
Abstract
Background:
People with inflammatory rheumatological conditions (IRCs), are at increased risk of comorbidities such as cardiovascular disease, osteoporosis, anxiety and depression. The INCLUDE pilot trial evaluated a nurse-delivered review of people with IRCs which sought to identify and initiate management of comorbid conditions.
Aim:
A nested qualitative study was undertaken to examine the acceptability of the INCLUDE review.
Methods:
A qualitative interview-based design in UK primary care settings. A purposive sample of 20 patients who attended an INCLUDE review, were interviewed. Inductive thematic analysis was undertaken. Themes were agreed through multidisciplinary team discussion and mapped onto constructs of the Theoretical Framework of Acceptability (TFA).
Results:
Six themes mapped onto six of the seven TFA constructs. Patients reported the review to be effective by identifying and initiating management of previously unrecognised comorbid conditions. Some participants reported barriers to following recommendations, such as lifestyle modifications or taking more medication.
Conclusion:
A nurse-delivered review to identify comorbidities is acceptable to patients with IRCs. The TFA provided a novel analytical lens.
Keywords
Introduction
Inflammatory rheumatological conditions (IRCs) include rheumatoid arthritis (RA), psoriatic arthritis (PsA), ankylosing spondylitis (AS), polymyalgia rheumatica (PMR) and giant cell arteritis (GCA). People with IRCs are at an increased risk of comorbidities such as cardiovascular disease (CVD), osteoporosis and depression,1–6 which are key NHS priorities. 7 Despite people with IRCs being at increased risk of these morbidities they are often poorly managed, 8 leading to increased morbidity and mortality.
At present, proactive monitoring of people with IRCs is not routine, except for RA, where an annual review is a target within the Quality and Outcomes Framework (QOF). 9 The content of the review is not specified by QOF, although NICE guidance 10 advocates a ‘holistic assessment’. These reviews are often fragmented across primary and secondary care, resulting in duplication of some activities (with cost implications), for example, for CVD whilst other morbidities remain unrecognised and untreated.11,12 Review of patients with other IRCs does not routinely occur.
We undertook a pilot cluster randomised controlled trial with a qualitative process evaluation to test the feasibility and acceptability of a nurse-delivered primary care review for patients with IRCs to identify and assess, plus provide advice and signposting, for common comorbidities including anxiety and depression, and risk of cardiovascular disease and fragility fracture. Patients were provided with an individualised management plan. 13 The INCLUDE study protocol paper 13 provides details of the INCLUDE intervention.
An intervention that is not acceptable to those receiving or delivering it is not useful in clinical practice. Qualitative methods play an important role in investigating acceptability of intervention components or trial procedures. 14 However, the term ‘acceptability’ is vague, and until recently there has been little guidance on how to specify acceptability. The theoretical framework of acceptability 15 defines acceptability as ‘a multi-faceted construct that reflects the extent to which people delivering or receiving a healthcare intervention consider it to be appropriate, based on anticipated or experienced cognitive and emotional responses to the intervention’. The TFA consists of seven constructs: affective attitudes, intervention coherence, perceived effectiveness, burden, self-efficacy, opportunity-costs, and ethicality. The aim of our study was to examine the acceptability of the INCLUDE review using the TFA theory as an analytical tool for the first time in a feasibility trial.
Methods
Study setting, sampling and recruitment
The study setting was UK primary care. A sample of participants (n = 55) who attended an INCLUDE review were invited (by mail) to participate in a semi-structured interview. Participants were purposively recruited to include a range of gender, age, and IRCs (RA, PsA, AS, PMR or GCA). Attempts were made to collect data to the point where ‘new’ data did not further develop the outcome of the analysis. All interviews were undertaken by an experienced qualitative researcher (DH). Written informed consent was obtained prior to each interview. DH was not previously known to the participants as part of the INCLUDE study. NHS Research Ethics Committee approval was obtained (Ref: 17/WA/0427).
Study design
An interpretivist research paradigm underpinned this study, with the research team recognising that findings were underpinned by multiple, subjective realities, and were influenced by the interaction between participants and the researcher/s. Therefore, this research study aimed to capture these subjective experiences of the INCLUDE review through a qualitative methodology.
