
Abstract
Background
The relationship between dietary patterns (DP) and health outcomes (elevated blood pressure, dyslipidaemia, hyperglycaemia, and body mass index) among adolescents and young adults (AYA) with HIV is not well understood. We aimed to identify dietary patterns and determinants associated with metabolic syndrome components among adolescents and young adults living with HIV in Lagos, Nigeria.
Methods
We conducted a cross-sectional study among 180 participants at an ART clinic in Lagos. Information on sociodemographic and clinical characteristics, as well as 72-hour dietary recall were collected. Anthropometric measurements (BMI (kg/m2)) and blood pressure readings were collected. Blood samples were assayed for fasting blood sugar and lipid profiles. Statistical analysis was done using SPSS version 27, WHO Anthro Plus software.
Results
The male-to-female ratio was 1:1. Four major DPs identified were DP 1 (higher consumption of beverages, vitamins, and vegetables); DP 2 (high intake of minerals, and fruits); DP3 (higher intake of carbohydrates, fat and oil); and DP4 (higher intake alcohol and vegetables). DP1 was associated with dyslipidaemia, underweight BMI and hyperglycaemia were associated with DP4, while DP2 had lower odds of overweight and elevated blood pressure.
Conclusion
This outcome provides valuable insights into DPs and their association with metabolic co-morbidity among AYA with HIV. This will inform nutritional counselling and interventions to promote quality of life and health.
Adolescents and Young Adults living with HIV (AYA with HIV) are at an increased risk of developing co-morbid metabolic disorders, majorly originating from Antiretroviral therapy. Our study explored the contribution of diets to the burden of these comorbid metabolic disorders among AYA with HIV. The study participants on diets rich in minerals, fruits, and vegetables were found to be protective against hypertension and overweight. This will guide the development of nutritional guidelines for AYA with HIV to curtail the adversity of metabolic disorders.Key messages
What is already known this topic
What does this study add(s)
How affect research, practice or policy
Introduction
Adolescence and youth are critical in the growth and development phase towards the transition to adulthood.1,2 This age group (adolescents and young adults) faces various challenges that could undermine achieving maximal human capabilities and capacities, particularly nutrition.2,3 The nutritional status among this age group is influenced by risk factors, such as peer influences, parental modelling, food availability, food preferences, cost, convenience, personal and cultural beliefs, mass media, and body image that modulates their overall well-being.4,5 Special populations such as adolescents and young adults (AYA) living with chronic diseases are of particular interest due to the interplay between immune status and nutrition. 3
Research has shown varied dietary patterns among AYA with HIV, ranging from diets rich in fruits, vegetables, lean protein, and whole grains to those high in processed and fast foods with low nutritional value.6–9 The dietary patterns among AYA with HIV can have significant long-term health implications, such as elevated blood pressure, hyperglycaemia, dyslipidaemia and unhealthy BMI (underweight/overweight/obesity), which can undermine the gains of antiretroviral therapy (ART) and their overall well-being.10,11 Balanced diets are essential for enhancing immune response, improving ART efficacy, and maintaining this cohort’s optimal health.12,13
Adolescents and young adults, especially those with HIV, often receive insufficient attention regarding their diet, resulting in a poor understanding of their dietary behaviours.3,14,15 Emerging adulthood, a key stage for developing lifelong healthy habits, requires clear nutritional guidelines and education to promote better dietary choices. Targeted strategies, including nutrition-focused interventions, are essential to enhancing the well-being of AYA with HIV(3,14,15).
Therefore, considering the importance of diet to health in this cohort, our study aims to investigate the relationship between specific dietary patterns and metabolic comorbidities among AYA with HIV. The study will also characterize the common dietary patterns, as well as determine the association between dietary patterns and metabolic disorders components (hyperglycaemia, hypertension, dyslipidaemia and nutritional disorders (underweight/overweight/obesity) among AYA with HIV. We hypothesize that certain dietary patterns are associated with elevated blood pressure, dyslipidaemia, hyperglycaemia, and unhealthy (underweight/overweight/overweight) BMI) among AYA with HIV. This will provide valuable information that could inform nutritional guidance/counselling and the development of interventions to promote healthy dietary habits and lifestyles to enhance response to ART, immune function, and ultimately, improve the health and overall quality of life among AYA with HIV.
