
Abstract
Background
The co-occurrence of chronic diseases and acute infectious events exacerbates disability and diminishes quality of life, yet research in Low- and Middle-Income countries is scarce. We aimed to investigate the relationship between infectious events and multimorbidity in resource-constrained settings.
Methods
We conducted a sequential mixed-method study in Lima and Tumbes, Peru, with participants having multimorbidity from the CRONICAS Cohort Study. They completed a questionnaire on the occurrence, treatment, and health-seeking behaviour related to acute infectious events. Qualitative interviews explored the perceptions and links between multimorbidity and acute infectious events for a subgroup of participants.
Findings
Among individuals with multimorbidity, low awareness of chronic conditions and poor medication adherence. The cumulative incidence for respiratory and gastrointestinal infections, the most reported acute conditions, was 2.0 [95%CI: 1.8–2.2] and 1.6 [1.2–1.9] events per person per year, respectively. Individuals with cancer (6.4 [1.6–11.2] events per person per year) or gastrointestinal reflux (7.2 [4.4–10.1] events per person per year) reported higher cumulative incidence of infectious events than others, such as those with cardiovascular and metabolic conditions (5.2 [4.6–5.8] events per person per year). Those with three or more chronic conditions had a slightly higher cumulative incidence compared with individuals with two conditions (5.7 [4.4–7.0] vs 5.0 [4.4–5.6] events per person per year). Around 40% of individuals with multimorbidity sought healthcare assistance, while others chose drugstores or didn't seek help. Our qualitative analysis showed diverse perceptions among participants regarding the connections between chronic and acute conditions. Those who recognized a connection emphasized the challenges in managing these interactions.
Interpretation
Our study advances understanding of multimorbidity challenges in resource-limited settings, highlighting the impact of acute infections on patients' existing multimorbidity burden.
Introduction
Globally, the average population age and life expectancy have increased. 1 Associated with this, the prevalence of chronic physical and mental health conditions such as diabetes, hypertension, chronic obstructive pulmonary disease (COPD) and depression have also increased, making the co-occurrence of two or more chronic conditions more frequent. This phenomenon, known as multimorbidity,2–4 is rising in importance as a clinical and public health concern due to its negative effects at both the individual and societal level.5,6
Many healthcare systems in low- and middle-income countries (LMICs) are not prepared to address long-term chronic conditions, including multimorbidity.7–9 Additionally, LMICs also carry a high burden of acute infectious diseases, 10 making it highly likely for people to experience acute events on top of their chronic health conditions. There is little study of the intersection between acute infections and multimorbidity. The co-occurrence of multiple diseases, whether chronic or acute, might be due to common pathophysiological mechanisms or shared risk factors associated with these conditions. For example, chronic respiratory conditions such as asthma and COPD are often exacerbated by bacterial or viral infections,11,12 increasing existing morbidity in people with those conditions. 11 In addition, it is known that susceptibility to these exacerbations varies among patients and that some of their risk factors are poor treatment and altered immune markers. 12 Also, it has been reported that patients with COPD and cardiovascular disease (CVD) have higher risk of developing community-acquired pneumonia compared to those with CVD alone. 13 Furthermore, it is known that diabetes has direct impacts on the immune system, increasing morbidity and mortality from infectious diseases.14–16 A recent example is the elevated mortality rates observed among COVID-19 patients with multimorbidities. 17 Conversely, it has also been noted that individuals with one pre-existing chronic condition face a significantly increased risk of developing multimorbidity following a COVID-19 episode. 18
The co-occurrence of chronic diseases and acute infectious events increases disability and reduces quality of life, 19 yet there is very little work exploring this in LMICs. In this study, leveraging data from the CRONICAS Cohort Study, 20 spanning urban and semi-urban areas across different geographies in Peru, we re-contacted participants with multimorbidity, i.e., two or more chronic health conditions, residing at sea level. Following a mixed-methods approach, combining quantitative and qualitative techniques, we sought to explore the links between infectious events and multimorbidity as well as the experience of infection-related acute events among people with two or more chronic conditions in resource-constrained settings.
Methods
Study design
This is a sequential mixed-method study, 21 with a quantitative phase followed by a qualitative phase in participants with multimorbidity from two sites of the CRONICAS Cohort Study. 17 The qualitative phase included a sub-sample of the participants.
Study settings and participants
The CRONICAS Cohort Study, described in detail elsewhere, 20 is a longitudinal cohort conducted in four Peruvian settings that differ by level of urbanization, household air pollution, and altitude. This cohort study had three evaluations, one at baseline, which took place in 2010, and two subsequent follow-ups, spaced approximately 15 months apart. The main study's inclusion criteria required participants to be 35 years old or older, permanent residents in the area, capable of comprehending procedures, and able to provide informed consent. Conversely, the exclusion criteria encompassed pregnant individuals, those with cognitive incapacity affecting consent or questionnaire responses, individuals with physical disabilities impeding measurements, active pulmonary tuberculosis cases, and a restriction allowing only one participant per household to enrol. 20
In the present study, participants with multimorbidity from the CRONICAS Cohort Study sites from Pampas de San Juan de Miraflores, a peri-urban community in Lima, and from a group of semi-urban communities in Tumbes, northern Peru, both at sea level, were re-contacted. All data for this mixed-method study were collected in Spanish between November and December 2019, nine years after the baseline assessment was conducted.
Identification of participants with multimorbidity
Chronic conditions assessed during the CRONICAS Cohort Study to define multimorbidity for the present study.

COPD: Chronic Obstructive Pulmonary Disease; FU1: first follow-up of the CRONICAS Cohort Study; FU2: Second follow-up of the CRONICAS Cohort Study.
Procedures for the mixed-method study
Quantitative phase: Door-to-door survey
All individuals identified from the CRONICAS database with multimorbidity from Lima and Tumbes were re-contacted and surveyed by trained personnel who had previously worked on the study sites. Electronic forms implemented in Open Data Kit (ODK) were used for the survey. The study coordinator reviewed the uploaded data daily to ensure its consistency and quality.