Semi-structured interviews were conducted with participants using a topic guide, developed by the study team and informed by a patient advisory group (PAG). This group, consisting of six patients with different IRCs, gave suggestions on re-phrasing questions to make them more accessible. The topic guide included questions that would help the team identify if there were aspects of the trial processes or intervention components that needed to be changed before proceeding with the next phase of evaluation. Questions were about experiences of inflammatory conditions, engagement with specific components of the intervention, what participants liked and did not like and why, what happened as a result of the review and if there was anything missing from the review. The guide was refined during data collection and analysis, to better capture the participants’ experiences and views of acceptability.
Face-to-face interviews took place either within the participant’s home or at their general practice. All interviews were digitally audio-recorded and transcribed verbatim by an independent transcription company. Transcriptions were checked against the audio-recording and anonymised. Interviews lasted between 30–121 minutes (average of 58 minutes).
Analysis
Analysis started as soon as the first interview was transcribed. Data were analysed using Inductive Thematic Analysis and constant comparison.16,17 Data, codes, subthemes, and themes were constantly compared with one another within and across transcripts. Codes and themes were defined by an experienced multidisciplinary team. To further understand patient acceptability, subthemes were then mapped onto the constructs of the TFA. 15
Trustworthiness
Procedures were implemented to better ensure the trustworthiness of this research. 18 For example, investigator triangulation helped to promote credibility. Codes and themes were defined by an experienced multidisciplinary team. Details of the study setting was described, and illustrative quotes used to support interpretations to better ensure transferability of the findings. To help ensure confirmability, an audit trail across data collection, analysis and the interpretation of data, was recorded.
Results
20 participants (16 females and 4 males) with a mean age of 68 years old (range 35–80 years) were interviewed, most in the 70–79 age category (n = 12). This age and gender profile is the same as that for all participants in the pilot trial. Table 1 provides participant demographic information. A broad spread of participants according to type of IRC was achieved.
Participant information.

Through the thematic analysis, six themes were developed: Expectations of the Review; Experiences of the Review; Outcomes; Burden; Wanting to Focus on their Priority; and Barriers. These six themes and their sub-themes mapped onto six of the seven TFA constructs, including affective attitudes, intervention coherence, perceived effectiveness, burden, self-efficacy, and opportunity-costs (see Online Appendix A for data mapping). It was recognised that some of the sub-themes represented more than one TFA construct; where this occurred, the data were presented under the construct which best represented that data. The results are reported under the constructs of the TFA. Illustrative data is presented to support each construct.
Affective attitudes
Affective attitudes, the participants’ feelings towards the INCLUDE review, was the most prominent construct within the data and included reasons for participating, thoughts about the different components of the review, thoughts about the outcome/s of the review, and the timing of the review.
Participants felt positive about how the review made them feel, how it was undertaken and what it contained. Several participants felt that being invited to the INCLUDE review indicated that someone cared about them and that they were being listened to: I think these things are showing that somebody cares…You’re not just a name on the list. (P14) [Case-finding questions] important to pick that up because sometimes you can talk about how the condition makes you feel…those questions kind of make you be more frank and I think probably enabled the nurse to recognise whether more support is needed or not as well. (P3) …I think it is quite important, if only from sort of the mental side of being able to discuss things…Talking about your mood and how you feel ‘cause it can have a bearing on all sorts of things, can’t it? Especially if you’re feeling down. (P20) [Mood case-finding questions] made me feel a bit anxious really ‘cause I don’t really tell people that I’m in pain. I don’t really tell people how I’m feeling. (P10) The nurse was willing to listen…they actually smiled at me; it made me feel happy and didn’t make me feel like I was being judged…their overall demeanour was really nice and warming…It just made me feel more relaxed, being able to then say what I wanted to say without being judged. (P1) …cause they were calm. You know, they were saying, ‘Well, it doesn’t matter. You know, just tell me how you feel.’…they weren’t pressurising me. They were a bit more calming influence…They didn’t get agitated with me or anything which was quite good. (P13) …we’ve looked at it a couple of times [INCLUDE summary sheet], to see, you know, on the other side it shows you different things that we’ve not heard of where you could go and look online and that…you know they’ve pinpointed us in the right direction if I need anything where I can phone and go. (P6) Essential I think [having an GP appointment made for low mood], really appropriate, it was needed, yeah, so it was the right guidance, the right advice, you know, so it was really good. (P3) I thought that was absolutely ridiculous [mild depression identified], cause I don’t, I get angry at things, but no more than anybody else does. (P16) I could have them [statins] but I’m not interested in taking anything ‘cause I think they like it around five and it was 5.3, something like that. So to me that didn’t seem enough to start taking something that I probably didn’t need really. (P17) I haven’t had symptoms for a long time, really severe symptoms for a very long time so I was a bit surprised [at being invited]…I felt a bit of a fraud because I wasn’t…as I said I had had some stiffness, which is fine. (P3)
Burden
Burden refers to ‘the perceived amount of effort that is required to participate in the intervention’.
