
Abstract
Background
Ageing of the population increases the prevalence and coexistence of many chronic diseases; a condition called multimorbidity. In Finland, information on the significance of multimorbidity and its relation to the sustainability of healthcare is scarce.
Aim
To assess the prevalence of multimorbidity, the transitions between patient groups with and without multiple diseases and the associated healthcare cost in Finland in 2017–2019.
Methods
A register-based cohort study covering all adults (n = 3,326,467) who used Finnish primary or specialised healthcare services in 2017. At baseline, patients were classified as ‘non-multimorbid’, ‘multimorbid’ or ‘multimorbid at risk’ based on the recordings of a diagnosis of interest. The costs were calculated using the care-related patient grouping and national standard rates. Transition plots were drawn to observe the transition of patients and costs between groups during the two-year follow-up.
Results
At baseline, 62% of patients were non-multimorbid, 23% multimorbid and 15% multimorbid at risk. In two years, the proportion of multimorbid patients increased, especially those at risk. Within the multimorbid at-risk group, total healthcare costs were greatest (€5,027 million), accounting for 62% of the total healthcare cost of the overall patient cohort in 2019. Musculoskeletal diseases, cardiometabolic diseases and tumours were the most common and expensive chronic diseases contributing to the onset of multimorbidity.
Conclusion
Multimorbidity is causing a heavy burden on Finnish healthcare. The estimates of its effect on healthcare usage and costs should be used to guide healthcare planning.
Introduction
Ageing of the population increases the prevalence and coexistence of many chronic diseases; a condition called multimorbidity. Globally, wide disparities in the prevalence estimates (ranging from 13%–72% in the general population) exist due to varying multimorbidity definitions and methodologies.1,2 According to the WHO definition, ‘multimorbidity is the coexistence of two or more chronic conditions in the same individual’, and it is the most used definition in scientific literature. 3 However, some definitions also include acute conditions or use the cut-off point of three or more. The number of medical conditions included in the measures of multimorbidity has been shown to vary widely, ranging from a few conditions to hundreds. 4 Also, there are differences in the methods to define multimorbidity, starting from the simple counting of diseases to more complex clustering and in data sources (i.e. register data and self-reports) between the previous studies. 5 Due to these differences, it has been difficult to compare findings across populations and to develop solutions to tackle this growing public health problem which challenges western countries and the sustainability of their social and healthcare systems.
Previous research has shown that patients with prevalent multimorbidity are often older and have increased risk factor levels, high use of health services, more hospitalisations and higher mortality compared with healthy populations or patients with only one chronic condition. 6 Further, higher rates of primary and specialised care visits, medication use, emergency department visits and hospital admissions in patients with multiple chronic conditions have all been connected to rising healthcare expenses. 7 With the increasing prevalence of multimorbidity, healthcare expenses and resource consumption rise dramatically, even exponentially. The National Institute for Health and Care Excellence (NICE) has published a guideline on assessing and managing patients with multimorbidity. 8 In accordance with the NICE Guidelines, the Finnish Medical Society Duodecim has published the Current Care Guidelines, which aim to improve the care of people with multimorbidity and is intended as a basis for treatment decisions. 9 These guidelines indicate the situations in which the identification of patients with multiple diseases and the individual planning of treatment are essential. Such situations include patients with both physical illnesses and mental health problems, patients with frailty, patients who use many health services, patients with multiple medications and patients who have difficulties managing their everyday lives. These multimorbid patients are at higher risk of premature death, hospitalisation and increased costs than others.8,9
Managing multimorbidity is difficult for patients and healthcare systems, and multimorbid patients frequently require primary and secondary care services. Existing healthcare services are not adequately designed to meet the challenges of multimorbidity; they have often been focused on the care of single diseases. 10 Social and healthcare systems that can manage the emerging issues associated with multimorbidity and related costs are urgently needed. Country-specific knowledge about the prevalence of multimorbidity and estimates of its effect on healthcare utilisation and costs are required to guide healthcare planning and improve care quality. In Finland, information on the significance of multimorbidity and its relation to the sustainability of healthcare is scarce. Therefore, this study aims to assess the prevalence of multimorbidity, the transitions between patient groups with and without multiple diseases, and associated costs in Finnish healthcare in 2017–2019.
Data and methods
The data were extracted from the Finnish Care Registers (Care Register for Health Care and Register of Primary Health Care Visits) from 2015–2019. The registers provide information on a patient’s gender, age, and healthcare contacts. Each individual contact with a healthcare professional is recorded in the register, including information about the type of contact and diagnoses (ICD and ICPC codes). The study cohort includes all adults aged 18 years or older who used Finnish primary or specialised healthcare services in 2017. Altogether, 3,326,467 patients were included in the analyses.