Questionnaire
The questionnaire contained the following sections: demographic and current socioeconomic information; self-reported diagnosis of chronic conditions and their current treatment and treatment adherence to the following conditions: (1) Hypertension, (2) Type 2 diabetes, (3) Asthma, (4) Chronic bronchitis, (5) COPD, (6) Depression, (7) Cancer, (8) Heart failure, (9) Stroke, and an opened question for other chronic conditions. The medication adherence question presented three response options: a) almost never or occasionally, b) only during discomfort due to illness, and c) as specified by the physician. Participants were considered adherent when they reported the last option. We then collected data on self-reported acute infectious events in the previous 12 months, including infection frequency, treatment, and help-seeking behaviours (i.e.: for each kind of infectious condition, when this type of event occurs, who or where do you turn for help?) for the following type of infectious events: (1) Respiratory, (2) Gastrointestinal, (3) Urinary, (4) Oral, (5) Skin and soft tissues, and an open question for other infections; and, number and reason for hospitalisations if any. Socioeconomic status was calculated and presented as tertiles based on the sum of the inverse probability of owning 14 of the following possessions: gas stove, toilet with drain, radio, colour TV, refrigerator, washing machine, computer, landline, cell phone, cable, Internet, bicycle for adults, motorcycle, and car; also, monthly family income was asked.
Cumulative incidence of acute infectious events
Using the frequency of the self-reported acute infectious events, the cumulative incidence was calculated by type of infection condition and in total by computing the average of acute infectious events reported during the previous 12 months by all the people surveyed. It is expressed as the number of events per person in the previous 12 months.
Type of chronic condition-groups
To assess whether specific types of chronic conditions were associated with a higher cumulative incidence of acute infectious events, based on the conditions that determined multimorbidity in our study (Table 1) five groups of chronic condition types were defined, and an analysis was done with each of them, coding 0 if the participant had none of the conditions of the group, and as 1, if the participant had at least one of conditions included in the group. The groups are defined as: (1) Pulmonary group, which includes asthma, chronic bronchitis, and COPD; (2) cardiovascular (CV) and metabolic group, which includes hypertension, type 2 diabetes, heart failure, peripheral arterial disease, and stroke; (3) mental health group, which includes alcohol disorder and depression; and (4) cancer and (5) gastrooesophageal reflux were considered separately as a fourth and fifth group. For example, for the Pulmonary group, if the participant had one or more of the pulmonary conditions mentioned above, he/she was coded as 1. If the participant had other conditions except for a pulmonary one, he/she was coded as 0 in that group. The cumulative incidence of acute infectious events was calculated only for subjects coded as 1 in each group, and then compared among the five groups. Additionally, we calculate the cumulative incidence of acute infectious events based on the number of chronic conditions (two chronic conditions, three or more chronic conditions) reported during any previous CRONICAS Cohort Study evaluation.
Data analysis
For quantitative data analysis, proportions, means (± standard deviations), or medians and interquartile ranges (percentile 25 to percentile 75) were calculated as appropriate. Differences in the distribution of categorical variables were determined using Chi-squared or Spearman (non-parametric) tests, depending on the expected frequencies of the categories. Data were analysed using Stata v16 (StataCorp, College Station, Texas, USA). Data from re-contacted and not re-contacted participants are shown in Supplementary Table 1.
Qualitative phase: Semi-structured interviews
In this phase, qualitative semi-structured interviews were conducted in a subgroup of 16 participants that, during the quantitative phase, recognized having two or more chronic conditions, and self-reported having had at least one acute infectious event in the previous 12 months. This is because we wanted to gain deeper insights into their experiences but ensuring that participants were fully aware of the chronic or acute health conditions discussed during the interview. A sex and site-stratified random sample of them was taken, having 4 males and 4 females from each site. Names were provided to fieldworkers, who scheduled a visit for the interview. If the selected subject had problems making themself understood or did not have time to participate in the interview, another subject, from the same sex and site was randomly selected.
Interview guide and procedure
Topics and sub-topics used to guide the semi-structure interview from the qualitative phase.

Data analysis
The interviews were digitally recorded and then transcribed verbatim. Transcriptions were coded using ATLAS.ti v7 software (Scientific Software Development GmbH, Berlin, Germany). A first codebook was developed based on the main topics and questions of the interview guide, and additional codes were included when new relevant topics emerged. However, notwithstanding the extensive nature of the codes generated, this study selectively focuses on the analysis of codes pertinent to the study’s primary objective focused on exploring the connection between acute infectious events and multimorbidity in resource-constrained settings.
Ethical considerations
The study protocol, informed consent forms, and instruments were approved by the Institutional Ethics Committee of Universidad Peruana Cayetano Heredia (SIDISI 102440). Written consent was obtained from all survey participants, who also consented to be interviewed and recorded for the qualitative phase, in case they were selected.