Methods
This was a prospective quantitative cross-sectional study among adolescents and young adults (AYA) with HIV (aged 10 to 24 years) who attended the ART Clinic at the Clinical Sciences Department of the Nigerian Institute of Medical Research (NIMR), Yaba, Lagos, Nigeria, between July and October 2019. The ART clinic is in the commercial capital of Nigeria and offers comprehensive HIV care and treatment to adults, adolescents, children and pregnant women. The ART clinic operates an adolescent-friendly clinic on the second Saturday of every month with about four hundred AYA with HIV currently in care. A cross-sectional design was chosen to provide a snapshot of the dietary patterns and their associations with metabolic comorbidities in AYA with HIV. This study design was done to ensure efficient data collection and cost-effectiveness. Eligible participants were AYA with HIV who had been on antiretroviral drugs for at least six months and consented (consent ± assent) to participate in the study. Excluded study participants were AYA with HIV with significant co-morbidities (seizure disorders, sickle cell anaemia, chronic hepatitis B infection, and those with acute illness) and those who were pregnant.
A sample size of 189 was determined using the Raosoft© online calculator. The calculation was performed with a 5% margin of error, 95% confidence level, a response distribution of 50% and a population of 300 AYAs with HIV attending the facility based on the ART clinic database at the conception of the study. Furthermore, an attrition rate of 10% was considered. A convenient sampling technique was used to select the required number of study participants. A case report form was used to obtain information on sociodemographic and clinical characteristics, clinical examination, laboratory parameters, and dietary patterns.
Socio-demographic and clinical characteristics
Age, gender, education, occupation, clinical parameters (age at HIV diagnosis, duration and type of ART, and family history of comorbidities [hypertension and diabetes mellitus]), physical examination (anthropometric measurements, blood pressure readings) and recent laboratory parameters (HIV RNA viral load and CD4 count within the 6 months of the study period).
Dietary information was obtained from respondents using the 72-hour dietary recall tool, which was administered three times to the study respondents (twice on a weekday and once on a weekend) to provide a detailed view of dietary intake among study participants. This information was analyzed and categorized into five classes of food (carbohydrates, fat and oil, minerals, vitamins, and proteins), with alcohol, beverages, fruits, and vegetables being extra classes.
Clinical examination
The anthropometric measurements (weight in kilograms, height in centimetres) were obtained with the patient in light clothing and barefooted using the Seca® combination weighing scale and stadiometer. The body mass index (BMI), expressed in kilograms per square meter, was calculated from the weight and height measurements. The BMI measurements were converted into z-scores using the WHO AnthroPlus software, a tool specifically designed for assessing the growth and development of children and adolescents. The z-scores provide a standardized way to compare the adolescents’ growth to a reference population.
Two blood pressure readings were obtained one minute apart, using an electronic sphygmomanometer (Omron M3 Intellisense TM, Model: M3 (HEM-7131-E [Omron Healthcare Co. Ltd]) with the participant comfortably seated and the right arm placed at the level of the participant’s heart. The mean of the two readings was recorded as the participant’s blood pressure. A third measurement was conducted after another 20 minutes if a high reading was obtained. The mean of the two closest readings is recorded as the participant’s blood pressure. Point Hypertension was defined as a blood pressure reading ≥ 95th percentile for age, sex, and height or readings above 130/80mmHg irrespective of participant’s age or gender. 16
Laboratory parameters
After a 12-hour fast, approximately 6 ml of venous blood was collected from the antecubital fossa of each participant to determine their fasting lipid profiles [total cholesterol, triglycerides, high-density lipoprotein-cholesterol (HDL-c), and low-density lipoprotein-cholesterol (LDL-c)] using Roche C311 Clinical Chemistry autoanalyzer. Hypertriglyceridaemia (TG ≥ 110mg/dl) and/or low HDL-c (≤ 40mg/dl) were used to define dyslipidemia as these are the two major predictive parameters for the development of cardiovascular disease. Age and gender-specific lipid profile cutoff points were used (normal and abnormal categories).