15
Most participants did not report the review as being burdensome. However, a few participants found that the suggestions of new medications to deal with newly identified comorbidities added extra treatment burden: I don’t want to take anymore [medication]. Cause with cholesterol, is it creams and things and butter and fat…I can cut that down myself without having another tablet…The less tablets I take, the better. (P16) They asked me to see the nurse because when they took the reading, it was high. I wish [the nurse] hadn’t done that because I was already being treated for that and had been quite recently so I didn’t feel as though I needed that but you know…so I didn’t feel as though I needed that. (P11)
Intervention coherence
Intervention Coherence is the extent to which the participants understand the intervention, including the purpose of the INCLUDE review and what it entailed, and their increased risk of comorbid conditions.
Prior to attending their review, many participants were unsure of the focus of the INCLUDE review: I didn’t know what to expect…I didn’t realise they were going to talk to me about the other underlying conditions that I can have. (P10) I mean not really. They didn’t really tell me what things it could involve, the actual disease itself…(P17) …it included the whole of your wellbeing and not just your symptoms of what’s wrong. I thought it was good…Just managed to touch on everything. Cause it isn’t that long an appointment, but we seem to get quite a lot done. (P6)
Opportunity costs
Opportunity Costs are defined as ‘the extent to which benefits, profits, or values must be given up to engage in an intervention’.
15
Most patients did not need to give up ‘benefits, profits, or values’ to participate in INCLUDE. However, a small number of participants illustrated the opportunity costs of participating as they felt that the outcome from the INCLUDE review interfered with their personal priorities: I think it could be a bit complicated if you were trying to cope with you know two things…let’s get one thing sorted and then let’s start on another thing. (P15) I don’t want to think about it [comorbid conditions]…I’ve got enough with that one [partner]…it scares me a little bit, let’s put it that way. It frightens me a little bit because if he’s still alive, I won’t be able to look after him. (P19)
Perceived effectiveness
Perceived Effectiveness refers to ‘the extent to which participants perceive the intervention as achieving its purpose’.
15
Participants’ perceived the INCLUDE review to be effective as it identified their risk of comorbidities, increased knowledge of their risk of comorbidities and how this could be mitigated. Most participants reported the review to have been helpful in identifying and initiating management of previously unrecognised comorbidities: …it’s flagged a few things up with the doctors that have just let things slide, regarding me, yeah and now I’m on top of it all. (P6) The nurse said that, you know, ‘perhaps you could go to your doctors, I can’t authorise a scan for brittle bones’…(P16). The nurse identified a need for me to see the doctor, so they just said I think it would be a really good idea, why don’t you stay and see…they went straight out to see if I could see the doctor straight away so I didn’t have to do anything. (P3) it’s nice to have that reassurance that you’re doing as much for yourself as you can, you know. (P17) …it highlighted things perhaps and made it more real you know and talking about, just probably you know informing me…reminding me of the risks as well of the condition and what I can do to lower those risks as well. (P3)
Self-efficacy
Self-efficacy refers to ‘the participant’s confidence that they can perform the behaviour(s) required to participate in the intervention’.
15
As seen above participants found the review increased their understanding and awareness of comorbid conditions. Many participants were unaware of this risk until participating in the study. This awareness and understanding, whether a comorbid condition was newly identified or not, allowed patients to act indicating good self-efficacy. Although low self-efficacy was not a prominent feature of the data, there were a few examples where participants felt unable to follow through with the INCLUDE nurses’ recommendations: I do a bit – be a bit more active which sometimes, I find a bit difficult…’cause it’s painful, so I don’t walk out now like – not like I used to…in fact, I rarely go out, unless we go in the car. I mean I go and do the shopping, but I won’t walk to the shops. We’ll go in the car; that sort of stuff. (P 20)
Discussion
Summary
This qualitative study investigated acceptability of a new primary care integrated nurse-led review for patients with IRCs. We have used a novel approach by applying the TFA as an analytical lens, allowing a multidimensional and detailed investigation of acceptability. Six of the seven TFA’s constructs were identified within the data (affective attitudes, intervention coherence, perceived effectiveness, burden, self-efficacy and opportunity-costs). The findings illuminate the acceptability of an integrated primary care nurse-led review from the patient’s perspective, and have illustrated areas of further development, including enhancing INCLUDE nurse training. This study contributes to the rapidly growing literature around TFA and has implications for the presentation of the TFA findings, including presenting it in a more dynamic model to illustrate interconnectedness and significance of constructs for the proposed intervention. The implications and recommendations are discussed in more detail under the implications section.
