
Abstract
Purpose
Understanding variation in multimorbidity across sociodemographics and social drivers of health is critical to reducing health inequities.
Methods
From the multi-state OCHIN network of community-based health centers (CBHCs), we identified a cross-sectional cohort of adult (
Results
Among 642,730 patients, 28.2% were Hispanic/Latino, 42.8% were male, and the median age was 48. The median MWI was 2.05 (IQR: 0.34, 4.87) and was higher for adults over the age of 40 and American Indians and Alaska Natives. The regression model revealed a higher MWI at younger ages for patients living in areas of higher deprivation. Additionally, patients with social risks had a higher MWI (3.16; IQR: 1.33, 6.65) than those without (2.13; IQR: 0.34, 4.89) and the interaction between age and social risk suggested a higher MWI at younger ages.
Conclusions
Greater multimorbidity at younger ages and among those with social risks and living in areas of deprivation shows possible mechanisms for the premature aging and disability often seen in community-based health centers and highlights the need for comprehensive approaches to improving the health of vulnerable populations.
Introduction
Multimorbidity, commonly defined as the co-occurrence of chronic conditions, is associated with numerous poor health outcomes (e.g., higher health care utilization, mortality).1-7 Generally, the focus on multimorbidity research and intervention has been on adults 65 years old or older, limiting our understanding of the early development of multimorbidity in younger age groups, such as young or middle-aged adults.8-15 This is a critical knowledge gap because identifying individuals who are at a higher risk of developing multimorbidity at a younger age is essential for effective primary prevention to advance health equity.
The maldistribution of health-promoting resources in the United States has disadvantaged racial and ethnic minoritized populations and increased the negative influence of social drivers of health. These social drivers of health include structural factors such as neighborhood deprivation and individual-level social risks, such as food and housing insecurity.16,17 They are associated with a higher prevalence of morbidity, particularly among minoritized racial and ethnic populations.18-23 While the mechanism of these differences are due to the confluence of physiological, structural, and environmental factors, research has begun to uncover how structural and interpersonal barriers due to race/ethnicity and socioeconomic status result in biological disruption and accelerated aging.24-26 There is evidence that this process is expressed by the earlier onset of multimorbidity with some studies indicating that racial/ethnic minoritized groups experience this burden at an earlier age.27-33 However, this research remains limited by its narrow focus on a small number of chronic diseases, oftentimes fewer than 10, and an outsized focus on older adults.27-33
In this study we sought to examine the relationship between sociodemographics, social drivers of health, and multimorbidity among patients aged 25 and over receiving care at the nation’s largest network of primary care community-based health centers (CBHCs). We hypothesize that minoritized racial/ethnic populations (i.e., non-White), those living in neighborhoods with high deprivation, and those with social risks will have a higher burden of multimorbidity, and at younger ages, compared to non-minoritized racial/ethnic groups, those in areas of less deprivation, and those without social risks.
Methods
Study design and setting
The data for this cross-sectional study comes from the OCHIN network of CBHCs. OCHIN is a nationwide network of CBHCs who all use OCHIN Epic © electronic health record (EHR) providing the largest collection of community health data in the country.
Participants
Our study population included patients with at least one visit in 2019, 2020, or 2021 to an OCHIN member clinic that had at least 2,000 primary care visits in 2019. This criterion was applied to ensure that these clinics are providing routine primary care where these chronic conditions would be captured. A patient cohort of 1,131,478 patients was created from 218 unique clinics in the OCHIN network. Our final analytic cohort was limited to patients 25 years old or older (n = 801,266), without missing sex (n = 800,718), without missing/unknown/other race (n = 706,041), without missing ethnicity (n = 678,541), with a valid address match to a census tract (n = 642,730) (Supplemental Figure 1). The characteristics of this final study cohort, n = 642,730, were consistent with that of all potential patients that met the age criteria (Supplemental Table 1). Our examination of social risk was limited to patients with a social risk screening (31.7%; n=203,669) in any domain. As shown in Supplemental Table 2, there were important differences in the population screened for social risks with a higher proportion of Black/African American, Hispanic/Latino, and females being screened.