Dietary pattern assessment
Dietary patterns were determined using exploratory factor analysis (EFA). Kaiser–Meyer–Olkin (KMO; value of p > 0.05) and Bartlett’s test of sphericity (value of p < 0.05) were used to check the adequacy of the sample-to-factors ratio. The existence of a correlation between food items was determined for each step of factor analysis. Then, EFA was done under orthogonal rotation with the varimax method to enhance the interpretability and independent dietary patterns. In determining the final dietary patterns, we considered factors with a communality above 0.2 and an eigenvalue greater than 1. These factors account for more variance than a single variable and are deemed significant in principal components analysis that reflect distinct consumption behaviours within the population.
Nutritional status assessment
The nutritional status of the participant was assessed through anthropometric measurements which include height, and weight, informing the calculation of the Body Mass Index (BMI). The World Health Organization (WHO) classification for adolescents was adopted, using age- and sex-specific growth charts. BMI is categorized as follows: underweight is below the 5th percentile, normal weight is between the 5th and 85th percentiles, overweight is from the 85th to less than the 97th percentile, and obesity is at or above the 97th percentile. While for the young adults aged 20–24, the WHO standard adult BMI classification was applied. The categories were underweight (BMI < 18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25.0–29.9 kg/m2), and obesity (BMI ≥ 30.0 kg/m2).
In this study, we identified distinct dietary patterns among AYA with HIV and determined how these eating habits influenced the study participants’ nutrition and health. To achieve this, we employed regression models to evaluate the relationship between dietary patterns (exposure variables) and nutritional status as well as metabolic disorders (outcome variables). This approach provided a robust framework to understand the potential impact of dietary patterns on the health of study participants.
Statistical analysis
A descriptive analysis was performed to characterize the dataset, employing frequencies, percentages, means, and standard deviations. The distribution of each variable was assessed to determine the normality, with outliers identified as values outside of the range (mean ± 3SD). The chi-square test was used to assess the association between variables and gender, while binary logistic regression analysis was used to determine the association between dietary patterns (DPs) with sociodemographic characteristics and metabolic disorders. Multivariate logistic regression analysis was done to assess further correlation between the DPs and metabolic disorders while controlling for covariates in the models (Model 1 was adjusted for age and sex; Model 2 adjusted for age, sex, education, ethnicity and religion). Missing values and outliers for interested variables below a threshold of 5% of the total population were replaced with the mean (normally distributed data) or median (non-normally distributed data). Statistical analysis was done using SPSS version 27, WHO Anthro Plus software, and R studio, with statistical significance set at a p-value ≤ 0.05.