Results
Multimorbidity in the CRONICAS Cohort Study and participants re-contacted and surveyed for this evaluation
Using the information collected during the three CRONICAS Cohort Study, we found that 584 out of 2137 (27%) subjects living in Lima (350/1105 ≈ 32%) and Tumbes (234/1032 ≈ 23%) had multimorbidity. When comparing CRONICAS Cohort information, there were some differences, e.g., we found a higher proportion of people with chronic bronchitis (47/90) and peripheral artery disease (34/59) in participants with multimorbidity re-contacted and surveyed in this evaluation when compared with those not surveyed (Supplemental Table 1 provides characteristics of all participants with multimorbidity that we were able to re-contact and those we were not able to re-contact). Among the individuals with multimorbidity, 93 had passed away, leaving 491 individuals potentially re-contactable. Out of this group, we successfully administered questionnaires to 347 individuals, resulting in a response rate of approximately 71%. The reasons for loss to follow-up included individuals moving out of the community (n = 61), discontinued participation in the previous follow-ups (n = 29), lack of interest in participation (n = 26), loss of cognitive function (n = 16), and individuals not being found during this re-contact visit (n = 10). Further details are provided in Figure 1. Study participants’ flowchart. CC: chronic condition. FU: Follow-up.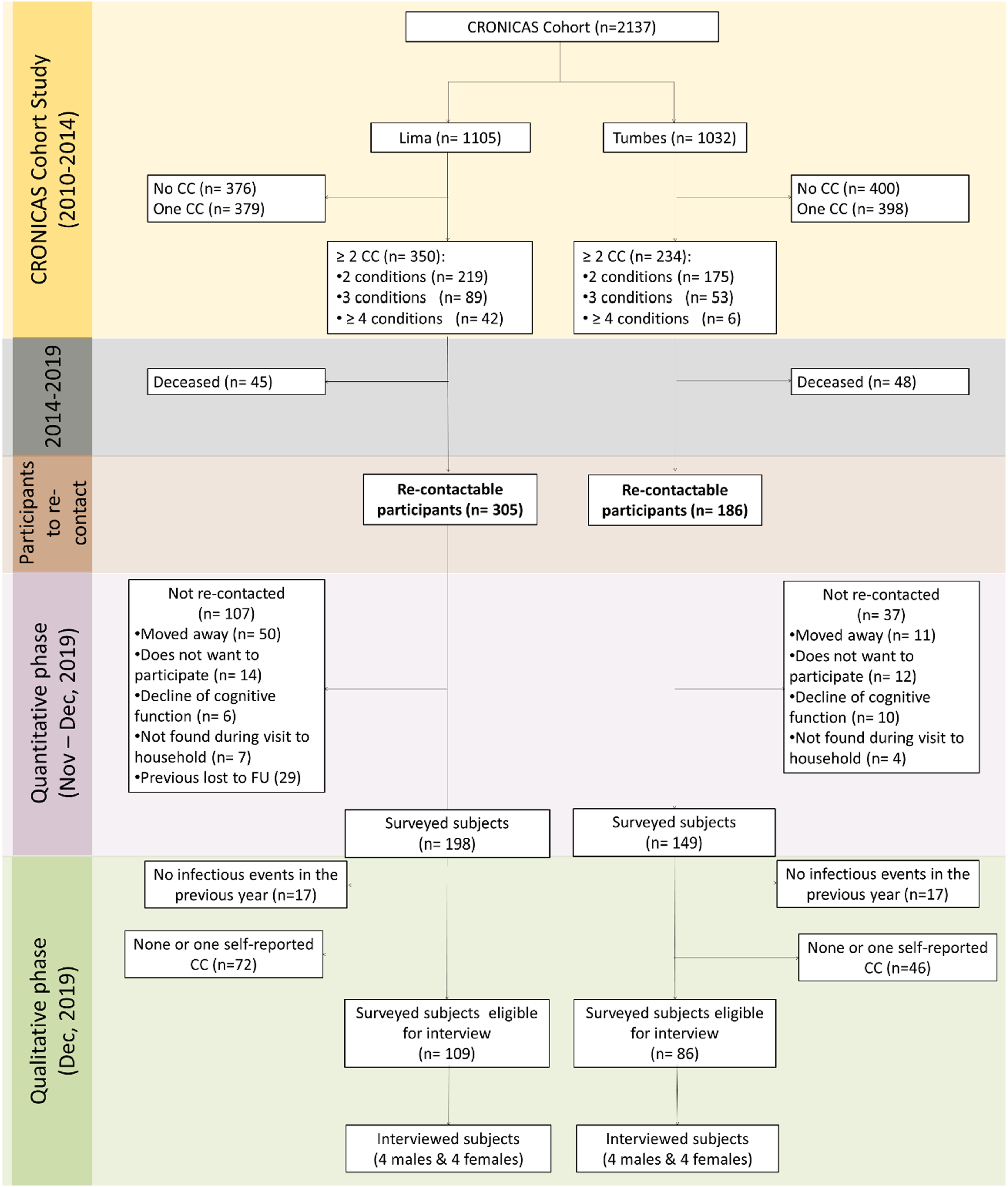
Socio-demographic characteristics and chronic conditions of participants surveyed in the present study from Lima and Tumbes (2019).

*Non-parametric test. ¥ Results may not add due to missing values.
Current insights on health perspectives in chronic and acute conditions: findings from re-contacted participants – Qualitative phase
The qualitative analysis identified five prominent themes reflecting participants' perspectives on health related to chronic and/or acute conditions: general health, chronic diseases, acute infectious diseases, healthcare system, and quality of life (
After conducting a qualitative data analysis, five central themes emerged reflecting participants' perspectives on health: general health, chronic diseases, infectious diseases, healthcare system, and quality of life. Participants, primarily older adults, reported physical discomfort related to chronic conditions or ongoing acute infectious events such as fatigue and headaches. In Lima, those with chronic respiratory issues experienced improvements in their health due to seasonal changes, while some in Tumbes reported respiratory complications alongside diabetes or cardiovascular conditions. Managing multiple chronic conditions proved complex, involving changes in perspectives they have about the diseases, increased healthcare visits, consistent medication adherence, and ongoing adoption of a healthy lifestyle. Diagnosis often occurred during routine check-ups for initial conditions or after significant health episodes, leading to varied timelines for their diagnoses. Following diagnosis of chronic conditions, most participants promptly began treatment and monitoring for them in healthcare settings, while a minority delayed treatment initiation. The level of importance participants assigned to managing their chronic conditions varies based on the severity of the disease and their duration of living with the diagnosed condition. Some prioritized treatment for the most bothersome or concerning condition, sometimes overlooking other co-existing conditions. Patients with diabetes and/or cardiovascular diseases attended regular medical check-ups approximately every two months. Conversely, individuals with chronic respiratory issues sought medical attention mainly during severe episodes. Over time, some patients decreased their routine check-up frequency due to emotional fatigue or access to home measurement devises like glucometers and blood pressure monitors. In Lima, two out of five participants with diabetes owned glucometers, while one participant in Tumbes has access to a family member's blood pressure monitor. While initially accepting pharmacological treatment for chronic conditions, adherence tends to decline over time as the number of medications increases due to multimorbidity. Reasons for treatment delay or abandonment include difficulty accepting the diagnosis, medication, drug intolerance (particularly with diabetes treatments), and prioritization of medications for more severe conditions. Notably, participants with Type 2 diabetes prescribed insulin express resistance and reluctance to use it due to fear of injections or perceived complications. Some participants adhere to pharmacological treatments alongside various traditional plants, juices, or dietary supplements, particularly prevalent in Lima, irrespective of their chronic conditions. Some integrate these traditional options into their regimen alongside medications, especially when managing multiple medications. For example, a participant with a history of cancer, diabetes, and chronic obstructive pulmonary disease incorporates a variety of alternative products into their regimen, from fruits to insects. Specifically for diabetes management, individuals consume leaves of certain plants and fruits to “lower blood glucose”. Popular choices include passion fruit juice, parsley water, hibiscus tea, or moringa infusions. Among participants with chronic respiratory issues, two individuals—one from Lima and one from Tumbes—use Chuchuwasi, a medicinal plant from the Peruvian Amazon that is commonly consumed as an alcoholic maceration, as an alternative to medications to relieve and treat bronchial problems and cough. Chronic conditions require individuals to make lifestyle changes, including adjustments to diet and physical activity in addition to pharmacological treatment. Despite efforts to implement these changes, they often prove difficult to sustain over time. Adhering to dietary recommendations proved challenging, especially for individuals with diabetes and/or cardiovascular diseases. Eleven participants modified their diets based on healthcare advice or personal observations of not healthy foods. Others reduced certain food items like sugar, salt, and flour, although not always due to chronic condition management. Limited information about the foods they can consume due to their chronic conditions, as well as their prices, were challenges for sustained dietary changes. Despite medical recommendations, intentional physical activity is minimal among