
Abstract
Objective:
This article explores experiences of people with multimorbidity, and attempts to advance understandings of the complexity of living with multimorbidity outside the medical encounter in a social identity theoretical framework.
Method:
This is a qualitative study using individual semi-structured interviews among nine persons living with multimorbidity. The interviews are analysed inductively according to thematic content analysis.
Results:
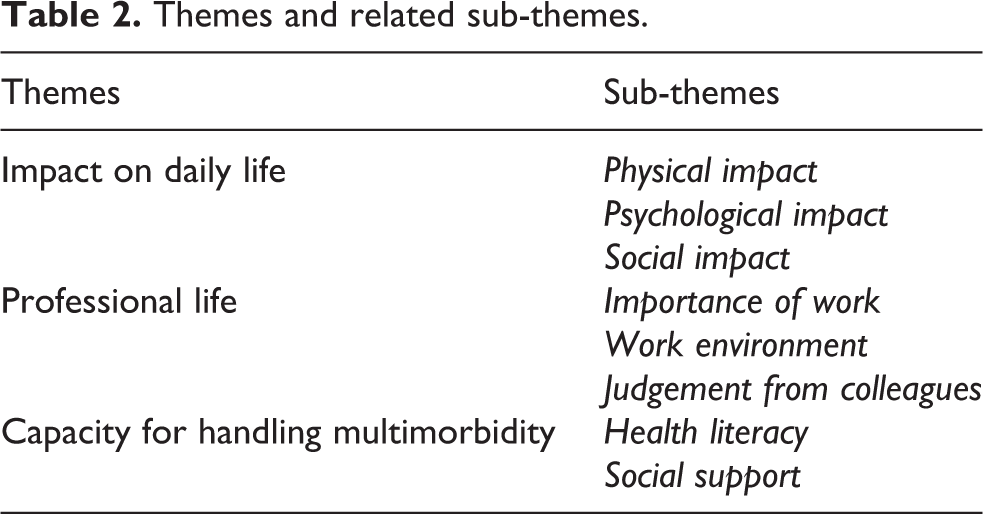
The emerging themes are: 1) Impact on daily life, 2) Professional life and 3) Capacity for handling multimorbidity. People with multimorbidity experience physical limitations and psychological distress, which limits their ability to maintain social relations and affiliation to the labour market. Accordingly, they are challenged in their ability to retain a sense of normal everyday life, which is mediated by their capacity for handling multimorbidity.
Discussion:
Multimorbidity may compromise various social identities. The complexity of living with multimorbidity is increased by an aspiration to maintain valued social identities in order to preserve a coherent sense of self and a normal everyday life. This study suggests an increased focus on individual priorities and values outside the medical encounter, and argues in favour of recognizing the conflicts that people experience as they try to balance multimorbidity with other important aspects of their daily lives.