Ethical issues
Ethical approval was obtained from the Institutional Review Board (IRB) of the Nigerian Institute of Medical Research, Lagos before the commencement of the study. All enrolled participants and/or caregivers were provided informed written consent at enrollment into the study.
Results
Gender-specific classification of sociodemographic and HIV characteristics.

Gender-specific metabolic disorders.
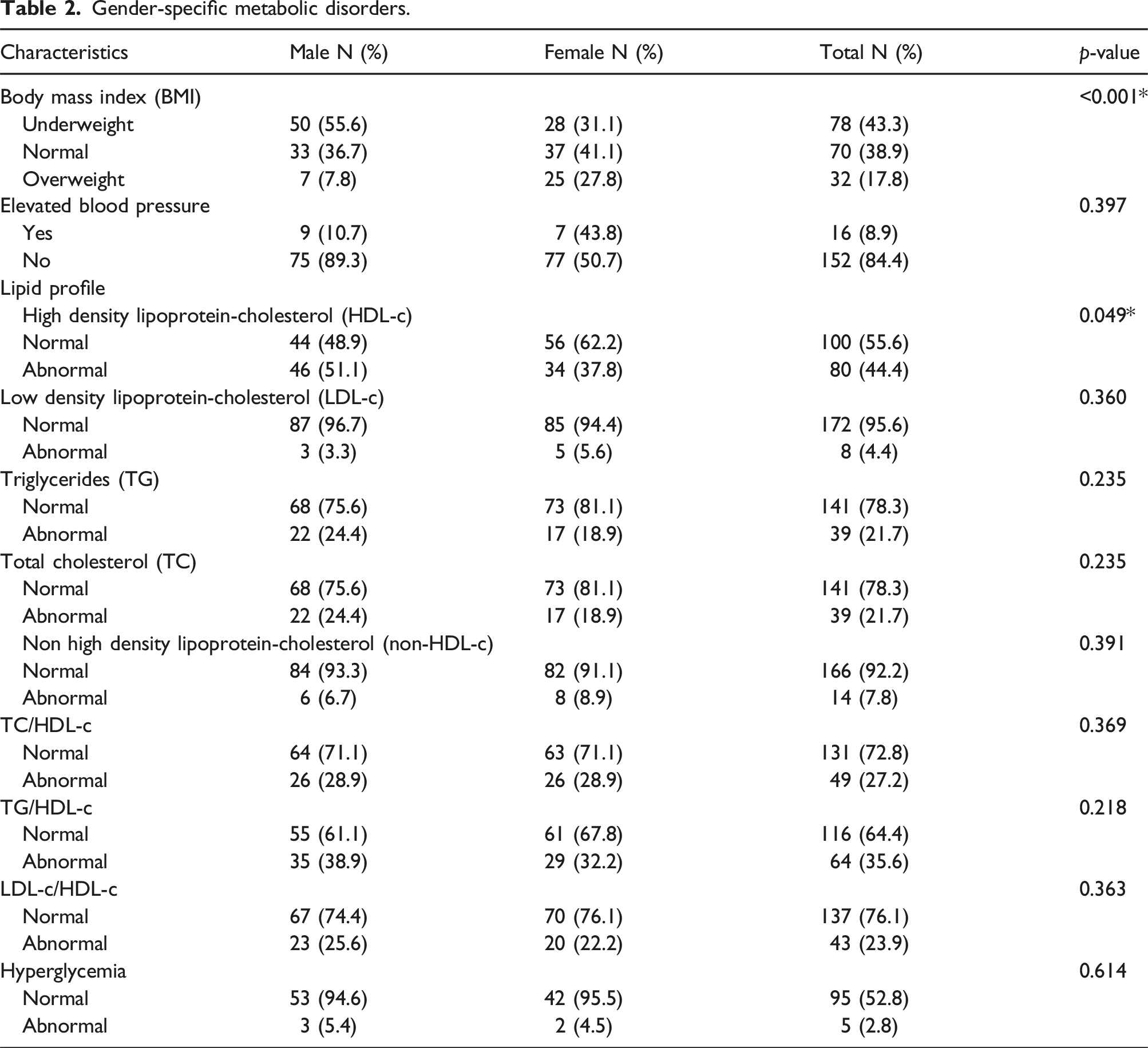
The prevalence of hypertension in the study was 9.5%, with the lipid profile revealing abnormal HDL-c (44.4%), LDL-c (4.4%), Triglycerides (21.7%) and Total Cholesterol (21.7%) levels among study participants. Only 2.8% of the study population had abnormal fasting hyperglycaemic levels (Table 2).
Figure 1 depicts the four dietary patterns identified among AYA with HIV enrolled in the study. These dietary patterns account for approximately 65% of the study population (Supplemental data Table S1, S2 and S3). Dietary pattern 1 (23.5%) is characterized by higher consumption of beverages, vitamins, and vegetables while dietary pattern 2 (16.4%), contains predominantly minerals and fruits but is low in vegetables, carbohydrates, protein, and other essential nutrients. Dietary pattern 3 (13.2%) consists of high consumption of carbohydrates, fats and oil, along with low micronutrient content, while dietary pattern 4 (11.6%) had a high composition of alcohol, vegetables, and minerals, but low protein and carbohydrate content. (Figure 1). Dietary patterns among study participants following meal 72 hour recall.
Dietary patterns and BMI (underweight and overweight)
Association between sociodemographic status and dietary patterns.

Dietary patterns and blood pressure
Regression model to assess the association between dietary patterns and metabolic disorders.

Model 1: Adjusted for age and sex.
Model 2: Adjusted for age, sex, education level, ethnicity and religion.
p-value < 0.05 – statistically significant.
Dietary patterns and hyperglycaemia
Only dietary pattern 4 was associated with hyperglycaemia irrespective of the model utilized (p <0.05). Table 4
Dietary patterns and dyslipidaemia
Regression association between abnormal lipid indices and dietary patterns.

Discussion
Our study explores the association between dietary patterns and metabolic disorders (BMI, elevated blood pressure, dyslipidaemia, hyperglycemia) among AYA with HIV at a large ART clinic in Lagos, Nigeria. We identified four distinct dietary patterns with varying associations with metabolic disorders in the study population. Dietary pattern 1 was positively associated with higher likelihood of underweight and dyslipidaemia. Dietary pattern 2 was protective against elevated blood pressure and overweight, while dietary pattern 4 was associated with study participants being underweight and hyperglycaemic. Dietary pattern 3 did not show any association with any component of metabolic disorders.