participants. Only one maintains a frequent exercise routine, while another exercises daily. Inactivity is attributed to chronic cardiovascular or respiratory conditions, acute infections, leg or foot ailments, or fatigue from daily activities. Half of the participants continue working, but with reduced intensity. Three work consistently, while others ceased work due to severe health conditions advised by doctors. Retirees and homemakers make up the non-working group. Living with chronic diseases prompts diverse shifts, from habits and customs to complex changes in life perspectives and social interactions. Many participants have stopped or reduced alcohol and tobacco use, leading to altered social dynamics and increased isolation. Mood changes are common, with one feeling like a different person than before diagnosis. Others gain new perspectives on life and relationships, prioritizing health processes and embracing understanding and acceptance of diseases. Participants with multimorbidity faced challenges in recalling the exact number of acute infectious diseases experienced in the past year but highlighted significant infections due to severity or impact on daily life. Despite chronic conditions, they reported experiencing one to four types of acute infections, with gastrointestinal, respiratory, and urinary tract infections being most common. Responses varied on infection trends compared to previous years, with half perceiving increased acute infections and the rest split between consistent or decreased rates of acute infectious events. Many noted acute infections as more severe than previous episodes, with causes attributed to age, diet, work, stress, climate, and environmental factors. Few participants associated multimorbidity directly with increased acute infection risk, indicating varied perceptions and understanding of their acute and chronic health conditions. Participants typically respond to acute infections by first visiting drug stores to purchase prescribed medications for acute infections or attempting home remedies before resorting to healthcare facilities, depending on the severity of symptoms. Some self-medicate at the onset of recurring acute infections to prevent escalation. Participants seek formal healthcare when initial self-care measures prove ineffective. Limited access to specialist appointments and monthly healthcare visits under public insurance lead to out-of-pocket expenses for additional care and medications. When purchasing medications, participants prioritize disclosing chronic conditions to pharmacists to avoid potential drug interactions. Those with previous prescriptions for similar acute infections adhere to prescribed regimens. Managing multiple medications during acute infections requires careful organization or temporary suspension of certain medications to mitigate adverse effects. Infections typically did not lead to radical lifestyle changes for individuals with multimorbidity, although participants noted significant impacts on health, including physical weakness and decreased motivation during acute infection symptoms. During acute infectious illnesses, dietary adjustments are minimal compared to the changes required by their existing chronic conditions. Participants reported consuming light foods and avoiding fats, fish, and cold items based on the type of acute infection they have. Despite discomfort or lethargy, participants engaged in work or household activities even during illness, demonstrating resilience despite symptoms. Acute infectious episodes notably affect mood, with some participants describing irritability, low spirits, and heightened concern about their condition. Managing multimorbidity and acute infectious conditions can be complex and exhausting. Despite resorting to simpler treatments like home remedies, participants seek healthcare for accurate diagnoses and effective treatments. One individual in Tumbes avoids treatment for his chronic conditions and going to medical appointments due to fear of a new dire diagnosis. Participants prefer known places for care, often visiting the same centres for chronic and acute infectious diseases, turning to hospitals in emergencies, and occasionally opting for private clinics. Participants in the study often encounter challenges when attempting to schedule medical appointments at public facilities, with wait times varying, ranging from queuing at 4am to be seen at 7am same day, to waiting anywhere from 1 to 3 months for a specialist medical appointment, based on the speciality required. Similarly, accessing services presents obstacles, particularly for speciality consultations, prompting some individuals to seek private healthcare alternatives to address urgent medical needs or avoid lengthy wait times. While participants describe the process of accessing healthcare as cumbersome, their perceptions change significantly based on the quality of care received. Physicians who demonstrate empathy and provide effective treatment are highly regarded by participants, fostering loyalty and patient satisfaction despite longer waiting periods for appointments. Regarding nursing staff, opinions are divided: some view them positively for their kindness, while others see them negatively as a barrier between doctors and patients, providing poor treatment. Individuals covered under public or social health insurance systems benefit from free medications provided by public health institutions. However, some participants opt to purchase medications from external drug stores due to stock shortages or personal preferences for brand-name drugs. The perceived effectiveness of generic medications is a topic of discussion, with individuals often preferring brand-name medications when financially feasible. Following a diagnosis, individuals seek information from diverse sources, including healthcare providers, television programs, and trusted friends or family with medical expertise. Despite varied information sources, most participants prioritize and trust the guidance provided by healthcare professionals, valuing medical expertise even in brief consultation settings. The quality of life for individuals with multimorbidity is significantly impacted by both declining health and changes in their relationships with family and friends due to their chronic conditions. The physical and emotional burden of managing multiple illnesses affects their overall well-being and alters their social and family dynamics, often leading to limitations in social activities and interactions. Individuals with