Strengths and limitations
A key strength of this research study was the method of analysis and procedures used to better ensure trustworthiness of data. 18 For example, inductive thematic analysis helped to maintain the participants’ voices and grounded the findings in the participant data. Subsequent deductive mapping of themes and subthemes to the TFA further interrogated the data and provided deeper insight into acceptability through its multiple constructs.
We interviewed a sample of participants from the INCLUDE trial. However, those who did not find the review acceptable may not have agreed to participate in interviews. However, overall in the pilot INCLUDE trial, there was good uptake of the INCLUDE intervention as 76% of those invited came to a review.
We only report on the perspectives of patients, and these need to be considered alongside perspectives of the nurses delivering the intervention. Analysis of interviews with nurses and general practitioners is ongoing and will be reported separately.
Comparison with existing literature
The TFA is fast gaining recognition in health research and has been used throughout studies in different ways, including: to highlight how their findings were in line with TFA constructs19–25; in aspects of study design or analysis26–30; and in protocol papers outlining how they will use the TFA in future.31–34 Unlike this study, Nadarzynski et al. 27 used the TFA to inform questions on a topic guide about acceptability of artificial intelligence led chatbox services; however, they did not analyse the data using the TFA.
Like our study, other studies have used the TFA to analyse their data. For example, Jan-Kuriawati et al. 28 used TFA constructs to guide thematic analysis of data in a qualitative study of private practitioner’s views of mandatory tuberculosis notification in Indonesia and report 4 TFA constructs in their data. Murphy et al. 29 also applied the TFA as a coding scheme to analyse data from interviews with Community Pharmacists on acceptability of a men’s mental health promotion programme, and report effectiveness of the intervention, burden, and self-efficacy as the most commonly occurring constructs.
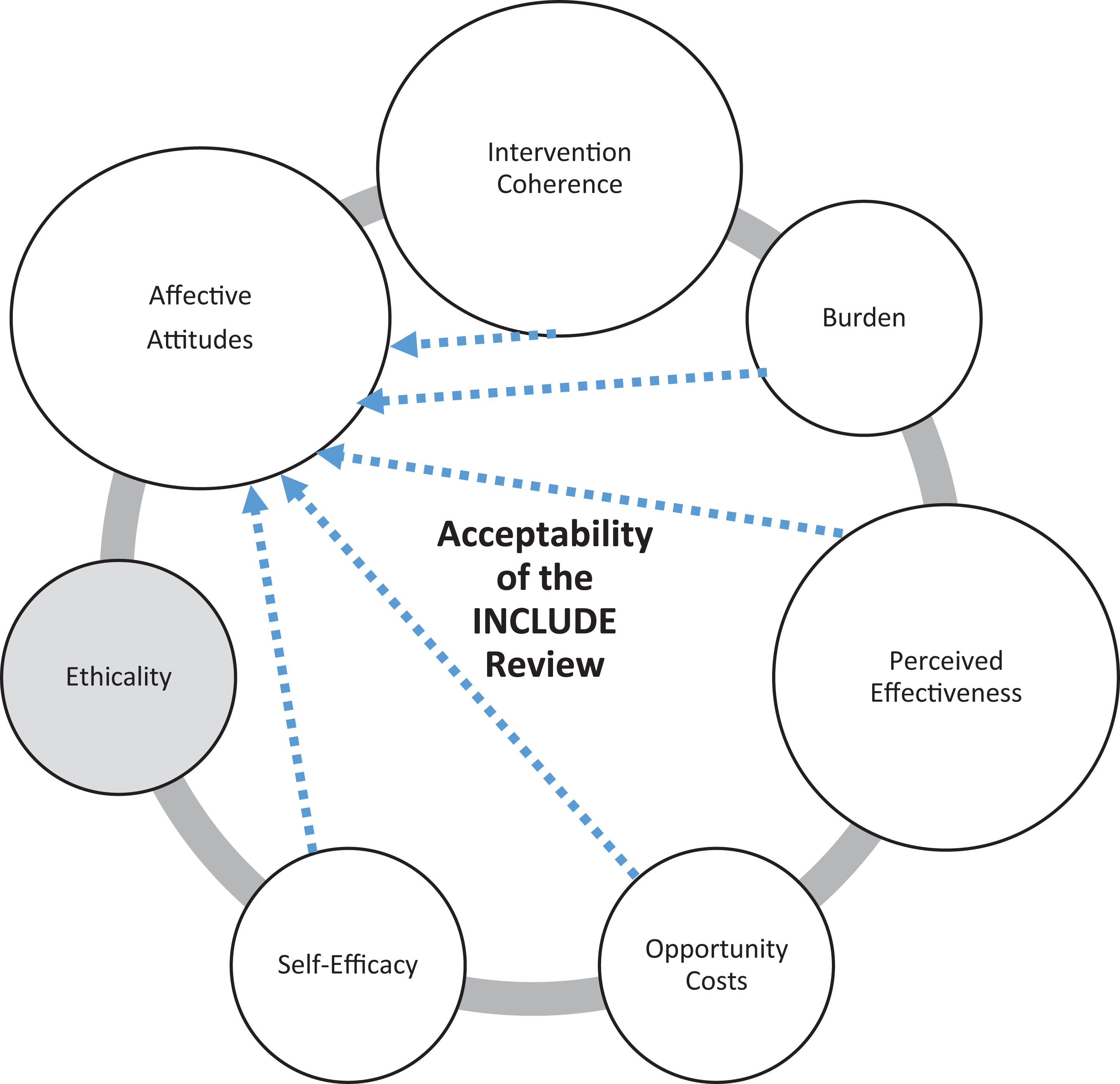
Some studies have proposed new acceptability domains. Jan-Kuriawati et al. identified external and environmental factors of acceptability. 28 Mukunya et al. suggested that social and cultural dimensions of acceptability are undervalued currently in the TFA. 30 Our study has also contributed to the development of the TFA, recommending the TFA findings be presented in a more dynamic model to illustrate interconnectedness and significance of constructs for the proposed intervention (see Figure 1). As only two of the original 43 reviews used to develop the TFA were qualitative reviews, 15 future qualitative studies will have an important role in providing and then assessing new insights on acceptability domains and adding to the model as it is used in wider contexts and settings.
Acceptability of the INCLUDE review using the Theoretical Framework of Acceptability.
