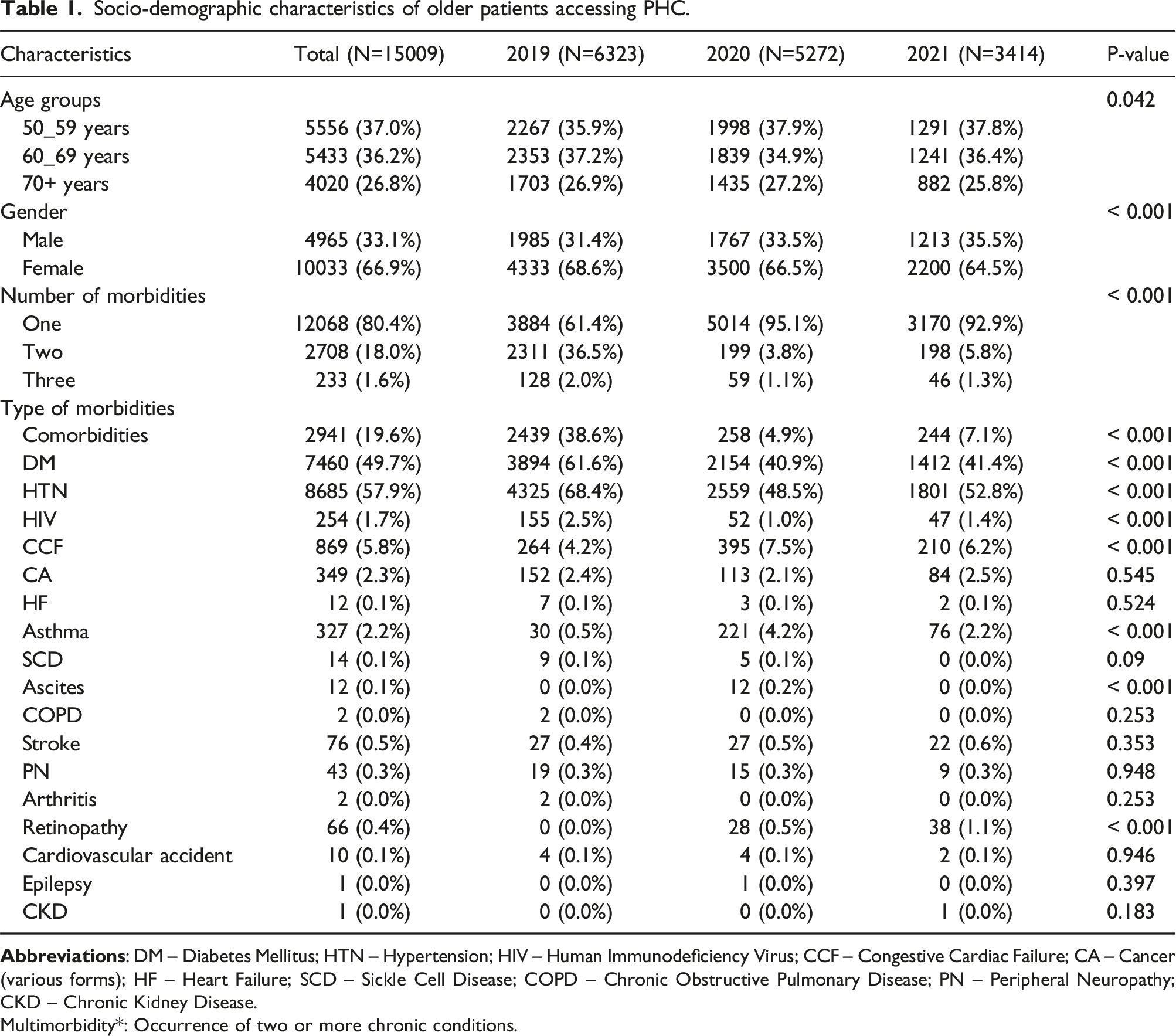
Multimorbidity*: Occurrence of two or more chronic conditions.

A multivariable analysis of factors associated with multimorbidity.
Figure 2(a) depicts the total number of chronic conditions across various age groups, emphasizing the age-related prevalence of multimorbidity. While most conditions show a steady increase in prevalence with advancing age, diabetes follows a different trend. Its prevalence is slightly higher among individuals aged 50–59 (53.9%) and 60–69 (52.4%) compared to those aged 70 and older (40.3%). After adjusting for year of clinic visit, gender, and study location, individuals aged 70 years and older were significantly less likely to have multimorbidity compared to those aged 50-59 years (AOR = 0.57, 95% CI: 0.52–0.62, p < 0.001). However, no significant association was found between individuals aged 60-69 and those aged 50-59 years (Figure 1). Overall, the data indicate a cumulative rise in multimorbidity with age, which plateaus at age 60 and beyond. Prevalence rates of comorbid conditions weighted for age group, gender, location and year of clinic attendance. 