Exposures: Sociodemographic and social drivers of health
There were two main categories of exposures of interest: sociodemographics and social drivers of health. Sociodemographic factors included age, race/ethnicity, and sex. Age was calculated in years based on the age at their latest encounter between 2019-2021. Race and ethnicity were obtained from a patient’s EHR and included the following categories: the racial categories of American Indian or Alaska Native (AIAN), Asian, Black or African American, Native Hawaiian or Other Pacific Islander (NHOPI) and White, and ethnicity options of Hispanic or Latino or Not Hispanic or Latino. While race and ethnicity are collected separately, we combined them into a single variable. Individuals who reported being Hispanic or Latino, regardless of race, were identified as such. Therefore, the racial groups are comprised of non-Hispanic or Latino individuals (e.g., White is Non-Hispanic White). OCHIN member clinics generally have high rates of race/ethnicity collection and reporting.
Social drivers of health operate at both the neighborhood and individual level. Given that previous work 34 has illuminated the incongruence of these measures – and their different conceptual underpinnings – we sought to examine them separately. The Area Deprivation Index (ADI)35, 36 was used to measure neighborhood level deprivation. We used the sociome R package 37 to obtain the Census-tract level ADI estimates from the 2019 American Community Survey based on the patient’s most recent geocoded address from the study period (2019-2021), using the entire nation as the reference level. We then divided the study population into quintiles, as has been done previously. 38 Individual-level social risks include the following domains: child/family care, education, employment, financial strain, food insecurity, health literacy, housing instability, housing quality, relationship safety, social isolation, transportation insecurity, and utilities insecurity. Members of the OCHIN network use existing social risk screeners,39, 40 or develop their own targeted questions to assess a patient’s social risks during a clinical visit.
Outcome: Multimorbidity weighted index
We used the Multimorbidity Weighted Index (MWI), developed by Wei et al.41-43 as our measure of multimorbidity for this study. This index weights over 80 different chronic conditions (Supplemental Table 3) based on their association with changes in the Short Form-36 physical functioning scale where a one-point increase in MWI corresponds to a one-point decrease in physical functioning. Previous analyses have shown the MWI to be associated with physical and cognitive performance and mortality.15, 41-43 Given its large number of included conditions, previous validation, and association with physical functioning, the MWI represented the best potential index for use in this study. In addition to the MWI score, we also used the total count of the MWI conditions by patient in supplemental analyses. We used the MWI estimated from the problem list at the patient’s last visit in the study time frame (2019-2021).
Statistical analyses
The statistical analyses in this study set out to answer our two core research questions: Does multimorbidity vary by sociodemographics and social drivers of health? Is there additional variation in multimorbidity when further stratified by age? To answer these questions, we report descriptive statistics of the median and interquartile range (IQR) of the MWI, stratified by the sociodemographics and social drivers of health, and then further stratified by age group. As a sensitivity analysis, we also present the count of MWI conditions stratified by these factors. To further examine the relationship between each sociodemographic and social driver of health exposures (primary predictors) and MWI (the outcome), we conducted five separate generalized linear regression models. Despite the non-normal distribution of the MWI, a linear model was appropriate given the large sample size 44 and observing no improvement after implementing transformations 45 and examining the residuals. We adjusted for biological sex and age, with the estimate representing the effect of a 5-year increase in age. Each model included an interaction between age and the primary predictor. The goal of these models was to adjust for age and sex to understand the relationship more precisely between sociodemographics and social drivers of health and multimorbidity. We present the effect size with a 95% confidence interval, with an alpha of 0.05. SAS version 9.4 was used for data cleaning, while R version 4.2.2 was used for analysis and visualization.
Ethical and regulatory approvals
This study was approved, including a waiver of informed consent, by the Case Western Reserve University Institutional Review Board (STUDY20210933).
Results
Study Population Characteristics.

1Reported racial groups are all Non-Hispanic/Latino.
Sociodemographics
Distribution of Multimorbidity Weighted Index, by Sociodemographics and Social Drivers of Health.

1Reported racial groups are all Non-Hispanic/Latino;
2Patient-reported social risks (e.g., food insecurity, housing insecurity) from individual screening.
Linear regression models of the relationship between sociodemographics and the Multimorbidity Weighted Index.