Implications
Optimising acceptability of the include review
This work identified a few areas for optimisation of the INCLUDE review ahead of a larger evaluation. These can mostly be addressed through enhancing the nurse training programme as follows: Recognition that patients may feel concerned discussing the depression and anxiety case-finding questions (Affective Attitudes) Clarification that risk of comorbidities is not necessarily related to current inflammatory activity of the IRC (Coherence) Discussion of the potential impact of increased medication required for newly identified conditions or risks (Burden) and how patient’s existing priorities may be impacted by the review (Opportunity Cost) Reinforcement of strategies to check how the patient feels about following recommendations made in the review and to determine their confidence in attempting lifestyle changes (Self-efficacy)
Reflections on the use of the Theoretical Framework of Acceptability (TFA)
The TFA theory provided a useful analytical framework by allowing a more in-depth and multi-dimensional, theoretically informed analysis of acceptability. Sekhon et al. present the constructs of the TFA in alphabetical order in a linear model and outline the extent to which they may cluster or influence each of the temporal assessments of acceptability is an empirical question. 15 Our study has illustrated that the constructs are interconnected, not isolated and constructs exerted influence over one another. For example, patients’ perceptions that recommendations from the nurse added extra burden (Burden), influenced how they felt towards the review (Affective Attitudes).
Though the TFA’s constructs represented in these findings were important for assessing acceptability of the INCLUDE study, some were more populated than others. No data were mapped to the TFA construct of ethicality; though the lack of findings linked to ethical issues may be explained by the topic guide not being generated using TFA constructs.
We recommend presenting TFA findings in a more dynamic model to illustrate interconnectedness and significance of constructs for the proposed intervention as illustrated in Figure 1. Instead of a linear representation of the constructs we have used a ring. Larger circles represent constructs that were well presented in the dataset, smaller circles had less data, and those greyed out had no data. Arrows show the direction of influence between constructs. The approach is applicable to all studies using the TFA. In the INCLUDE study all constructs identified in the data exerted influence on affective attitudes. In a study of prospective acceptability of giving smoking cessation advice at the point of cervical screening, Mansour et al. 19 found that expected interaction (quality of communication) between the person delivering and the person receiving the intervention would influence affective attitude. Our study supports links with all TFA constructs and affective attitude in a retrospective analysis (after the intervention has been experienced). Other studies may find different links.