Introduction
More and more people1–3 are living with multimorbidity, usually defined as the co-existence of two or more chronic diseases in the same individual. 4 Despite inconsistencies in regards to the definition of multimorbidity,5–7 there is generally consensus around multimorbidity being acknowledged as a complex phenomenon.8–11 It is well-established in the literature that people with multimorbidity experience an increased illness burden, such as reduced quality of life,12–14 lower functional level, 15 higher symptom burden and higher prevalence of pain compared to people with single conditions. 15 In addition, people with multimorbidity often experience an increased treatment burden, as they are involved in numerous treatment regimens due to the specialized organization of the healthcare system, which is associated with poor coordination of care, 16 fragmented treatments, 17 polypharmacy and associated potential adverse drug reactions, 18 as well as non-adherence to medical treatment. 8
A few studies point to the dilemmas people with multimorbidity experience outside the medical encounter as they balance disease and treatment with everyday life.19,20 People with multimorbidity experience disrupted daily routines,21,22 a lack of authority over their own lives,20,21,23,24 the impression of ageing prematurely 10 and difficulties with maintaining affiliation to the labour market.10,22,24,25 This may impose changes in self-identity and self-perception, 24 as well as familial and social roles, 21 which may increase the complexity of living with multimorbidity in addition to the disease and treatment burdens. Several studies highlight the continuous need to explore the complexity of living with multimorbidity from a patient perspective in order to address patients’ individual preferences, needs and goals.10,20,26–30
Social Identity Theory (SIT) is a social psychological theory focusing on how people define themselves through social groups. 31 The social nature of identity is described through three processes: 1) social categorization, 2) social identification and 3) social comparison. 32 A person can have several social identities depending on the groups that they perceive themselves as belonging to, e.g. family, friends, sports teams, religious groups and/or work teams.33–36 Social identity has various positive psychological impacts, since identification with social groups contributes to enhanced self-esteem, a sense of worth and belonging, and a sense of identity.31,33,36 A person may also experience psychological distress if his or her social identity is weakened in some way, e.g. if the person is rejected by an in-group (i.e. a collective of people who are perceived or perceive themselves to share common characteristics), leaving or changing groups, or if negative intergroup comparisons lead to stigmatization against the out-group.36,37 In this study, we use SIT to advance the understanding of the individual experience of complexity when living with multimorbidity. Previous studies have explored chronic illness and multimorbidity in relation to changes in self-identity21,22,24 and identity crisis, 38 how illness intrude on valued social identities, 39 as well as the significance of maintaining pre-existing identities and social roles 19 following illness onset. To our knowledge, no previous studies have explored the complexity of living with multimorbidity in a SIT framework.
SIT was originally developed to explain the social identity bases of prejudice, stereotyping and intergroup conflict, 31 but critical perspectives suggest that the theory has changed towards a greater focus on an individual psychology of concept formation, and argue that identity is primarily an individual cognitive process, and that the self is located within the individual.33,34,40 Acknowledging the shift of focus, we find that SIT allows an exploration of the complexity of living with multimorbidity from a social psychological perspective, yet with the original emphasis on prejudice and stereotyping as previous research have shown occurring with multimorbidity. 8 This article examines experiences of people living with multiple chronic conditions, focusing on the process of prioritizing between challenged social identities owing to multimorbidity.
Methods
Design
This qualitative study was designed by CS and KR, who both have a background in Public Health science. AJ and TW contributed with extensive research experience in the area of multimorbidity as well as backgrounds within anthropology and medicine. Initially, the aim of this study was to explore the experience of treatment burden among patients with complex multimorbidity. The focus was narrowed to adults in the working age, as most previous research on the experiences of living with multimorbidity is based on the elderly population.10,25,41 Moreover, qualitative research highlights that being affiliated with the labour market is associated with increased illness and disease burden. 20 After familiarizing ourselves with data it became clear that what was really at stake among the informants was the complexity of living with multimorbidity; and the challenge of maintaining a normal everyday life. In particular, the subject of work life became significant during the interviews. In this context, SIT was perceived as a highly relevant theory to allow an interpretation of the findings and obtain a better understanding of the complexity of living with multimorbidity.
Sampling and data collection
A total of nine informants participated in the interviews. Informants were selected based on criteria that we expected would increase complexity in multimorbidity.42,43 Thus, informants would have three or more chronic diseases from at least three different groups of diagnoses (Table 1), including referral from the General Practitioner (GP) to the secondary sector for at least one of the diseases and be in the working age, here defined as 18–65. Diagnoses for risk factors (i.e. hypertension, hypercholesterolemia and osteoporosis) were excluded, as risk factors do not necessarily target those patients who are most in need of health care. 43 Informants were recruited through different recruitment platforms according to purposeful sampling and out of convenience. Two GPs in urban settings, which the authors established contact with through a GP cluster meeting and personal network, contributed to the recruitment of eight informants. The GPs were instructed about the inclusion criteria and carefully selected eligible patients, who would be willing to participate. The GPs contacted the patient by phone, informed about the project, and patients interested in participating consented to sharing contact information. A single informant was recruited through a post on social media, which provided adequate data to reach data saturation. In addition, some informants chose to have relatives participate in the interview as well. Initially, the relatives functioned as a support for the informants, however, their engagement increased during the interviews, which contributed with additional and nuanced perspectives on living with multimorbidity. CS and KR conducted the individual semi-structured interviews (lasting 55–85 minutes) with the informants in order to explore the complexity of living with multimorbidity, following a semi-structured interview guide (see Online Appendix 1). The authors did not have any relation to the informants, and only had initial contact to the informants prior to the interviews due to practical reasons. The majority of informants were interviewed in their home in order to provide a comfortable setting for the informants, however, one informant wished to have the interview in a GP’s office for practical reasons. All interviews were recorded, transcribed and analysed using the software Nvivo.