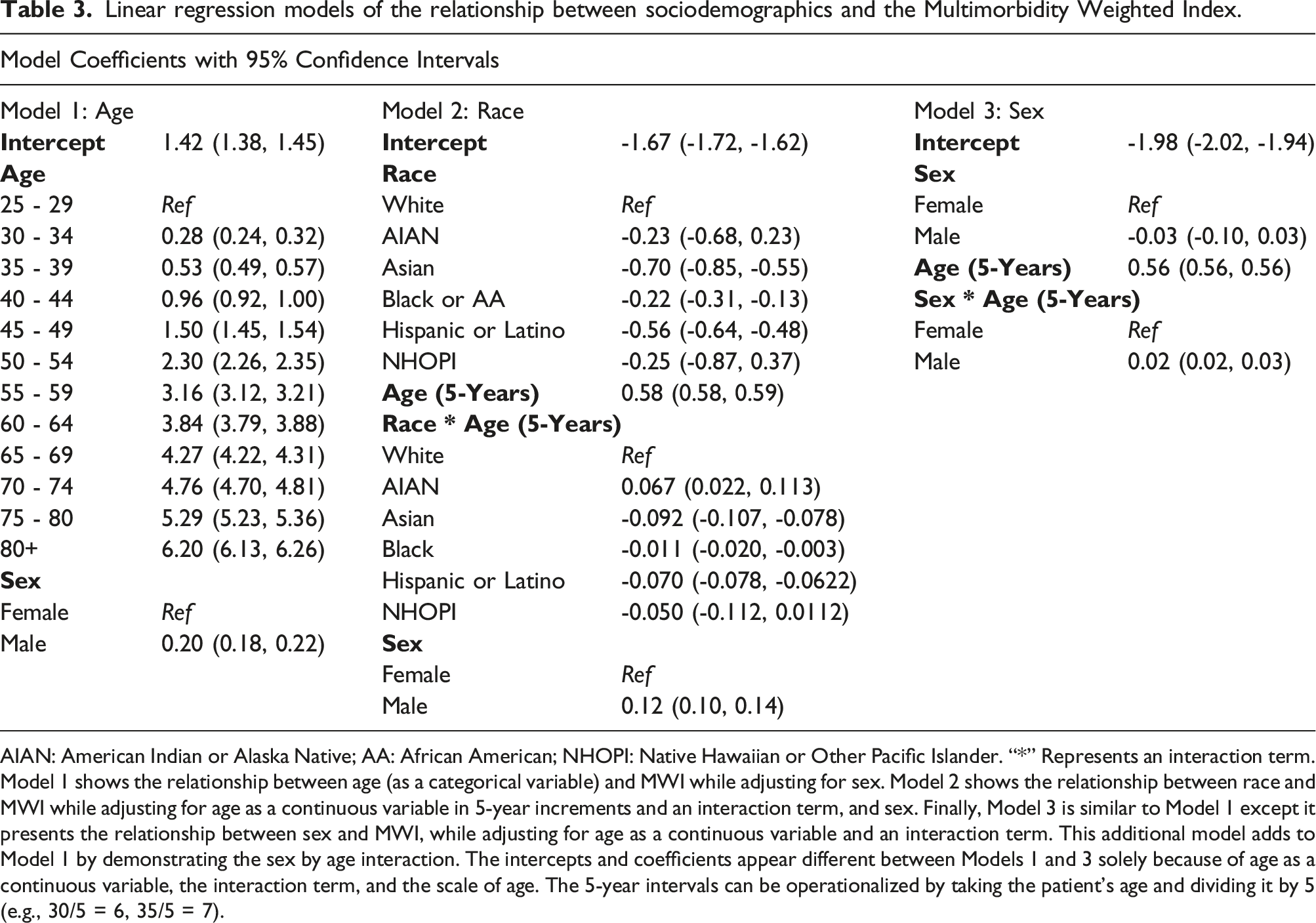
AIAN: American Indian or Alaska Native; AA: African American; NHOPI: Native Hawaiian or Other Pacific Islander. “*” Represents an interaction term. Model 1 shows the relationship between age (as a categorical variable) and MWI while adjusting for sex. Model 2 shows the relationship between race and MWI while adjusting for age as a continuous variable in 5-year increments and an interaction term, and sex. Finally, Model 3 is similar to Model 1 except it presents the relationship between sex and MWI, while adjusting for age as a continuous variable and an interaction term. This additional model adds to Model 1 by demonstrating the sex by age interaction. The intercepts and coefficients appear different between Models 1 and 3 solely because of age as a continuous variable, the interaction term, and the scale of age. The 5-year intervals can be operationalized by taking the patient’s age and dividing it by 5 (e.g., 30/5 = 6, 35/5 = 7).