multimorbidity are aware of varied perceptions from others regarding their chronic and acute infectious health conditions. Some experience sympathy and solidarity, while others encounter indifference, highlighting the complexities of social interactions in the context of managing multiple health challenges. Health conditions lead participants to face significant social limitations, resulting in reduced participation in social gatherings due to dietary restrictions, physical limitations, and managing depression alongside multimorbidity. Despite these challenges, one participant stands out for maintaining normal social and family engagement, albeit without alcohol. Fourteen participants receive crucial support from family caregivers, mainly adult children, who assist in managing their parents' healthcare needs. However, two participants lack caregiving support due to factors like estrangement from their children or their children's busy lives, preventing them from relying on family assistance for their health care. Individuals living with chronic or acute infectious conditions often experience physical discomfort and sensitivity that significantly impacts their daily lives. Managing multiple health conditions presents challenges in treatment approaches, healthcare accessibility, medication adherence, and necessary lifestyle adjustments over time. Early detection of asymptomatic or unrecognized chronic conditions is difficult, and the initiation and continuity of treatment vary based on perceived condition severity. Lifestyle changes recommended for chronic conditions are hard to maintain consistently, often due to limited physical activity caused by health constraints. Social isolation resulting from lifestyle changes and health limitations further affects quality of life. However, the support of family caregivers is essential for individuals with multimorbidity. Acute infectious diseases, experienced by all participants, mainly affect the gastrointestinal, respiratory, and urinary systems, with perceived severity increasing compared to previous years. Accessing healthcare is hindered by appointment delays, which differ between public and private facilities. Participants generally have positive perceptions of healthcare providers but mixed views towards nursing staff. The preference for brand-name medications over generics highlights the need for improved patient education and communication with healthcare providers. Managing multimorbidity presents significant challenges for healthcare systems due to deficiencies in user access and the provision of adequate care, especially for individuals with chronic conditions. As diseases progress, the complexity of treatments and necessary care intensifies, posing additional obstacles to effective management. These findings underscore the nuanced complexities involved in addressing chronic and acute infectious health conditions in clinical practice.Results
Overall health
Chronic diseases
Response to diagnosis
Approach to healthcare facilities
Treatment
Use of traditional and alternative medicine
Changes in daily life following diagnosis of chronic conditions
Changes in diet
Changes in physical activity
Changes in work activity
Other changes
Acute infectious diseases
Response to acute infection
Approach to healthcare facilities
Treatment
Changes in daily life after acute infection
Changes in diet
Changes in work activity
Changes in mood
Health care system
Access to healthcare facilities
Perception of received care
Access to medications and effectiveness
Information seeking
Quality of life
Perception of health condition by others
Family and social limitations
Caregiver support
Summary remarks
The interaction between chronic conditions and acute infectious events was perceived differently among participants, with some individuals acknowledging the interplay between these health factors, while others did not perceive any interaction. Acute infections, such as respiratory or urinary tract infections, frequently exacerbated existing chronic conditions, leading to heightened discomfort, diminished quality of life, and increased healthcare demands. Managing acute infectious events alongside chronic conditions posed significant hurdles in treatment adherence, symptom management, and overall healthcare navigation as reported by some individuals interviewed. Participants commonly reported experiencing physical weakness, emotional strain, and disruptions in daily routines during acute infectious events, highlighting the complex interplay between acute and chronic health issues. These findings accentuate the critical importance of adopting comprehensive care strategies that holistically address both acute and chronic aspects of individuals' health conditions within clinical practice and healthcare delivery systems. For more details, please refer to
Participants’ awareness, treatments, and perceptions and experiences related to chronic conditions
We observed strong evidence of difference (p<0.05) between the mean number of chronic conditions detected during the CRONICAS Cohort Study on the re-contacted individuals (2.5 ± 0.8 in Lima, and 2.2 ± 0.5 in Tumbes), and the self-reported mean number of chronic conditions of the re-contacted individuals on this evaluation (1.7 ± 1.2 in Lima and 1.8 ± 1.2 in Tumbes). Hypertension (57.4%) and type 2 diabetes (32.9%) were the most frequently self-reported conditions. Moreover, in Tumbes, a higher number of participants with multimorbidity self-reported having hypertension and type 2 diabetes compared to those in Lima. Conversely, conditions such as asthma, bronchitis, depression, and cancer were more frequently self-reported among participants in Lima than in Tumbes (Table 3).
During the interviews, some participants evidenced low awareness of their chronic conditions.
I: ... How did you know you had high glucose levels? P: I got 165 [mg/mL of blood glucose levels], but I didn't pay attention to it. I went to Lima and... I got 165, the same as here, but... what can I say, it was my carelessness and the doctor's carelessness that he sent no pills for high glucose.
I: And, how long ago did you know you have diabetes? P: Three years ago, but I was told before that, but I didn’t want to… I didn’t want to… accept or listen, I was calm until the doctors spoke to me seriously; then, at that moment, I just kind of became aware, right? Seeing that diabetes is a disease that so many people die of, their legs are cut-off… then… I became aware, and I understood I also have diabetes and now, I accept it.