Distribution of single chronic conditions
The prevalence of single chronic conditions, whether isolated or comorbid, across genders is illustrated in Table 1. Overall, 12,068 individuals (80.4%) had isolated single chronic conditions. Figure 2(b) shows that among men (n = 4,965), the most common chronic conditions were diabetes (52.8%), hypertension (51.1%), congestive cardiac failure (7.2%), and other conditions (7.6%). In women (n = 10,033), the leading chronic conditions were hypertension (61.2%), diabetes (48.1%), congestive cardiac failure (5.1%), followed by other conditions (6.2%).
Dyads (two chronic conditions)
Distribution of leading dyads and triads by age group, gender and location.

Triads (three chronic conditions)
Out of 2,941 patients with multimorbidity, 233 (8.0%) had three chronic conditions). Table 2 also shows the distribution of triads by age group, gender, location and year. Overall, the leading triads of hypertension + diabetes + HIV were similar between men and women. Older patients aged 60-69 years exhibited the highest number of cases with the triad of diabetes, hypertension, and HIV, totaling 51 cases (4.5%). This was followed by the 50-59 age group with 44 cases (4.5%), and those aged 70 and above with 15 cases (1.8%). The prevalence of the diabetes, hypertension, and HIV triad was consistent across all age groups in the target population.
Across the study sites, the most prevalent combination of three chronic conditions in Lilongwe and Mangochi was diabetes, hypertension, and HIV. However, Mzimba exhibited a different leading triad, with HIV, cancer, and peripheral neuropathy being the most common combination, occurring in 10 out of 261 cases (3.8%), as shown in Table 2.
PHC attendance and prevalence of multimorbidity (2019-2021)
Out of 15,009 cases recorded over the three-year period, we observed a higher number of older patients attending PHC in 2019, with 6,323 cases (42.0%), compared to 2020 and 2021, which recorded 5,272 cases (35.0%) and 3,414 cases (23.0%) respectively (Figure 2(c) & 2(d)). The prevalence of multimorbidity sharply increased in 2019, reaching 38.6%, but dropped significantly to 4.9% in 2020 and 7.1% in 2021. In 2020, older people had 0.06 times the odds (AOR) of presenting to the PHC clinic with multimorbidity compared to those in 2019 (p < 0.001, CI 0.05–0.07). Similarly, in 2021, they were 0.08 times less likely to present with multimorbidity (p < 0.001, CI 0.07–0.10) (Figure 1).
Discussion
We report the demographic and clinical characteristics of multimorbidity among older patients attending primary care in Malawi.
Our findings revealed that the median age of older people with multimorbidity attending PHC clinics is 62 years. This age is well above the WHO-defined lower limit of 50 years for older people in LMICs, indicating an increased likelihood of developing multimorbidity with advancing age. 22 This trend aligns with global patterns of multimorbidity.3,4,24 However, we observed a plateau in the prevalence of multimorbidity from the age of 60 and above. Individuals with severe multimorbidity often experience higher mortality rates due to the compounded effects of their chronic conditions. 25
Among older people, this increased mortality may be linked to insufficient identification and management of these conditions. In a related qualitative study, we found that older people face multiple barriers to accessing and utilizing PHC services, including a lack of comprehensive care. 26 These challenges may contribute to increased mortality, reducing the likelihood of some affected individuals reaching advanced age. Consequently, the elevated mortality might explain the observed plateau in multimorbidity prevalence within the surviving population. Enhancing access to and utilization of PHC services could improve quality of life and significantly reduce mortality rates in this group. Additionally, investigating specific combinations of chronic conditions is crucial for understanding the impact of multimorbidity on health outcomes and mortality.
The prevalence of multimorbidity in this study was generally similar across genders, in contrast to findings from a systematic review of the World Health Organization’s Study on Global Ageing and Adult Health (conducted in China, Ghana, India, Mexico, Russia, and South Africa), which showed a higher risk of multimorbidity among women. 3 In a related cohort study analyzing secondary data from participants with a median age of 29 in Malawi, The Gambia, and Uganda, findings revealed that Malawian females faced a higher risk of multimorbidity compared to their male counterparts. 20 However, our study suggests that, in the Malawian context, gender-based social, biological, or physical differences may not significantly influence the prevalence of multimorbidity among older people, as seen in other demographic groups. Further research is needed to explore other factors that may contribute to this pattern.
Overall, the prevalence of multimorbidity among older people was 19.6%, which differs significantly from those observed in other LMICs. For example, a study in Burkina Faso found a multimorbidity prevalence of 65.0%, while the prevalence was 57.0% in India and 29.1% in Brazil among the adult population.27–29 Similarly, we observed a steep annual decline in clinic attendance alongside the prevalence of both single and comorbid conditions. In 2019, a larger proportion of older people visited PHC clinics, displaying a higher prevalence of both single and comorbid conditions compared to the following years, 2020 and 2021.