Characteristics of informants.

* Examples: hypercholesterolemia, hypertension, BMI<18.
Data analysis
All authors contributed to the data analysis and analysed the content of the interviews inductively according to thematic content analysis. 44 The aim was to present key elements of the informants’ accounts of the multimorbidity experience. The first stage of the analysis consisted of familiarizing ourselves with the data, i.e. listening to the interviews while reading through the transcripts and observational notes. At this stage, CS and KR checked the transcripts for accuracy according to the taped recordings. Subsequently, all authors independently coded transcripts according to significant statements. The codes were organized into broader sub-themes and themes, which described the experience of living with complex multimorbidity. Whenever the authors had different perceptions of the data, CS and KR discussed the content of the code and related themes in order to achieve consensus. Disagreements were in most cases related to the quote or coding having multiple interpretations and thus some coding were included in multiple themes. At this stage, SIT was applied to unfold the themes in a theoretical analysis.
Ethical issues
The interviews were initiated with a thorough explanation of the purpose of the study. The informants then provided written and oral consent prior to the interview and were given the opportunity to withdraw from the research project at any time. Also, all informants were anonymized and identifiers changed. Transcripts were not made available to informants during the data analysis to allow for comment or correction. This decision was based on an assessment of the individual patient’s burden of disease and burden of illness, and in all cases, we found that it would be an unnecessary task to impose on the informants. All informants were offered a summary of the findings after the data collection and analysis were completed.
The study did not need ethical approval according to Danish research guidelines, but followed best practices of research conduct as outlined by the Helsinki Declaration in its latest form and the Principles of Professional Responsibility by the American Anthropological Association.
Results
An overview of the characteristics of the informants is presented in Table 1. A total of nine informants were interviewed. The mean age was 54.1 years (range 38–65 years), and the proportion of women (66%) was higher. The informants’ occupational status varied from early retirement to full-time employment, and their chronic diseases ranged from common diseases, for instance type-2 diabetes (endocrine diagnosis) and chronic obstructive pulmonary disease (lung diagnosis), to rare diseases with severe influence on physical functioning, such as neurosarcoidosis (neurological diagnosis) and scleroderma (musculoskeletal diagnosis).
The complexity of living with multimorbidity
The experience of living with multimorbidity among adults in the working age was organized through three interrelated themes: 1) Impact on daily life, 2) Professional life, 3) Capacity for handling multimorbidity. Table 2 presents these themes and the related sub-themes.
Themes and related sub-themes.
Impact on daily life
The informants emphasized how several aspects of their daily life were affected by living with multiple chronic diseases. The findings related to the impact on the informants’ daily lives involve three closely related sub-themes (Table 2). For example, a physical impact of treatment or disease (e.g. side effects or symptoms) may impose additional psychological consequences (e.g. decreased self-esteem) or consequences on a person’s social life (e.g. not being able to attend social events).