Classification of chronic diseases
Calderón-Larrañaga et al. 11 provided a list of chronic conditions using ICD-10 codes and grouped all four-digit level codes into broader categories to measure multimorbidity in the older population. We modified the existing disease list using three-digit ICD-10 codes and added the corresponding ICPC-2 codes. In addition, we excluded the three-digit codes which included certain sub-codes for an acute version of the condition. Based on the codes, we identified all diagnoses of interest from the Care Registers and created broader disease groups.
Previously, Fränti et al. constructed a multimorbidity network covering all Finnish primary and specialised care services patient visits in 2015–2018 and related diagnoses represented as blocks of ICD-10 codes.12,13 Using the network data, we ensured that relevant diseases were comprehensively identified and grouped to assess multimorbidity. Furthermore, a multimorbidity measure was created based on these 34 disease groups and used for the analysis to understand the impact of multimorbidity on healthcare utilisation and costs in Finland. Supplementary Table 1 presents the disease groups and codes used to identify chronic diseases.
Multimorbidity status
Multimorbidity status (non-multimorbid, multimorbid or multimorbid at risk) at baseline was determined based on the recordings of a diagnosis of interest using Finnish Care Register data. For the analysis, patients who were free from all selected diseases or had only one disease (i.e. disease or diseases from one disease group) were defined as ‘non-multimorbid’ at baseline. Patients with co-occurrence of two or more chronic diseases (i.e. diseases from ≥ 2 disease groups) were defined as ‘multimorbid’. ‘Multimorbid patients at high risk’ were patients with both physical illnesses and mental health problems, multimorbid patients with age-related physical weakness or disabilities (ICD-10 code R54; ICPC-2 codes: A28, N28, P28, Z28), or multimorbid patients who used emergency care services three times or more per year. In this study, the concept of “multimorbid patient at risk” was adopted from the guidelines.8,9 In the guidelines, the definition of multimorbid patients at risk includes a slightly broader set of criteria than we were able to use due to the limited availability of information from the register.
The non-multimorbid, multimorbid and multimorbid at risk patients were defined at the moment of their first visit to the health services in 2017. Only those who had at least some kind of a contact to health services in 2017 were included in the analyses. Data from prior years was used to capture the actual multimorbidity status at baseline. Those who had previously (between the years 2015-2017) or at that visit diagnoses of two or more chronic diseases were regarded as multimorbid. Similarly, those who fulfilled the criteria of being at risk by the first visit in 2017 were regarded as multimorbid at risk patients. Follow-up of each individual continued until death from any cause or the end of the two-year follow-up period. The date of death was received from the National Register of Causes of Death.
Statistical analysis
Frequencies and percentages were used to describe the baseline characteristics in patient groups with and without multimorbidity and diseases contributing to the onset of multimorbidity and related costs in this patient cohort. The costs were calculated also in patient quartiles based on healthcare costs. The counting of costs started on the date of the first visit in 2017 and costs of all contacts were counted for 730 days (2 years) after the first visit in 2017. The costs were calculated using the care-related patient grouping and national standard rates. The costs for hospitalisations and outpatient hospital visits were based on the NordDRG patient grouping definitions, which use the International Classification of Diseases 10th revision (ICD-10) codes and the Finnish version of the Nordic Classification of Surgical Procedures (NCSP) codes for diagnostic and treatment procedures. The cost weights for DRG-grouped hospital discharges and outpatient hospital visits are calculated using large national samples of individual-level cost accounting data from Finnish hospitals by the national authorities. The unit cost estimates for community care bed days were derived from the national price list for unit costs of healthcare services in Finland and used with the individually calculated length-of-stay data. The primary care contacts were grouped according to the contact type (visit, call, home care, e-messages) and the healthcare professional. Each primary care contact type was priced according to the national price list for unit costs. 14 Prices were adjusted to the 2017 level using the healthcare price index by Statistics Finland.
Transition plots were drawn to observe the transition of patients and costs between non-multimorbid, multimorbid, multimorbid at-risk and dead categories during the two-year follow-up.
Results
Baseline characteristics in patient groups with and without multimorbidity.