Additionally, during the current survey, all participants who reported having a chronic condition were asked about their current treatment, whether pharmacological or not, their adherence and perception of medications. The participants with type 2 diabetes, hypertension, and COPD, were the ones who more frequently reported having a treatment either pharmacological or not, with 86% (98/114), 79% (157/199), and 75% (3/4) of positive responses, respectively. However, only 10% (10/98), 12.1% (19/157), and 33.3% (1/3) of them, respectively, reported being adherent, that is, following the treatment as per the doctor's recommendations. During the interviews, when exploring if the treatment was taken as their doctors suggested, participants mentioned that at the beginning, they followed clinicians’ instructions; however, as time went on, and due to the number or physical size of the pills, their adverse effects, or because of the onset of other diseases, their adherence decreased: Lima, Woman #2 P: ... sometimes I want to put down those darn pills, because they are really big. I: Which ones? P: The one for diabetes, metformin. Ah!! They are really disgusting, they are bitter, and I have to take so many pills, sometimes... I get sick with my throat... I have to take my pills for diabetes, my pills for... they hurt my stomach, too… I: How many pills do you have to take a day for diabetes? P: I have to take two, three, four big pills. I: At what times? P: After breakfast, I have [...] Metformin. Then I take metformin for lunch with the little one, and one at night before I go to bed. Lima, Woman #3 P: […] the disease is already difficult (sobs), they prescribed me a lot of pills that my body rejects. Why does it reject it? I feel heartburn, I feel like I want to vomit, and I cannot resist that. I pray every day because of the pills that I take, for the ones for [blood] pressure, because I went to the cardiologist, and he told me: ‘you have to take them’... I: And the other pills? P: Sometimes I take the ones for diabetes; sometimes, as I say, my body does not resist them, the only thing [that my body resists] is traditional medicine.
Regarding the healthcare received for their chronic conditions, not all patients have the same experience when attending a health facility. In some quotes, we can notice differences between attending a Ministry of Health facility (Lima, Woman #1), which provides a broader (in terms of reach) and more generic health service to the entire population, irrespective of affiliation or employment status, compared to an ESSALUD facility for the wage-earning population (Lima, Woman #8) which operates as a social security system funded by contributions from formal workers and their employers, and that offers healthcare specifically to this demographic and their dependents. This situation might impact how patients experience their conditions. Lima, Woman #1 I: When you go to the hospital, what is the care like? P: Ufff, you have to be lucky to get an appointment. For example, right now I have been told that there are no appointments for endocrinology until next year. Imagine, I need to see the endocrinologist and there are no appointments... I: When was your last appointment with the endocrinologist? P: It was in… December, last year (1 year ago), the doctor sent me to pick up some medicines, telling me: “I'm going to give you [medication] for 3 months…” Lima, Woman #8 I: And is it easy or difficult to get an appointment? How complicated can it be? P: If you are right there [during an appointment], I mean, you go to the doctor and the doctor gives you your next appointment. I only [have delays] getting appointments for dental and ophthalmology, which does take a long time. For example, I have been given an appointment for dental, I think, after half a year because it is difficult to get it.
Relationship between acute infectious events and multimorbidity among re-contacted participants
Characteristics of interviewed participants.

Acute infections occurred in the previous 12 months by type of chronic conditions in subjects with multimorbidity.

aNumber and percentage of participants that self-reported having at least one acute infectious event.
bCumulative incidence: number of events per person in the previous 12 months. Pulmonary group includes asthma, chronic bronchitis, and COPD. CV and metabolic group include hypertension, peripheral artery disease, heart failure, stroke and diabetes. Mental includes depression and alcohol disorder. Others group includes depression and alcohol disorder.
In the qualitative phase, the interviewees' perceptions were diverse, with some participants thinking there was a link between their chronic conditions and acute events, whilst for others, such links were not present, or they were not clear. Tumbes, Woman #7 I: What do you think the infections are due to? P: I think they are because of the kidney problem or gastritis that I have. It may be because of that. Tumbes, Woman #5 I : Do you feel that these (chronic) conditions have predisposed you to infections? P: Well… where do they come from? Why do people get these infections? I: What do you think? What could it be due to? P: I think it must be because of too much work, that’s what I think, right? Because I have worked for thirty-five years, and then I got that infection… Lima, Woman #1 I: And what do you think could be the cause of your infections? P: I don't know, I asked the doctor that. The doctor tells me that infections are due to diabetes itself… I: What do you think? P: I think it's because of a lot of dryness …and the wound cream they prescribed for me is also expensive, and sometimes I don't have the money….
Healthcare help-seeking behaviours, experiences and perceptions about acute infectious events among re-contacted participants
Seeking for help during an acute infectious event in subjects with multimorbidity [n (%)]

aNumber of subjects that self-reported having at least one acute infectious event in the previous 12 months.
Some interviewees described these preferences, while some explained that they did not go to a healthcare service because of their fear to be diagnosed with a new disease, others mentioned that it is because of the time it may take to get an appointment with the specialist. Lima, Man #5 I: [...] What do you do when your stomach suddenly hurts, or you have diarrhoea... What do you do immediately? P: [...] I tell my wife that my stomach hurts, and she says “Drink hot water, perhaps it is because of the cold”, if I'm going to the bathroom very often [...] my wife says: I have to prepare some muña [local herb] tea. I drink it... If it does nothing, then I go to the hospital. Lima, Woman #1 P: Sometimes I do not, let's say, go to the hospital immediately [when feeling sick], because I am afraid to go and that they might diagnose me with a new disease. So I buy myself an Uropol, a Diclofenac and I take them. Then, perhaps, that's why I don’t get better because this time they [health professionals] are trying and trying to cure me, but they can’t.
I: […] At some point, when you had a respiratory or urinary infection, have you had to go to see the doctor? P: No, I go to the drugstore and ask only the pharmacist what pill I need to take, and I take it.