Distribution of Multimorbidity Weighted Index by Sociodemographics of Interest (race/ethnicity, sex, age).
Social drivers of health
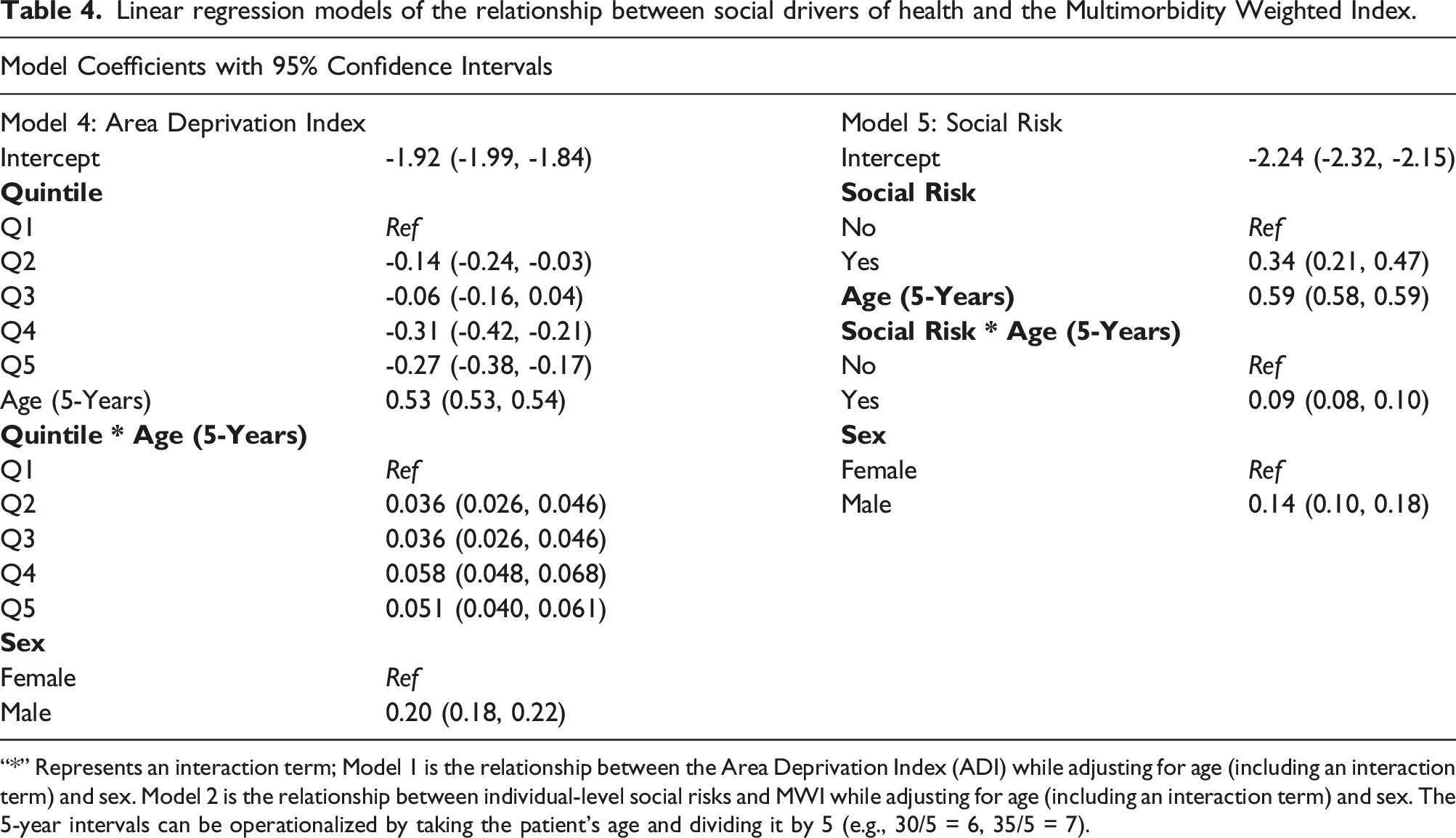
The relationship between neighborhood deprivation and multimorbidity was more nuanced than that of sociodemographics. Individuals in the third quintile of neighborhood Area Deprivation Index (ADI) had the highest median MWI of 2.29 (IQR: 0.34, 5.17) (Table 2 and Figure 2). When stratified by age the MWI remained relatively constant until after age 55 (Supplemental Table 4, and Supplemental Figure 5). The regression model confirmed this relationship and showed that higher quintiles of ADI were associated with higher MWI (Table 4). This analysis indicated a slight variation in the relationship between age and multimorbidity based on neighborhood deprivation (Table 4, Supplemental Table 4, Supplemental Figure 3). Distribution of Multimorbidity Weighted Index by Social Drivers of Health (Area Deprivation Index Quintile and Social Risks). Linear regression models of the relationship between social drivers of health and the Multimorbidity Weighted Index. “*” Represents an interaction term; Model 1 is the relationship between the Area Deprivation Index (ADI) while adjusting for age (including an interaction term) and sex. Model 2 is the relationship between individual-level social risks and MWI while adjusting for age (including an interaction term) and sex. The 5-year intervals can be operationalized by taking the patient’s age and dividing it by 5 (e.g., 30/5 = 6, 35/5 = 7).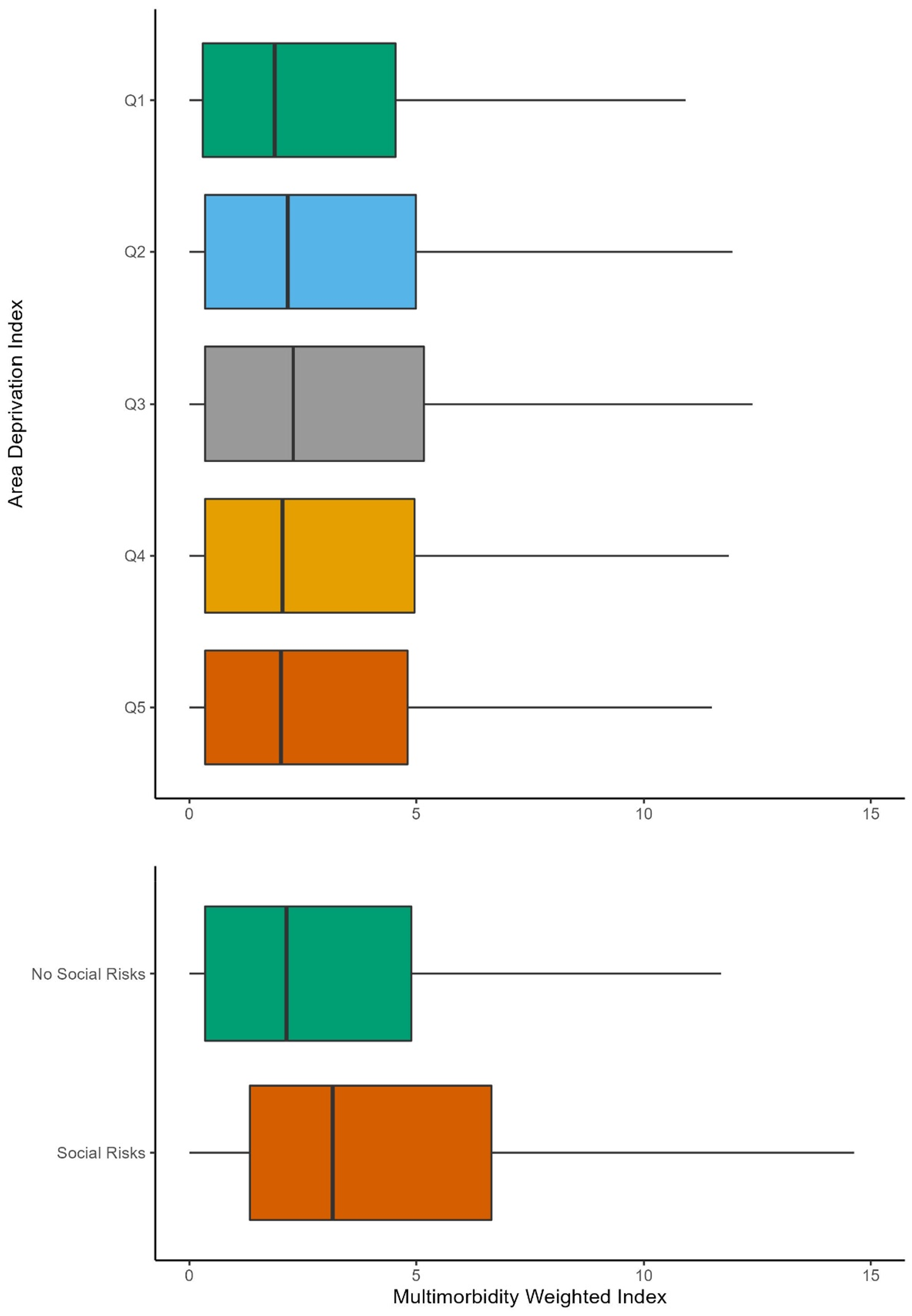
Perhaps the clearest finding was that those individuals with social risks had higher multimorbidity than those without. Of the 203,669 individuals who were screened for social risks, 43.3% (n = 88,210) reported a social risk. Among those individuals reporting at least one social risk, the median MWI was 3.16 (IQR: 1.33, 6.65) versus 2.13 (IQR: 0.34, 4.89) among those who were screened but reported no social risks (Table 2, Figure 2). This difference was also seen in our regression model interaction with age (0.09, 95% CI: 0.08, 0.10) suggesting a higher burden at younger ages (Table 2, Supplemental Table 4, Supplemental Figure 4).