Multimorbidity transitions and associated healthcare costs during the two-year follow-up
We found a considerable number of patients moving from the non-multimorbid group to multimorbid and multimorbid at-risk groups during the two-year follow-up (Figure 1). After the follow-up, altogether, 45% (1,498,627) of patients were non-multimorbid, 26% (877,802) were multimorbid, and 25% (846,966) were multimorbid at risk of poor outcomes, and 3% (103,072) had died. During the follow-up, the observed transitions between patient groups with and without multimorbidity were similar among men and women. However, multimorbidity was more prevalent among women than among men. In 2019, 60% of multimorbid patients were women, and 40% were men (data not shown). Transitions of patients (n) with and without multimorbidity in the 2017 patient cohort during the two-year follow-up.
In this prevalent patient cohort, the proportion of multimorbid patients at risk increased the most during the follow-up (15% in 2017 vs 25% in 2019). It was also the costliest patient group, costing €5,027 million and accounting for 62% of the total healthcare cost of this patient cohort in 2019 (Figure 2). Correspondingly, 18% (€1,504 million) of the total healthcare cost was associated with healthcare usage among multimorbid patients and 13% (€1,038 million) among non-multimorbid patients in 2019. In 2017, the proportions of healthcare cost were 35% (€2,819 million), 29% (€2,403 million) and 36% (€2,929 million) in the non-multimorbid, multimorbid, and multimorbid at-risk groups, respectively. Costs (€) associated with multimorbidity transitions in the 2017 patient cohort during the two-year follow-up.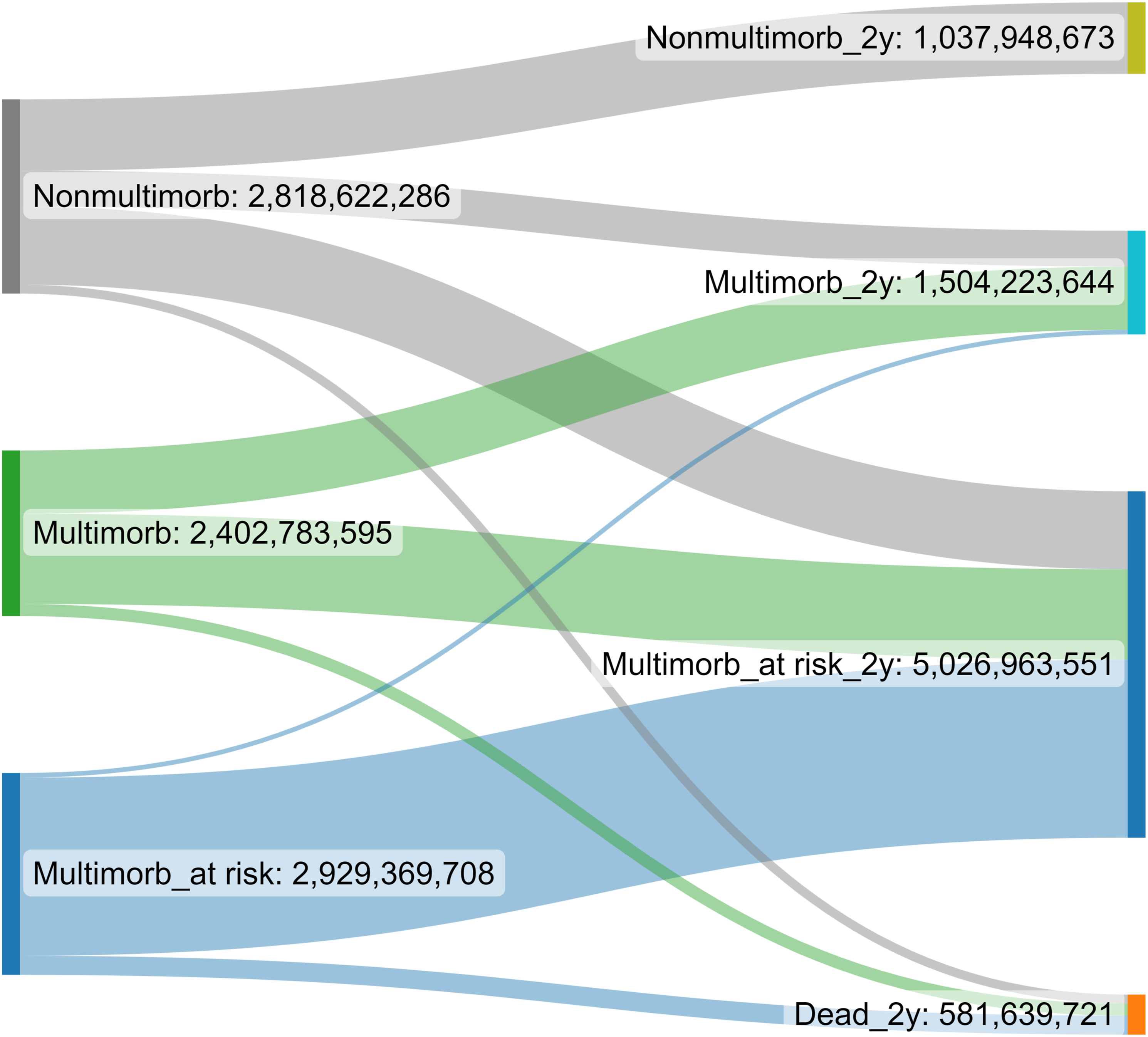
Incidence of multimorbidity among non-multimorbid patients during a 2-year follow-up in the 2017 patient cohort
The most common patient groups becoming multimorbid and related healthcare costs during the two-year follow-up in the 2017 patient cohort.