Several factors may account for the variations in multimorbidity prevalence observed in this study. In a related systematic review, we highlighted the insufficient emphasis on person-centered care in LMICs, where holistic assessments were often inadequate. 12 Multimorbidity, especially in older people seeking care for specific conditions, may not have been fully addressed and diagnosed. Conversely, during the first two years of the COVID-19 pandemic, healthcare workers intermittently engaged in industrial action due to issues related to remuneration, working conditions, and a critical shortage of Personal Protective Equipment (PPE). Furthermore, rampant conspiracy theories linked hospitals and healthcare workers to potential COVID-19 transmission, creating fear and apprehension among the general public. Older people, including those with multiple chronic conditions, were equally impacted and tended to avoid hospital visits during 2020 and 2021 due to the rising COVID-19-related deaths. Although Malawi declared a state of national disaster due to the COVID-19 pandemic on March 20, 2020, and confirmed its first case on April 2, 2020, 30 life prior to these events remained largely unchanged. People carried on with their daily routines, reflected in the typically high clinic attendance rates. However, fears escalated following government announcements through electronic and print media, which highlighted conditions and comorbidities—such as advanced age, diabetes, and hypertension—associated with a higher risk of severe and fatal COVID-19 outcomes. 31 Daily updates on confirmed cases and deaths further amplified these fears. The data we analyzed showed that most patients had these risk factors, which might have contributed to reduced social interactions and avoidance of health facility visits in 2020 and 2021. As COVID-19 restrictions intensified, hospital visits were actively discouraged, encouraging individuals to stay home to minimize contact with others. 32 Consequently, these factors might have contributed to a lower observed prevalence of multimorbidity during this period, likely driven by reduced PHC attendance. High public transport fares, resulting from government restrictions on the number of passengers to reduce COVID-19 transmission risk, contributed to reduced access to PHC particularly for older people, most of whom do not have a steady source of income.
Additionally, a lack of awareness about the need for ongoing medical care during the pandemic, long distances to healthcare facilities combined with physical functional challenges, and negative attitudes from some primary care providers significantly impacted access to PHC.12,26 It has also been reported that healthcare utilization patterns change during pandemic disease outbreaks, with high-mortality epidemics like COVID-19 likely reducing demands on the health system.33,34 Strengthening community approaches has proven effective in maintaining PHC services during pandemics. However, to ensure effective utilization of PHC services, response strategies should be developed with input from community representatives and delivered through trusted community actors and structures. 35
Among the three districts examined, Mangochi exhibited the highest prevalence of multimorbidity at 48.7%, followed by Mzimba at 36.7%, and Lilongwe with the lowest prevalence at 16.5%. Such variations could be resulting from the interplay of multiple factors. Evidence suggests a strong link between income levels and various health outcomes. 36 For instance, the main economic activity in Mangochi District is fishing, and the district has a lower income index of 0.374 compared to Lilongwe and Mzimba, which have indices of 0.416 and 0.439, respectively.37,38 This economic characteristic may suggest a more equitable distribution of disposable income among Mangochi residents compared to those in the other two districts. This evidence supports the notion that multimorbidity is more prevalent in affluent households. 39 Conversely, other studies indicate that multimorbidity is associated with socioeconomic deprivation, particularly in cases involving mental health disorders. 24
While our study did not identify mental health disorders, it is crucial to investigate the underlying causes for the coexistence of various chronic conditions in older people. Hypertension was found to be the most common condition, either alone or alongside other chronic diseases. Hypertension and diabetes were the most frequently observed dyads of chronic conditions, with evidence from LMIC supporting their status as the most common comorbidities. 40 The coexistence of hypertension and diabetes, both sharing similar risk factors, is well-documented and often grouped under metabolic syndrome. 41 Since both the diagnosis and management of hypertension and diabetes are handled at the primary care level, many patients may visit PHC clinics for these conditions.