Physical impact
People with multimorbidity experience various physical limitations as a consequence of their increased disease and treatment burden. Some informants emphasized the symptoms related to their chronic diseases, for example pain, fatigue and premature ageing. One informant highlighted how symptoms of chronic back pain pose restrictions on her ability to maintain a daily life: The other diseases haven’t restricted me. It’s my back pain that is my primary concern. 100%. It’s my back that gives me my limitations. I was still able to take care of my work when I broke my leg, which was a vein rupture and took a long time to heal. The vein rupture limited me so that I couldn’t practice the sport I did before, but I was still able to maintain a normal everyday life. (Female, 57 years) I know that the day after [she had injected the weekly medication], I’m not capable of doing much. But I do take my medicine, because I respect authorities, and I feel that it helps. But these are the trade-offs to me; on one hand, to feel that it’s helping me, but on the other hand, I have to live with the side effects. That’s like choosing between plague and cholera. (Female, 46 years)
Psychological impact
Informants also expressed negative psychological impacts related to living with their multimorbidity. Some informants perceived multimorbidity to be associated with premature ageing and loss of autonomy: [Mother of informant] It has taken a long time for him to overcome using a walker. He didn’t want to use it. It was just standing there for almost a year. But finally, you use it. But it is also a help. […] He has overcome using the walker; otherwise, he couldn’t go anywhere. [Informant]: ‘I couldn’t’ (Male, 38 years).
The mental adjustment of transitioning from being an active and independent individual to relying on equipment or social support was psychologically challenging. Informants expressed difficulties related to dependency as it enforced a feeling of being a burden to other people: What bothers me the most is that I don’t want to be a burden to others. I don’t want to be a hassle to anyone. No one should have to take my needs into consideration. That is hard to accept. (Male, 50 years) My daughter said it was ridiculous…Because she doesn’t have any injuries, she’s a superwoman who works 80 hours a week, and has already started working again [after giving birth]. She’s independent. She can’t quite understand that you just can’t do everything. (Female, 57 years)
Social impact
Informants highlighted difficulties of prioritizing social life vs. adhering to treatments: I get UPSET that I have to cancel the doctor, because I know it will take six months before I can get another appointment. But I also get upset if I have to cancel my trip. And the trip, it’s here and now, right? That’s just how it is. I have also experienced it the other way around, where I say: Well, I can’t go on that trip, because I have an appointment there [at the doctor]. (Female, 62 years)
The consequences of living with multimorbidity not only affected the informants themselves; it also affected their relatives and friends. The mother of an informant emphasized: It affects the whole family at many times. I’ve also had a hard time going out and having fun, because I know he’s at home, laying down (laughs sarcastically). Informant: “I told you, you shouldn’t worry about that.” […] Mother of informant: “…I come home and I’m happy and I tell him about everything I’ve experienced, and I’ve been out eating and stuff. He doesn’t experience shit, right?” (Mother of male, 38 years)
Professional life
Importance of work
In general, work life was important to many informants. Informants who were affiliated to the labour market, described how their job was very important to them, as it provided their life with meaning and structure: ‘After all, one’s work is part of one’s everyday life, to have something to get up to every day’ (Female, 57 years). In continuation, some informants stressed the social aspect of going to work, which provided them with a surplus of energy and acted as a motivation to perform daily activities.
Some informants dealt with the fact that the prospects they had for their work life were no longer realistic or achievable due to living with multiple chronic diseases. An informant had a hard time accepting that she could no longer maintain a full-time job, and she constantly tried to continue her prior work life: If I get up at night to pee, I might think “my back is fine now, you might as well work 15 minutes” (…) I did that for a period of time to see how many hours I could work…and pushed myself (…) I started to work weekends and nights (…) I blamed myself when I thought: Now you can go for a walk. Well, if you can go for a walk, then you can work too. (Female, 57 years)
Work environment
The degree of the complexity of living with multimorbidity was dependent on the flexibility and acknowledgement of the workplace. Many informants expressed that they had a positive work environment and understanding colleagues, which were important factors in regards to maintaining their health, well-being, and affiliation to the labour market. It escalates, both in terms of my ADHD and my bipolar. So, I have a hard time just sitting at work meetings and staying focused, and there are MANY meetings in the municipality. Fortunately, I have been allowed to decide what meetings I need to attend. And that’s a big help. (Female, 54 years)
Judgement from colleagues
Some informants experienced judgements from their colleagues, which were visible in various instances and had consequences on the informants’ work lives. An informant indicated that some colleagues were mistrustful and judgmental regarding her willingness to work:
‘Many colleagues don’t believe I have my diseases. I just get told: “Pull yourself together” (…)’ (Female, 59 years).