Discussion
We have explored relationships between chronic conditions and acute infectious events in two sites of the CRONICAS Cohort Study in Peru. A previous report on this cohort using cross-sectional data from the baseline evaluation showed that there was a substantial proportion of subjects with multimorbidity, 23% and 15% in Lima and Tumbes, respectively.20,22,23 However, we found that this percentage increased to 32% and 23%, respectively, at 30 months from initial enrolment into the study. Among the re-contacted participants, we identified low awareness of chronic conditions, poor adherence to chronic conditions treatment, and varying perceptions when inquired about their healthcare attendance experiences. When evaluating the occurrence of infectious events, respiratory and gastrointestinal infections were the most reported. Approximately two-thirds of participants with multimorbidity who reported such events mentioned that they either did not seek help or only visited a drugstore. In drugstores, individuals typically receive advice from trained or qualified professionals, although in some cases, it is the shop owners or salesclerks with no formal education on medications who assist customers in their visits. While it is important to note that in many cases, seeking medical assistance may not be necessary, due to the complexity of multimorbidity care, there is a possibility that many of the people with several chronic conditions may indeed require healthcare facility assistance. Here we reported that less than a third of participants do so. Furthermore, when we focus on specific categories of chronic conditions, particularly those associated with groups (namely cardiovascular and metabolic, pulmonary, mental health, cancer, or reflux groups), we observe that in cases where multimorbidity involves conditions like cancer or reflux, the cumulative incidence of chronic conditions exceeds those seen in instances with a pulmonary condition. Moreover, among individuals with 3 or more chronic conditions, the cumulative incidence of acute infectious events was observed to be slightly higher compared to those individuals with 2 chronic conditions. However, the confidence intervals did overlap, preventing from drawing definitive conclusions about this difference.
From the qualitative phase, we detected varying perceptions among participants regarding the interaction between chronic conditions and acute infectious events. While some individuals acknowledged this relationship, others did not see any connection. Acute infections, such as respiratory or urinary tract infections, were reported to exacerbate existing chronic conditions, leading to increased discomfort, diminished quality of life, and greater healthcare demands. A study highlighted poor adherence outcomes among outpatients with respiratory infections who were treated with antibiotics. 24 This finding emphasizes the challenges associated with managing acute infectious events within the context of chronic conditions, highlighting the complexities of healthcare navigation and treatment adherence in these populations. In addition to treatment adherence, managing acute events alongside chronic conditions presented significant challenges in symptom management and overall healthcare navigation, as certain participants emphasized. Physical weakness, emotional strain, and disruptions in daily routines during acute episodes were commonly reported, illustrating the intricate relationship between acute and chronic health issues. These findings highlight the importance of implementing comprehensive care strategies that address both acute and chronic aspects of individuals' health conditions within clinical practice and healthcare delivery systems. Additionally, as the rising prevalence of chronic conditions poses significant public health challenges, self-management strategies, i.e. home-based or community based, emphasizing patient responsibility and collaboration with healthcare providers, offer promising approaches for treating chronic conditions 25 and could also assist individuals with chronic conditions in managing acute infectious diseases effectively.
Of the entire group of individuals with multimorbidity across the two study visits, we found that 93 individuals died between the last follow-up and this evaluation. Of the re-contactable participants (n= 491) we were able to re-contact and survey approximately 71% of subjects. When comparing the CRONICAS Cohort Study baseline data of the individuals with multimorbidity surveyed in this evaluation vs those not surveyed, as expected, we found that those not surveyed were older and had a lower educational level. In addition, of those not surveyed, almost 40% of subjects had died, reinforcing the idea that multimorbidity and mortality are associated with lower education levels and older age. 26 These findings raise the possibility that the observed patterns may be even worse in these groups we could not re-contact. It is worth mentioning that we were not able to re-contact a greater proportion of people with peripheral artery disease and bronchitis. As previously reported, peripheral artery disease is associated with 7.05 years of potential life lost in southern Latin America 27 while chronic bronchitis is associated with 2.2 higher risk of all-cause mortality in subjects younger than 50 years old. 28 Additionally, if we consider that the presence of chronic bronchitis is associated with a higher number of respiratory infections, 29 this might have resulted in an even higher cumulative incidence of acute events if all individuals with chronic bronchitis had been re-contacted. In high-income countries, 5-year mortality can be predicted by multimorbidity and this might be mediated by disability; 30 however, similar estimations are needed for low- and middle-income country settings as the compounded effects of multiple challenges could be linked to a higher occurrence of negative health outcomes.
The observed discrepancy in the current analysis, in which fewer chronic conditions were identified in this assessment compared to previous data collected during the CRONICAS Cohort Study can be attributed to our reliance on self-reported information for medical conditions. It is well-documented that individuals may be unaware of their diagnosis for certain chronic conditions, resulting in underreporting.31–33 This phenomenon is particularly relevant when considering chronic conditions that may exhibit milder or asymptomatic manifestations such as early stages of hypertension, depression or type 2 diabetes, the most prevalent ones in our population. Concerning acute infectious diseases, the most commonly reported events were respiratory and gastrointestinal infections. However, what is striking is the cumulative incidence of acute events reported among individuals with multimorbidity over the last 12 months, which varied from 2 to 18 times that previously reported for adults in general.34–36 Considering that having multimorbidity is associated with substantially higher healthcare utilization, 37 this information should be taken into account by policymakers to improve health services and facilities, not only articulating the different medical specialities for multimorbidity but also incorporating an infectious conditions component to it, including navigation support to patients given the complexities of chronic conditions. Responses addressing these needs for acute care among people with multimorbidity may also improve the low help-seeking behaviour observed in our participants.
Suffering from more than one chronic condition implies more complex needs in terms of healthcare, 37 with repercussions in self-management and support. 38 This leads to a greater burden on staff and health systems, for which it is already a challenge to treat a single chronic condition. This was reflected in the results of Moth et al. in which general practitioners consider that care for people with multimorbidity is demanding and that it cannot be delegated to health personnel not prepared for these combinations of conditions, 38 which may influence the attitude of people with multimorbidity towards seeking help in primary care centres. One of the most critical health challenges in Peru and other similar resource-constrained settings is the high fragmentation of the health system, even at the institutional level, and insufficient and heterogeneous economic resources which lead to large regional gaps in healthcare access and quality.39,40 At the population level, this translates to a lack of confidence regarding quality healthcare, accessibility, and health system responsiveness when individuals seek care and support from the healthcare system. This could potentially explain why we observed that only approximately 30% of individuals with multimorbidity visit a healthcare facility during an acute infectious event, as indicated in our study. In such a context, especially considering that individuals with multimorbidity require sustained healthcare support for their diverse health conditions, 37 the multiple medications they are prescribed, 41 and the potential interactions that may arise upon adding new medication, 42 particularly in response to an acute condition, the situation becomes more complex.