The prevalence of underweight at 43.3% among AYA with HIV is within the prevalence reported (2 – 63%) among adolescents with HIV in LMICs in a recent systematic review. 17 However, our prevalence was higher compared with the reported prevalence of 27% in Nigeria, 18 20 - 27.2% in different studies across Ethiopia8,19,20 and 18% in Uganda. 21 The wide disparity in the prevalence could be attributed to the variation in study design, study settings, socioeconomic status and cultural values/disposition. Our findings buttress the burden of nutritional challenges among the HIV cohort, even in the era of test and treat protocol. The high demand for nutrients (required growth and development) in this age group irrespective of HIV status, is inundated with food insecurity and unbalanced energy expenditures. The prolonged span of undernutrition in the foetal and under-5 age group, along with the catabolic effects of HIV could explain the high prevalence of underweight. The disproportionate underweight burden among males is in concordance with prior studies in LMICs irrespective of HIV status.17,22–24 This could be attributed to the increased energy requirements and physical exertions among males amid poor food choices and socioeconomic status. 25
Dietary pattern 4 was characterized by low content of carbohydrates and proteins which are essential for growth and development but remain difficult to access due to prevailing food insecurity, food inflation and poor food choices in LMICs.4,5,25 In addition, underweight BMI status was also associated with alcohol consumption among AYA in our study similar to findings in previous studies.26–29 Although our findings differ from previous studies that have associated overweight/obese BMI status among adolescents with alcohol consumption, most of these studies did not include AYA with HIV population.30–33 Given the background HIV infection, poor appetite, opportunistic infections (in the gastrointestinal tract), and malabsorption of nutrients may result in the underweight status of our study populace. Future studies are required to delineate the impact of alcohol and dietary patterns on weight changes among AYA with HIV.
The prevalence of 17.8% for overweight among the AYA with HIV, with the female gender accounting for a higher proportion of the individuals who were overweight. This is higher than the reported overweight prevalence (6.1 - 15.6%) in a systematic review and meta-analysis by Gebrie et al. 17 The increased prevalence of overweight could be attributed to the positive effects of ART, creating a significant reversal of the catabolic effects of HIV infection and a corresponding reduction in inflammatory markers with resultant improved appetite and nutrient uptake.
The protective effect of dietary pattern 2 (rich in minerals and fruits) in preventing overweight affirms previous studies corroborating the importance of micronutrient intake which occurs by modulating the body’s metabolism, immune system, systemic inflammation, and oxidative stress.34,35 Although it is noteworthy that the current study focuses on dietary intake among the study population with chronic illness (HIV), other variables beyond the scope of our study could predispose to overweight/ obesity. These factors include genetics, other chronic diseases, drugs, and environmental factors.17,36–38
The burden of hypertension (9.5%) is within the pooled prevalence (0.2-24.8%) reported in a systematic review and meta-analysis in sub-Saharan Africa. 39 Our prevalence differed from the reported prevalence by (6.9%) by Odubela et al., 40 (10.5%) by David et al., 41 and 11% by Nsanya et al., 42 although there were variations in the study populations. In addition, our finding is lower than the prevalence estimates (10-40%) in Africa’s general population of adolescents and young adults, 29% by Lubega et al. 43 and 49% reported by Migisha et al. 44 in Uganda. The variability in the prevalence of hypertension could be due to genetic, racial, lifestyle and environmental factors. Dietary pattern 2 was protective against elevated blood pressure. This dietary pattern displays the interplay between diet composition and hypertension.45–47 Our finding affirms the effectiveness of dietary and lifestyle modifications in the prevention and management of elevated blood pressure and its complications.