Consistently, informants emphasized how the invisible nature of chronic diseases increased the complexity of living with multimorbidity. The following quote also highlights how living with invisible chronic diseases may lead to a lack of support from colleagues:
‘They don’t see that I’m actually sick. They do not see when I start to feel pain, because I have to leave work before I am completely in pain’ (Female, 57 years).
Some informants experienced that judgements from colleagues had a direct impact on their work life. An informant recalled how he was once turned down for a work project, as he suffered from severe problems with physical functionality:
“‘I really hope that they aren’t saying: Well, he really isn’t capable of doing much, we would rather have another colleague” or “We will choose another guy for this project.”’ (Male, 50 years).
The informant was worried that colleagues perceived him as incapable of accomplishing work efficiently; and thus he pushed himself to the limits at a physically demanding job, despite contrary recommendations from his GP and family.
Capacity for handling multimorbidity
The theme ‘Capacity for handling multimorbidity’ emerged from data, as the informants articulated various degrees of competences to cope with multimorbidity in their everyday lives.
Health literacy
According to WHO, health literacy is defined as: ‘the achievement of a level of knowledge, personal skills and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions’.
45
The informants varied greatly in regards to their health literacy. The variation was often determined by the informants’ social background and level of education. Some informants were more persistent in demanding specific treatments in the healthcare system compared to other less resourceful informants. But I’m also getting to a place where I say, ‘well, I listen to my body,’ and if I feel that it [the treatment] causes some side effects that I can’t live with, then I say: ‘this is not OK for me, it’s too much, I can’t tolerate it so in that way I am not afraid to say it to the health professionals. (Female, 46 years)
Social support
The informants’ capacity of handling multimorbidity was also expressed through support from their social network, such as friends, family, colleagues, and their GP. A majority of the informants mentioned their parents and/or spouse as significant support in their daily lives; both in terms of treatment and disease management. The support was helpful in order for informants to maintain their everyday life, indicated in the following quote: I have the most amazing husband. If I ask for something, then he does it. If I’m at work, he will cook because I have to take a nap when I get home from work. It’s not even a discussion, he just does it if I ask him to. So I am very lucky […] So yes, I do get a lot of support I must say. This is not where I see problems. But it’s tough on him. I see how he feels, even though he doesn’t complain. (Female, 57 years)
A few informants highlighted positive outcomes of patient associations and meeting other patients dealing with similar types of diseases. An informant elaborated on the benefits of being a part of a patient association: No doubt about it; it has been a help. Having someone, even if it’s someone who you don’t know; they understand what you are going through. […] They have a good understanding of what it means to be invisibly sick. Mentally, you start to relax a lot more. So yes, it has been very beneficial to meet the others. (Female, 46)
Discussion
The purpose of this study was to investigate how people living with multimorbidity prioritize between social identities outside the medical encounter. So far, the vast majority of studies have tried to understand complexities of living with multimorbidity by examining the accumulation of treatment burden and disease burden.8,10,46,47 This study, too, found an increased treatment and disease burden, which underscores this as a pervasive issue among patients with multimorbidity. Further, we found that the complexity of multimorbidity is increased outside the medical encounter. Our results have shown, firstly, that people with multimorbidity experienced that the chronic diseases led to extensive physical limitations and psychological distress, which imposed challenges to maintain important aspects of their daily lives. Secondly, affiliation to work life was, too, of great importance to the informants who were still able to work full time or part-time, and they found it challenging to maintain. Lastly, we found that the impact of multimorbidity was modified by the capacity of handling multimorbidity, i.e. health literacy and/or social support.