While research on chronic conditions is ongoing, health leaders should take proactive measures to adapt health systems, implementing both new and established prevention and treatment strategies, and rigorously monitor and evaluate processes to gain insights into the factors contributing to the successful implementation of these strategies. Some recommendations encompass enhancing the training of health workers to proficiently manage and communicate with individuals affected by the complexity of multimorbid conditions,43–45 particularly focusing on addressing the specific needs of certain populations, such as elderly patients or those with complex combinations of conditions, depending on the healthcare settings where they receive care. 23 Such adjustments are crucial to ensuring that health systems can effectively address the challenges posed by the interaction of acute infections with multimorbidity and offer comprehensive and tailored care to diverse patient groups.
Strengths and limitations
The present study has both strengths and limitations. This is a mixed-methods study carried out in two resource-constrained sites, where the prevalence of multimorbidity is high, providing unique insights into the participants’ experience of the occurrence of acute infectious events among people with multimorbidity. Also, leveraging existing cohort studies and introducing new assessments can be advantageous because we already have our study population identified. Nonetheless, it is crucial to acknowledge certain limitations in our study. This study's focus on 12 specific conditions only may be considered a limitation, as some investigations have included a broader spectrum of chronic conditions. 46 The rationale behind the selection of these conditions is based on taking advantage of the CRONICAS cohort, specifically, individuals who were detected, either by measurement or self-report, with two or more chronic conditions in the cohort assessments to re-contact them. The study began data collection in 2010 and used the list of 12 conditions in order to study non-communicable chronic conditions in different contexts in Peru. 20 A subsequent study of the chronic cohort already focused on multimorbidity only based on the baseline evaluation, considered these same 12 conditions as well. 23 Also, self-reported data, used in our research, may be susceptible to recall bias or challenges in accurately recalling medical history and experiences. This aspect could potentially impact the accuracy of the data, particularly in older populations. Furthermore, acknowledging the persistent challenge of cognitive decline in Peru 47 and its potential influence on participants' responses due to memory bias becomes significant in interpreting our study's findings. In a similar manner, reliance on self-reported physician diagnoses for gastroesophageal reflux could also pose a limitation. Differentiating between chronic and acute forms of this condition was not explicitly addressed during the CRONICAS Cohort Study. However, it is noteworthy that the medical definition for diagnosis refers to a chronic or recurrent condition. 48 Apart from using appropriate instruments, the pivotal role of well-trained field workers is essential. Their deep understanding of the community's context, social norms, language, and population dynamics fosters effective two-way communication. In this study, fieldworkers were community members who had participated in multiple evaluations within this population. This ensured that communication gaps were not a significant issue. Also, enhancing data collection methods is crucial for obtaining detailed reports and reducing the cognitive burden of recalling experiences. Streamlining processes and utilizing innovative tools like digital surveys and automated systems can improve data accuracy and participant engagement, benefiting both research and practical applications. 49 To address recall-bias for infrequently reported health conditions known to be prevalent, e.g., COPD, adopting a more comprehensive data-collection approach could be considered to have a better self-report of these conditions. This is also particularly relevant for short-term conditions like acute infectious diseases, which often have minimal lasting effects. One option is utilizing national surveillance data; however it's important to acknowledge the potential for underreporting, incomplete data, lack of specificity regarding health conditions, and the exclusion of marginalized populations. 50
Conclusions
Leveraging data from the existing CRONICAS Cohort Study, the present work is the first to explore the occurrence of acute infectious diseases among people with multimorbidity in urban and semi-urban sites in Peru, showing that certain type of conditions has higher cumulative incidence of infectious events as well as there being a higher incidence of acute infections in those with a higher number of chronic conditions, i.e. two chronic conditions vs three or more chronic conditions. However, it is worth mentioning that confidence intervals overlapped. In addition, we explore experiences and perceptions about health care related to multimorbidity and acute infectious events, evidencing low awareness of their multimorbidity and a shared preference between going to a drugstore or not seeking help when an acute event occurs. The complimentary qualitative information generated expanded our understanding of the frequency of acute infections, and perceptions related to pharmacological treatment and health-seeking behaviours. The qualitative analysis reveals complex challenges for older adults managing chronic and acute infectious conditions, including worsened discomfort and healthcare needs due to acute infections. Participant perceptions of the interaction varied underscoring difficulties in managing acute events within chronic conditions. These findings highlight the critical need for comprehensive care strategies in clinical practice, emphasizing tailored interventions for symptom management and treatment adherence. Taken together, this study advances the body of knowledge around the challenges of multimorbidity in low-resource settings, with particular emphasis on the role of acute infections adding to the existing large burden of multimorbidity experienced by patients and their households.
Supplemental Material
Supplemental Material - Multimorbidity and acute infectious diseases in urban and semi-urban settings in Peru: A mixed-methods study
Supplemental Material for Multimorbidity and acute infectious diseases in urban and semi-urban settings in Peru: A mixed-methods study by Cecilia Anza-Ramirez, Lizzete Najarro, Antonio Bernabé-Ortiz, Francisco Diez-Canseco, Edward Fottrell, Ibrahim Abubakar, Akram Hernández-Vásquez, Rodrigo M. Carrillo-Larco, John R. Hurst, J. Jaime Miranda in Journal of Multimorbidity and Comorbidity
Footnotes
Author contributions
ABO, EF, IA, JRH, and JJM participated in the conceptualization of this study and obtained funding. CAR, ABO, FDC, EF, IA, JRH, and JJM participated in the design of this study. CAR coordinated the project and wrote the first draft of the manuscript with inputs from LN and JJM. CAR and LN coordinated data collection. CAR and LN conducted the analysis of the study. All authors revised the manuscript and provided critical inputs. All authors read and approved the final version of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ‘Multi-morbidity and infectious diseases: Strengthening links between the UK and Peru’ was supported by an Institutional Links grant, grant IDs 413495350 (UK) and 223-2018 (Peru), under the UK-Peru partnership. The grant was funded by the UK Department for Business, Energy and Industrial Strategy and FONDECYT via CIENCIACTIVA/CONCYTEC and delivered by the British Council and the Newton-Paulet Fund.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.