Out of the patients with hypertensive diseases at the baseline, 56% (22,473/39,805) became multimorbid, followed by the proportions of the patients with arthrosis (54%; 14,696/27,228), diabetes (53%; 23,285/43,776), and other diseases of the heart and pulmonary circulation (52%; 16,821/32,126). Of patients with back diseases at the baseline, 43% (47,000/109,452) became multimorbid, causing the highest cumulative healthcare costs (€107 million) during the two-year period. The second highest cumulative two-year healthcare costs were €80 million in the group of patients with diabetes, and the third highest cumulative costs were €79 million in the patient group with cancer and in-situ carcinomas (Table 2).
The most common and expensive disease groups resulting in multimorbidity among non-multimorbid patients during the two-year follow-up in the 2017 patient cohort.

Overall, different musculoskeletal diseases, cardiometabolic diseases, and tumours were the most common chronic diseases among non-multimorbid patients in 2017, contributing to the onset of multimorbidity and causing huge expenses during the two-year follow-up.
Discussion
Summary of findings
This study is one of the first to estimate the significance of multimorbidity and its relation to Finnish healthcare sustainability using the register data covering all adults who used primary or specialised healthcare services in Finland in 2017. This study provides information on the prevalence of multimorbidity in Finnish healthcare, the transitions between patient groups with and without multiple diseases and associated healthcare costs during the two-year follow-up.
At baseline almost two-thirds of the patients were non-multimorbid, 23% were multimorbid, and 15% were multimorbid at risk. During the two-year follow-up, a considerable number of patients moved from the non-multimorbid group to multimorbid and multimorbid at-risk groups. The proportion of multimorbid patients at risk increased the most; from 15% to 25% in two years. They had also the greatest total healthcare costs (€5,027 million), accounting for 62% of the patient cohort’s overall healthcare spending in 2019. During the follow-up, the most common chronic diseases contributing to the onset of multimorbidity and causing huge healthcare expenses were musculoskeletal and cardiometabolic diseases and tumours.
Findings in context
Marked variations have been shown to exist among multimorbidity studies in terms of methodology and findings.15,16 Despite the variability, the results from the studies evaluating the effect of multimorbidity on healthcare utilisation and cost have shown to be relatively consistent. The review of Lehnert et al. included 35 international studies. It indicated a positive association between multimorbidity and healthcare use outcomes (physician visits, hospitalisations, use of medications) and healthcare cost outcomes (medication, out-of-pocket, total healthcare expenditures), 17 and later the review of Wang et al. confirmed their findings on the economic burden of multimorbidity. 18 Also, a systematic review of the UK literature showed that multimorbidity was associated with increased primary and specialised healthcare use and related costs (total costs, hospital costs, primary and dental care use, emergency department use, and hospitalisations). 19 In addition, it has been shown that healthcare use and costs tend to increase with the number of chronic conditions.7,17,20 Several studies have also demonstrated that particularly multimorbidity with mental health disorders or frailty is associated with higher levels of health service use and a higher cost.19, 21–23
A systematic review by Kudesia et al. determined the incidence of multimorbidity and the order in which chronic conditions accumulate to result in multimorbidity. 24 Of the 36 included studies, five analysed the accumulation of chronic conditions. In accordance with our findings, hypertensive and heart diseases and diabetes were the most common starting conditions resulting in later multimorbidity. Cerebrovascular diseases, mental health illnesses, chronic pain, osteoarthritis, cancer and hypercholesterolemia were reported as second or third conditions resulting in multimorbidity. Also, back pain is associated with an increased likelihood of comorbidity in previous studies.25, 26 However, starting conditions contributing to multimorbidity may vary by age. The study of Ashworth et al. found that coronary heart disease and diabetes were more common as starting conditions in those over 65, while depression was more common in those under 65 years old. 27 All ages are affected by low back pain, which is a major leading contributor to the burden of disease. 28
Recently, Tran et al. conducted a meta-analysis of 15 multimorbidity studies aiming to explore the cost of specific, most frequently reported, disease combinations in U.S. healthcare. 29 Based on the results, there are differences in costs for treating different disease combinations. The least expensive to manage were disease combinations involving hypertension, and the most expensive were those with cancer and mental health conditions. However, the cost difference for treating these combinations may vary significantly between countries because of the different healthcare systems. Stokes et al. aimed to examine the potential of defining multimorbidity clusters impacting secondary care costs in England. 30 They found that all combinations containing chronic kidney disease and hypertension, or diabetes and hypertension, made up a significant proportion of total secondary care costs. Similarly, Fränti et al. performed a cluster analysis of diagnoses using data from 58 million patient visits in Finnish primary and secondary healthcare. 12 Based on their results, the total costs were the highest (€2.3 billion) in the cluster, including cardiovascular and metabolic problems. In our study, musculoskeletal diseases, cardiovascular and metabolic diseases and tumours were the costliest diseases contributing to multimorbidity in Finnish healthcare.