The prevalence of hyperglycaemia among the participants was 2.8%. This finding is within the range of 2 - 28% in sub-Saharan Africa,41,48–51 0.4-7% in America,52–55 Europe,56,57 and 2.6 - 43% from the Asian continent.58,59 Significant contributors to hyperglycaemia include chronic inflammatory response (arising from HIV infection) and effects of ART (mitochondrial toxicity, altered endoplasmic reticulum function, alteration in adipocytokines & lipid metabolism, impaired insulin signaling pathways) in addition to other traditional risk factors.49,60–64 Excessive alcohol consumption can induce insulin resistance as alcohol can interfere with the liver’s ability to regulate blood glucose, predisposing to diabetes mellitus. 65 This aligns with previous studies on the relationship between blood sugar, metabolic disorders and alcohol intake in the general population.66–68
The pattern of dyslipidaemia with abnormal HDL-c ratios found in our study aligns with reports from across Africa.69–73 However, a reverse pattern of higher prevalence of hypertriglyceridaemia followed by low HDL-c was reported in other studies in Africa,74,75 Asia58,76 and Europe. 57 This variation could be due to genetic differences, dietary status and the class of ART. In consonance with prior studies, beverage consumption (DP 1) was associated with dyslipidaemia.77–79 Our finding buttresses the adverse implications of high beverage intake and dyslipidaemia. Thus, the evidence supports the need to improve the reach and quality of health information available to AYA to promote healthy eating habits and curtail adverse health conditions of metabolic disorders such as dyslipidaemia, obesity, diabetes mellitus and cardiovascular diseases.80,81
Strength and limitations
This study is one of the first to describe dietary patterns and their association with common metabolic disorders (elevated blood pressure, hyperglycaemia, abnormal body weight and dyslipidaemia) among AYA with HIV in Africa. Food recall, the nature of the study design (cross-sectional), and the number of food servings limit the generalization of our findings. The study did not account for environmental or sociocultural factors that may impact food intake, quality and quantity.
Conclusion
This study provides valuable insights into the dietary patterns and its association with metabolic disorders. It also provides evidence of the association between dietary patterns and metabolic disorders among AYA with HIV. The study findings affirm the need for comprehensive care to ensure the gains of HIV care are consolidated and promote wholesome health among AYA with HIV. This will entail continuous nutritional counselling and prompt monitoring of modifiable and non-modifiable risk factors to curtail the burden of non-communicable diseases. This finding will help inform nutritional guidance/counselling and the development of interventions to promote healthy dietary habits, prevent the onset of NCDs and, ultimately, improve the quality of life of AYA with HIV.
Supplemental Material
Supplemental Material - Dietary patterns and metabolic morbidities correlate among adolescents and young adults with HIV in Lagos, Nigeria: A cross-sectional study design
Supplemental Material for Dietary patterns and metabolic morbidities correlate among adolescents and young adults with HIV in Lagos, Nigeria: A cross-sectional study design by Mobolaji Olagunju, Abideen Olurotimi Salako, Titilola Abike Gbaja-biamila, Tomilola Musari-Martins, Priscilla Ngozi Ezemelue, Olusola Opaneye, Abubakar AhmadRufai Abubaka, Odusote Oluwatomisin Ibukun, Feyikemi Fasina, Adeniyi Adeyinka, Oreoluwa Alabi, Agatha Nkiru David, Lilian Ezechi, and Oluwatosin O. Odubela in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
Our sincere appreciation to the adolescents and young adults with HIV (AYA with HIV) and their caregivers/parents who participated in the study. Also, we appreciate the unflinching trust in the staff at the Clinical Sciences Department (CSD) at the Nigerian Institute of Medical Research (NIMR) by the AYA, parents/caregivers for over two decades. Furthermore, our depth of gratitude goes to the nurses, counsellors/social workers, members of the data unit, and the laboratory team at the Centre for Human Virology and Genomics, who have continued to work tirelessly towards improving the health and well-being of people living with HIV, especially AYA with HIV.
Ethical statement
Authors contributions
Conceptualization: AOS, MO, OOO, OO, TM, LE, NAD, TAG. Methodology and Data Collection: AOS, OOO, TM, PNE. AAA, TAG. Data Analysis-, MO, AOS, OOO, OO, AAA, TAG. Writing (Original Draft): AOS, MO, OOO, FF, AA, Writing – review & editing: AOS, OOO, OO, PNE, AAA, TM, FF, AA, LE, NAD, TAG. Supervision: AOS, OOO, LE, NAD, TAG.
Funding
No financial support or grant.
Declaration of conflicting interests
The authors declare no competing interest.
Data Availability Statement
All data generated or analyzed during this study are included in the published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.