Conclusions
The nurse-led review, aimed at identifying previously hidden comorbidities, was acceptable to patients with IRCs, participating in a pilot trial. Patients reported feeling cared for, and valued the components of the review, including the opportunity to discuss their health more broadly. There were few examples of reported burden, opportunity costs, and low self-efficacy. The theoretical framework of acceptability was useful in providing an in-depth and multi-dimensional analysis. Whilst this analysis is vital preparation for a fully-powered randomised controlled trial, there are also implications for clinical practice. Identifying and managing people with multimorbidity is an increasing challenge for primary care and recognising additional comorbidities in people with LTCs is key to improving patient outcomes. We have demonstrated that case-finding for additional morbidities is acceptable to patients, who are then willing to take on further work 35 in self-managing identified conditions.
Supplemental material
Supplemental Material, sj-doc-1-cob-10.1177_26335565211002402 - Acceptability of nurse-led reviews for inflammatory rheumatological conditions: A qualitative study
Supplemental Material, sj-doc-1-cob-10.1177_26335565211002402 for Acceptability of nurse-led reviews for inflammatory rheumatological conditions: A qualitative study by Daniel Herron, Carolyn A Chew-Graham, Samantha Hider, Annabelle Machin, Zoe Paskins, Kendra Cooke, Erandie Ediriweera Desilva and Clare Jinks in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-doc-2-cob-10.1177_26335565211002402 - Acceptability of nurse-led reviews for inflammatory rheumatological conditions: A qualitative study
Supplemental Material, sj-doc-2-cob-10.1177_26335565211002402 for Acceptability of nurse-led reviews for inflammatory rheumatological conditions: A qualitative study by Daniel Herron, Carolyn A Chew-Graham, Samantha Hider, Annabelle Machin, Zoe Paskins, Kendra Cooke, Erandie Ediriweera Desilva and Clare Jinks in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-docx-1-cob-10.1177_26335565211002402 - Acceptability of nurse-led reviews for inflammatory rheumatological conditions: A qualitative study
Supplemental Material, sj-docx-1-cob-10.1177_26335565211002402 for Acceptability of nurse-led reviews for inflammatory rheumatological conditions: A qualitative study by Daniel Herron, Carolyn A Chew-Graham, Samantha Hider, Annabelle Machin, Zoe Paskins, Kendra Cooke, Erandie Ediriweera Desilva and Clare Jinks in Journal of Comorbidity
Footnotes
Acknowledgements
We thank the General Practices who agreed to take part in the INCLUDE study and participants who were interviewed. We also thank the Research User Group at the School of Medicine at Keele University and the PPIE team who helped to co-ordinate the patient advisory group. This study was supported by Keele Clinical Trials Unit.
Author contributions
CJ, SH, CCG conceived of the study idea. CJ, SH, CCG, AM, DH, KC, EH all contributed to research design and protocol writing. DH undertook all data collection and led the analysis. All authors (CJ, SH, CCG, AM, ZP, DH, KC, EED) contributed to analysis and data interpretation. AM and DH lead the PPIE work. CJ and DH led the writing and all authors (CJ, SH, CCG, AM, ZP, DH, KC, EED) contributed to article writing. All authors read and approved the final manuscript.
Data availability statement
Data is available in Online Appendix A. The datasets used and/or analysed during the current study are available from Clare Jinks on reasonable request and in line with standard operating procedures on data sharing at Keele University. The INCLUDE Summary sheet is provided in Online Appendix B.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
NHS Research Ethics Committee approval was obtained (Ref: 17/WA/0427).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research jointly supported by the Haywood Rheumatology Research and Development Foundation and the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care West Midlands (NIHR CLAHRC WM), now recommissioned as NIHR Applied Research Collaboration West Midlands (WM ARC). ZP is funded by the NIHR Clinician Scientist Award (CS-2018-18-ST2-010). The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. CJ and CC-G are part funded by WM ARC.
Informed consent to participate
All participants provided written informed consent to participant in the INCLUDE trial. In addition, written informed consent was obtained prior to each interview.
Informed consent to publish
Prior to giving consent to participate in an interview patients received a Patient Information Leaflet that included the following statement ‘Quotations from the discussion may be used in reports of this study. Your identity (name, address and any personal information) will not be revealed in any such report, so that your personal details will not be shown’.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.