Strengths and limitations of this study
The main strength of this study is the register data, including all public primary and secondary healthcare visits of the Finnish adult population from 2015–2019. The Finnish Care Registers (Care Register for Health Care and Register of Primary Health Care Visits) include the ICD and ICPC-2 codes for diagnosis. Healthcare professionals record the codes in the register. The completeness and accuracy of the Care Register for Health Care providing data on both primary- and secondary-level inpatient care have been previously documented and shown to vary from satisfactory to very good. 31 The Register of Primary Health Care Visits provides additional data on outpatient primary healthcare activities. Recording activity in the register has shown to be at an acceptable level to be used for research purposes. 32 However, the registers do not include data from private health services and may have left out information on patients who prefer and can afford private health services and privately provided occupational health services. These services total about €2 billion in costs, while the costs of specialised care are about €8 billion per year, and in primary care, about €3.5 billion. 33
In addition, a comparison of the results of this study with the previous ones is challenging due to differences in data sources, methodologies, health systems and regions. Therefore, it is essential to provide country- and system-specific information on the impact of multimorbidity on healthcare utilisation and costs to inform policy and practice. 7
Implications for future research and clinical practice
The Finnish population is ageing, and the need for care is increasing. In Finland, the ongoing health and social services reform aims to centralise organisational structures to improve access to primary care and better integrate services.34,35 The ongoing reform offers possibilities to take action towards a more sustainable healthcare system, respond to the changes in care demand among the ageing population, and improve the continuity of care. This study shows how multimorbidity, especially multimorbid patients at risk, is causing a heavy burden and costs on Finnish healthcare. Furthermore, there seems to be reasonably small proportion of patients in all patient groups that cause most of the healthcare cost in that group. We would need better understanding about this phenomenon and whether service needs can be reduced among these patients. These timely results should be used to guide health service planning and targeting of preventative interventions and to deliver a good quality of care to patients with multimorbidity. Particular attention should be paid to patients with hypertensive or musculoskeletal diseases, which seem to be common conditions contributing to the onset of multimorbidity and are both conditions with prevention potential.
Supplemental Material
Supplemental Material - Multimorbidity transitions and the associated healthcare cost among the Finnish adult population during a two-year follow-up
Supplemental Material for Multimorbidity transitions and the associated healthcare cost among the Finnish adult population during a two-year follow-up by Katja Wikström, Miika Linna, Eeva Reissell and Tiina Laatikainen in Journal of Multimorbidity and Comorbidity
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the consortium project ‘Improving the Information Base and Optimising Service Solutions to Support Social Welfare and Healthcare Reform (IMPRO)’. The research was funded by the Strategic Research Council at the Academy of Finland, funding decision numbers 312703, 312707, 336325 and 336329.
Ethical statement
Consent to participate
All methods were carried out in accordance with relevant guidelines and regulations or declaration of Helsinki. The Finnish legislation (Act 552/2019) do not require informed consent for register-based research when study is solely based on registers and the study is considered to be of public health importance.
Data Availability Statement
The data that support the findings of this study are available from the Finnish Institute for Health and Welfare registers, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available due to Finnish data protection legislation. According to the legislation, register authorities give permissions to use register data including sensitive individual information (e.g., health data) to study specified research questions to named individuals who have signed a pledge of secrecy and they are not permitted to forward it to other researchers. Other researchers can apply for the data from the Health and Social Data Permit Authority Findata. Findata handles the data permit applications concerning Finnish Institute for Health and Welfare registers.
36
![]()
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.