Other studies have considered how multimorbidity challenges personal identity, in terms of disrupting daily routines and perceived roles.10,19–24 Nevertheless, people with multimorbidity strive to maintain pre-existing identities and valued social roles, e.g. ‘being a worker’, or ‘being a mum’ 19 as well as continuity of self-identity and independence. 22 Building on existing evidence about the complex experience of multimorbidity,10,19,20,24,48 SIT helps us to comprehend how the complexity of living with multimorbidity is increased by the constant conflict of prioritizing between trying to adhere to treatment and attempting to maintain identity in various social groups.
Using the SIT lens people – regardless of living with multimorbidity or not – categorize and identify themselves with various social groups (i.e. social categorization). Accordingly, the informants categorize themselves and others with work teams, families, social communities and friend groups. People adopt the identity of the group that they categorize themselves with, and membership in social groups thus provides a basis for social identities and self-concept (i.e. social identification). However, in the process of social identification, the findings suggest that living with multimorbidity compromises the informants’ abilities to maintain membership in these social groups due to physical, psychological and social impacts of living with chronic diseases. The challenges were illustrated in several situations, e.g. through increased dependency on others and equipment, lack of acknowledgement due to the invisible nature of chronic diseases, judgements from colleagues and difficulties related to completing work-related tasks. Moreover, six informants were not able to work full time (or had to retire early), and several informants could not attend social events. Thus, many social identities were affected by multimorbidity, although in this study there has been a focus on work identity. Moreover, the severity of disease and symptoms, such as pain or immobility, seemed to be crucial in relation to what extent the informants were challenged in maintaining their social identities, as some social identities were altered more than others.
In accordance with previous literature,36,37,39 we find that the informants experienced psychological distress (e.g. decreased self-esteem, lack of acknowledgement due to the invisible nature of chronic diseases, feeling like a burden to others and feelings of guilt) in cases where valued social identities were compromised in some way. In order to maintain identification with social groups, and thus psychological well-being, informants in this study repeatedly attempted to make adjustments by regulating work hours, structuring treatments and social events, ignoring symptoms at work, prioritizing social events over medical appointments or vice versa, as backed by previous literature.31,33,36 Townsend et al. (2006) found, too, that patients with multimorbidity prioritize ‘identity’ management at the expense of symptom management, and that they experience a conflict between controlling symptoms and maintaining control over social roles. In this process, we find that the informants also expressed a tendency to be involuntarily placed in out-groups, i.e. categorized as ‘abnormal’ or ‘them’, and different from the ‘normal’ or ‘us.’ 49 We see, for example, when the informants refer to themselves as ‘the one’ who cannot contribute on equal footing with colleagues, feeling judged, or are worried that they will be turned down for a work project, it demonstrates that they are no longer able to maintain their work identity, and accordingly they are placed or placing themselves in out-groups (i.e. social comparison). The exclusion by desired in-groups and the negative intergroup comparisons resulted in weakened social identities,32,36,37 e.g. constant fear of being rejected or judged. The trade-offs when prioritizing between managing chronic diseases and maintaining valued social identities, as well as the consequences that the informants experienced, demonstrate another level of the complexity of living with multimorbidity in addition to the disease and treatment burden.
Furthermore, we see that the ability to maintain social identities depends on the informants’ capacity of handling multimorbidity. High levels of health literacy, e.g. in terms of requesting coordinated treatments in the healthcare system or having a supportive spouse who takes on more household duties, was associated with sustaining certain valuable social identities, e.g. a worker identity, which is supported by previous research. 21 Thus, health literacy and social support are beneficial factors, which may reduce potential conflict associated with balancing social identities. As we found, it may be important to consider the opportunities for obtaining new social identities through patient associations, since people are more likely to receive and experience increased social support and acknowledgement from patients with similar diseases.36,50
Shippee et al. (2012) suggest a model – cumulative complexity model – that conceptualizes the complexity of living with multimorbidity. 8 The model depicts how patient complexity increases over time by workload-capacity imbalances due to accumulating burdens of treatments and illness. In continuation of the model, this study, using SIT, unfolds new insights into what increases the complexity of living with multimorbidity, emphasizing that complexity is not only created by demands from the healthcare system (i.e. patient complexity), but is to a high degree also created by demands outside the medical encounter. This study demonstrates that patients with multimorbidity attach significant value to social identities (i.e. being a worker), revealing that complexity is also increased by the social context of identity formation and in the prioritization of challenged social identities owing to multimorbidity.