The higher prevalence of hypertension and diabetes can be attributed to increased health literacy among patients, improved symptom recognition by primary care providers, and the availability of diagnostic facilities supported by national programs aimed at managing these conditions in public hospitals. Global estimates of diabetes prevalence in 2017, along with projections for 2045, indicate that low-income countries have the highest proportion of undiagnosed diabetes cases. 42 Similarly, global estimates from 2013 and projections for 2035 show a significantly lower prevalence of diabetes among older adults in low-income countries compared to higher-income countries. 43 These trends align with our findings, which reveal a notable decline in diabetes prevalence between the 50–59 age group and those aged 70 and above. This decline could be attributed to higher mortality rates as individuals reach advanced age. Likewise, despite the rising prevalence of hypertension, studies have highlighted low levels of awareness, treatment, and blood pressure control, particularly in LMICs.44,45 This underscores the need to evaluate national programs to ensure that individuals with these conditions are properly identified and initiated on treatment. Equally, the lower prevalence of other conditions may not accurately reflect the reality on the ground. Evidence suggests that many medical conditions may be underreported or underdiagnosed among people in LMICs. 46 Consequently, this could introduce a bias in mortality reporting, potentially creating a misleading impression that chronic conditions such as diabetes and hypertension—often prioritized due to significant government and international support—are the sole leading chronic conditions affecting older people in these settings. This underscores the need for greater investment in health system capacity planning, including training primary care providers and consistently supplying diagnostic products and medicines to PHC facilities, to effectively identify and treat all conditions, including seemingly rare ones. 7 To garner support and commitment from authorities for PHC facilities that address patients’ interests and needs, advocacy at all levels, including local district councils, policymakers, and the Ministry of Health, is crucial.
Additionally, community engagement initiatives are essential, as they have been proven to raise awareness and increase demand for these services, ensuring that those in need are actually accessing them. 47 This approach would lead to more chronic conditions being reported and treated, significantly improving the quality of life, especially for the older people living with multimorbidity. In our qualitative study, we found that some older people attending PHC at Mangochi District Hospital received transport support from a partner organization. 26 However, this support was not available at KCH or Mzimba District Hospital. This assistance may have contributed to higher PHC attendance rates among older people in Mangochi, increasing their opportunities for multimorbidity screening. Strengthening partnerships with organizations to expand such support could be vital for improving PHC attendance and enhancing the diagnosis and treatment of multimorbidity.
Strengths and limitations
To our knowledge, this is the first study to reveal multimorbidity patterns among older people accessing primary healthcare in Malawi. Data collection was restricted to patients in secondary and tertiary care facilities, excluding primary care facilities. Including primary care facilities could have added other dimensions to the findings. However, our previous systematic review established that older people in LMICs often bypass primary care facilities, opting for higher-level hospitals due to the unavailability of expert service providers and essential medicines needed to manage their conditions. 12
Clinic attendance by older people at PHC facilities may have been impacted by the COVID-19 pandemic. To address this concern, we conducted a three-year data collection study to identify any potential changes in attendance patterns. The data were gathered across three distinct COVID-19 waves in Malawi: the 1st wave (July–November 2020), the 2nd wave (December 2020–March 2021), and the 3rd wave (June–October 2021). 48 Malawi reported its first confirmed COVID-19 cases on April 2, 2020. 49
Despite these limitations, our study provides a timely contribution to understanding the demographic and clinical characteristics of multimorbidity in older people, particularly in Malawi. The findings offer valuable insights for designing care strategies for these patients and have significant implications for program planners, general practitioners, and policy-makers. This information is crucial for the comprehensive and coordinated management of chronic diseases and the delivery of primary care services in Malawi and other related resource-limited settings. Due to the cross-sectional nature of our study, we did not assess causality or disease trajectories. Future research is needed to examine the factors leading to the coexistence of various chronic conditions.
Future research should aim to validate these findings in other settings and populations. Additionally, exploring the implications of different multimorbidity clusters could be crucial for developing integrated care protocols, which currently tend to focus on individual diseases without considering comorbidities.
Conclusions
Our study highlights the specific combinations of chronic diseases that are highly prevalent among older people in Malawi. Our findings underscore the need to address the increasing burden of multimorbidity in policy formulation and health system planning. This includes workforce training, quality improvement strategies, and the development of clinical guidelines that address the concurrent presence of multiple chronic conditions. Additionally, our research emphasizes the importance of strengthening primary care systems in LMICs, as these are the most appropriate settings for managing patients with multimorbidity.
Supplemental Material
Supplemental Material - Demographic and clinical characteristics of older people with multimorbidity accessing primary healthcare in Malawi: A cross-sectional study
Supplemental Material for Demographic and clinical characteristics of older people with multimorbidity accessing primary healthcare in Malawi: A cross-sectional study by Duncan Kwaitana, James Jafali, Maya Jane Bates, Dorothee van Breevoort, Thomas Mildestvedt, Eivind Meland, and Eric Umar in Journal of Multimorbidity and Comorbidity
Footnotes
Authors contribution
DK, MJB, DvB, TM, EM and EU conceived and designed the study; DK collected the data; DK and JJ performed the analysis; DK wrote the manuscript. All authors contributed to editing the manuscript and approved the final version for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded through a clinical PhD fellowship awarded to Duncan Kwaitana by NORHED PRICE Project (NP/70324). Additionally, we extend our gratitude to the Royal Society of Tropical Medicine and Hygiene (RSTMH) for their support in data collection (2022 NIHR043).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.