Supplemental analysis: Count of conditions
Our supplemental analysis examining the count of conditions revealed largely similar findings (Supplemental Table 6). Specifically, younger ages (< 40 years old) generally had a median of 1 condition. After age 40, this increased to 2 and then finally to 3-4 conditions in the oldest age groups. The patterns across sociodemographics and social drivers of health were consistent with what we observed using the MWI score.
Discussion
This study identified variation in multimorbidity across sociodemographics and social drivers of health among patients seen at primary care CBHCs, most notably showing higher multimorbidity among AIAN individuals and those individuals with social risks. A few of these relationships further varied by age, suggesting a higher multimorbidity burden at younger ages for AIAN individuals, males, those in areas of high deprivation, and those with social risks.
Variation in multimorbidity by sociodemographics and the social drivers of health
Our study examined multimorbidity across a much wider age span than previous studies and found a low burden of multimorbidity among patients ages 25-40, with it increasing steadily after age 40. Our population had a lower distribution of chronic conditions (median: 1.79) compared to previous studies on older age groups and from studies from non-clinical settings such as the Nurse’s Health Study (medians of roughly 4-7).41-43 This may indicate that the commonly used chronic conditions do not capture the totality of CBHCs patients’ health status. For example, the MWI may be less sensitive for this study population given it was created using a population of patients that may not represent those who are seen at CBHCs. When we explored the sum of the conditions, instead of the weighted index, we observed similarly