The strengths of this study were its in-depth analysis of the informants’ experiences, allowing for a patient perspective on the experience of living with multimorbidity. In addition, the well-considered inclusion criteria enabled us to explore the experiences of living with multimorbidity among complex patients with higher needs of care.42,43 Our study had several limitations. The authors background and presumptions may have affected the data collection process and thereby the research findings. At the moment of data collection, CS and KR were public health students completing a final paper, and in that context the informants expressed an increased interest in helping to contribute to the field of research on multimorbidity. Yet the informants may have also perceived the authors as resourceful, healthy and highly educated individuals, which may have affected the interaction and outcome of the interviews. As an attempt to reduce any potential bias related to the interpretation of data, all authors reviewed and contributed to the coding of transcripts, which allowed for a broader understanding of the emerging themes.
The results are based on a limited number of interviews and are thus not necessarily representative or generalizable, but should be interpreted as a contribution to understanding what may form the experience of living with multimorbidity. In addition, common to other research, several eligible informants refused to participate in the interview, due to their severe disease state, lack of energy and resources. Thus, the study population may consist of a selected sample of resourceful patients compared to other patients living with multimorbidity. The cross-sectional perspective on the informants’ experiences may also be considered a limitation. Future research should consider applying a longitudinal approach, e.g. conducting follow-up interviews or using participant observation, which would provide a richer understanding of the informants’ experiences, daily lives and broader contexts.51,52
Conclusion
This study provides a patient perspective on the complexity of living with multimorbidity focusing on the impacts outside the medical encounter. The informants expressed physical, psychological and social impacts on their daily lives owing to multimorbidity, which in many cases was influenced by the level of health literacy and social support. The informants also highlighted the major effect that living with chronic disease has on the ability to maintain a normal work life, which is highlighted in this article.
Using SIT, our study illuminates that the aspiration to maintain membership within valued social groups is challenging for people living with multimorbidity because of the increased burdens of illness and treatments in their daily life. The results contribute with insights to the understanding of the complexity of living with multimorbidity from the patient perspective, focusing on how patients try to balance maintaining various social identities, while adjusting to medical appointments, treatments and other effects of living with multimorbidity. The patients are continuously confronted with demanding situations, where they are faced with dilemmas related to maintaining a coherent sense of self and a normal everyday life. The situation becomes complex, as the patients have different solutions for handling the conflict; some patients choose to prioritize symptom and treatment management, which compromises valued social identities. Other informants, on the other hand, prioritize valued social identities outside the medical encounter, which results in poorer adherence, e.g. neglecting consultations, medical advices, daily medications or treatments. Thus, this study highlights the importance of healthcare professionals recognizing the tensions and priorities that patients experience, as they try to balance multimorbidity with important aspects of their daily lives.
Supplemental material
Supplemental Material, sj-docx-1-cob-10.1177_26335565211009375 - Prioritizing social identities: Patients’ perspective on living with multimorbidity
Supplemental Material, sj-docx-1-cob-10.1177_26335565211009375 for Prioritizing social identities: Patients’ perspective on living with multimorbidity by Camilla Drivsholm Sand, Keren Rahbek, Tora G Willadsen and Alexandra R Jønsson in Journal of Comorbidity
Footnotes
Author Contribution
Camilla Drivsholm Sand and Keren Rahbek have contributed equally to this article and are first co-authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.