little variation across younger ages, sociodemographics, the social drivers of health (Supplemental Table 6). This would suggest that the limited variation was not solely an artifact of the weighting used. Most of the included conditions develop over time and are not as sensitive to younger populations that may experience a greater burden of acute conditions and symptoms before the development of a chronic condition. Overall, these findings contribute to the growing body of work that seeks to understand variation in multimorbidity across a wider age range and among minoritized populations.
Our findings related to variation in multimorbidity by the social drivers of health raise several important points. First, we observed very little variation in multimorbidity across the ADI. This finding was particularly interesting given the literature highlighting the higher burden of chronic conditions among patients who reside in neighborhoods with high deprivation. 18 When we examined individual-level social risk there was a much clearer difference in multimorbidity between those with social risks and those without, with having social risks increasing the MWI by 0.09 in our model. Despite only a modest increase, a one-point increase in MWI corresponds to a one-point decrease in physical functioning, this finding is more consistent with previous literature and nonetheless reinforces the importance of understanding both the neighborhood- and individual-level mechanisms that may create the association between these social drivers of health and multimorbidity. These seemingly disparate findings also echo the poor congruence between neighborhood deprivation and individual-level social risks, 34 and the perhaps higher homogeneity among patients seen at CBHCs. While CBHCs serve patients regardless of the ability to pay, their focus on ambulatory primary care may result in an underrepresentation of patients with social risks whose care is fragmented and occurs in other health care settings (e.g., emergency department).
Potential interpretations of paradoxical findings
The simplest interpretation of our findings is that there is a low multimorbidity burden and very little variation by sociodemographics and social drivers of health especially among the relatively younger age and largely low socioeconomic status patients who are seen at CBHCs. However, this interpretation is inconsistent with previous work in other populations with low socioeconomic status, 18 and inconsistent with biological evidence of the effect of deprivation and stress24-26 creating a paradoxical finding. We posit a further explanation that existing measures of multimorbidity are not capturing the totality of health needs of this population. Many multimorbidity indices are designed for older adults and may not always include some of the most common chronic health problems for younger adults such as allergies, asthma, and some mental health conditions. Additionally, recent work has demonstrated poor alignment of areal-level measures of social drivers of health and individual-level social risks demonstrating the risk of the ecological fallacy and may help explain some of this paradox. 46
Implications for practice, research, and policy
While the measured burden of multimorbidity among patients seen in an ambulatory primary care setting may be low, it is well documented that the clinical complexity is high.47, 48 This and other paradoxical findings of our study highlight that while providers should consider the influence of sociodemographics’ and social drivers of health on multimorbidity, current models of multimorbidity are unable to explicate this nuance. Care should be taken when using these existing measures for risk stratification or prediction in primary care settings. The results from this study also call attention to the need for additional research on how developed indices of multimorbidity may not fully capture the morbidity burden among younger populations served in community-based health center settings and develop specific indices that are more sensitive in these populations. Finally, health care policies are exploring incorporating the social drivers of health in risk adjustment and reimbursement.49,50 As these policies emerge, this study highlights the need to identify other potential measures that may better stratify both the neighborhoods and individuals who are most at risk for a higher burden of multimorbidity and its poor consequences.
Limitations and considerations
There are several limitations of this study. Foremost, the comparisons made within this study are among CBHC patients served by clinics in the OCHIN network. CBHCs serve communities that have been most economically and socially disadvantaged. This may reduce the amount of variation compared to other data sources that include patients who are not seen at CBHCs. Second, this work did not follow these patients longitudinally but instead described the distribution in a cross-sectional cohort. Third, the study period included the time of the COVID-19 pandemic which may have caused rapid changes in health and social risks. While we did not explicitly examine this in our study, future studies will specifically examine these questions. Finally, there is not uniform social risk screening among patients. This highly variable screening limits our understanding of the precise impact of social risks, and the observed bias in screening 51 (Supplemental Table 2) potentially biases our understanding of these relationships in this study sample. These limitations present clear opportunities for future work that would examine these trends among a more socioeconomically diverse sample of patients and examine these trends longitudinally to understand how specific sociodemographics or social drivers of health may be associated with the earlier development of multimorbidity at younger ages.
Conclusions
In a large national primary care community-based health center population, variation in multimorbidity, measured via the Multimorbidity Weighted Index, across sociodemographics, social drivers of health, and age among adult patients is less than was anticipated, but sociodemographics and social drivers of health are associated with a higher multimorbidity burden at younger ages. Future work must continue to assess how we can measure and operationalize the health needs of younger patients at community-based health centers, including developing multimorbidity indices for younger, diverse, primary care populations so that we can and how this higher burden of multimorbidity can be mitigated to improve health outcomes and advance health equity.
Supplemental Material
Supplemental Material - Variation in multimorbidity by sociodemographics and social drivers of health among patients seen at community-based health centers
Supplemental Material for Variation in multimorbidity by sociodemographics and social drivers of health among patients seen at community-based health centers by Wyatt P Bensken, Suparna M Navale, Brenda M McGrath, Nicole Cook, Yui Nishiike, Gretchen Mertes, Rose Goueth, Matthew Jones, Anna Templeton, Stephen J Zyzanski, Siran M Koroukian, and Kurt C Stange in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under award number R01AG074946. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This work was conducted with the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is led by OCHIN in partnership with Health Choice Network, Fenway Health, and Oregon Health & Science University. ADVANCE is funded through the Patient-Centered Outcomes Research Institute (PCORI), contract number RI-OCHIN-01-MC.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under award number R01AG074946. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.