
Abstract
Objectives
To categorize and examine the effectiveness regarding health-related quality of life (HRQoL), mental health, and mortality of care models for persons with multimorbidity in primary care, community care, and hospitals through a systematic review.
Methods
We searched PubMed, Embase, and Cochrane Central Register of Controlled Trials up to May 2020. One author screened titles and abstracts, and to validate, a second author screened 5% of the studies. Two authors independently extracted data and assessed risk of bias using the tool by the Cochrane Effective Practice and Organisation of Care group. Study inclusion criteria were (1) participants aged ≥ 18 years with multimorbidity; (2) referred to multimorbidity or two or more specific chronic conditions in the title or abstract; (3) randomized controlled design; and (4) HRQoL, mental health, or mortality as primary outcome measures. We used the Foundation Framework to categorize the models and the PRISMA-guideline for reporting.
Results
In this study, the first to report effectiveness of care models in patients with multimorbidity in hospital settings, we included 30 studies and 9,777 participants with multimorbidity. 12 studies were located in primary care, 9 in community care, and 9 in hospitals. HRQoL was reported as the primary outcome in 12 studies, mental health in 17 studies, and mortality in three studies—with significant improvements in 5, 14, and 2, respectively. The studies are presented according to settings.
Conclusions
Although 20 of the care models reported positive effects, the variations in populations, settings, model elements, and outcome measures made it difficult to conclude on which models and model elements were effective.
Keywords
Strengths and limitations of this study
• A major strength is the systematic approach to identify and include the randomized controlled trials. • The use of the Foundation Framework secured detailed descriptions of the care models. • It is a strength that the review includes all three settings: primary care, community care, and hospitals.
Introduction
Multimorbidity is often defined as the coexistence of two or more chronic conditions in the same individual1,2; however, the definition varies throughout the literature.3–5 Multimorbidity is associated with decreased physical functioning, decreased health-related quality of life (HRQoL), increased use of health services, and higher mortality. 6 The prevalence of multimorbidity is rising globally,7–9 resulting in burdens for individuals and healthcare systems. 10 Social disparities are linked to the prevalence of multimorbidity, 11 and a socioeconomic gradient has been observed in healthcare utilization, with more hospitalizations and bed days among persons with shorter education compared to those with longer education. 12 Furthermore, the lack of integrated care is a common experience among patients with multimorbidity. 13
Care models, as we defined as a number of model elements aiming to improve the quality of delivered healthcare services, have been developed for providing integrated, patient-centered care for single chronic conditions and multimorbidity. The most notable frameworks for care models are the Chronic Care Model,14,15 the SELFIE model (Sustainable intEgrated care modeLs for multi-morbidity: delivery, FInancing and performancE), 16 and the World Health Organization (WHO) model of integrated, people-centered care, 17 and more recently, the Multimorbidity Care Model from the European Projects CHRODIS and CHRODIS Plus. 18 These frameworks provide approaches to improve integration of care and increase patient-centeredness, but few have been adequately evaluated for effectiveness among populations with multimorbidity. Consequently, healthcare professionals and decision-makers are left with few options to provide evidence-based care for persons with multimorbidity. At the same time, there is a lack of consensus in describing models of care for multimorbidity as well as the most suitable outcome measures, which complicates concluding on the effectiveness of models of care for patients with multimorbidity. 19 In 2017, the Foundation Framework—a framework for developing and reporting models of care for multimorbidity—was published, offering an approach to categorizing models of care for multimorbidity. 19 The Foundation Framework is a powerful approach to undertake detailed comparisons of models of care and bring together the heterogeneous field of models targeting multimorbidity through shared descriptions.
To our knowledge, two former reviews have been conducted to test the effectiveness of models of care for multimorbidity. This is a Cochrane review of interventions for improving outcomes in patients with multimorbidity in primary care and community settings. 20 The review was updated in 2016, searched the scientific literature up to 2015, and included 18 randomized controlled trials (RCT). 21 The review was further corrected in 2021 removing one of the studies from the 2016 version. 22 Additionally, a systematic review updated and narrowed the focus of the Cochrane review by excluding comorbidity studies—taken the consequence of the growing discussing toward a distinction between the concept of multimorbidity and comorbidity. 23 The conclusions in the reviews were rather similar, both highlighting that the effectiveness of interventions for people with multimorbidity remained uncertain, with mixed findings overall and a need for further studies on the topic.21,23 The reviews did, however, only include studies conducted in primary care and community settings and did not include models of care taking place in a hospital setting.
This study aimed to categorize and examine the effectiveness of models of care designed to improve health-related quality of life (HRQoL), mental health, or mortality for persons with multimorbidity in primary care, community-based care settings, or hospitals through a systematic review of RCT studies.
Methods
We applied the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting and reporting the study. 24 The review protocol was registered with PROSPERO (Ref no: CRD42019119490).
Search strategy
Our search strategy built upon previous work21,25 and was modified in collaboration with a research librarian. We searched PubMed, Embase, and the Cochrane Controlled Register of Trials (CENTRAL) databases. Our searches for models of care in primary care and community-based care settings included the time period from August 2017 through May 2020. For models of care in hospital settings, we searched from January 2013 through May 2020. The time limit of 2013 onwards for hospital settings was applied after observing a spike in publications on the topic of multimorbidity in 2013 26 and deemed a meaningful way to limit the search to recent studies. All search strategies are presented in Supplemental file 1.
Inclusion criteria for considering studies for this review
We considered studies with RCT design in which outcome measures were evaluated for models of care. We included studies of participants aged ≥ 18 years with multimorbidity. We defined multimorbidity, in line with the widely used definition as “two or more chronic conditions in the same individual”. 2 Studies had to refer to multimorbidity or two or more specific chronic conditions in the title or abstract to be considered for inclusion. Studies had to report the effectiveness of one of the primary outcome measures: HRQoL, mental health, or mortality. This was based on the core outcome set for multimorbidity research developed using the Delphi method and in which these three outcomes were ranked highest and deemed the most relevant when evaluating models targeting multimorbidity. 27 We included studies taking place in primary care, community-based care settings, and hospitals. Primary care was defined according to the MeSH term as “care which provides integrated, accessible healthcare services by clinicians who are accountable for addressing a large majority of personal healthcare needs, developing a sustained partnership with patients, and practicing in the context of family and community.” 28 In the search, we included terms as general practice, general practitioners, family physicians, and primary health care. Community-based care was defined as “diagnostic, therapeutic and preventive health services provided for individuals in the community” 29 —and we included terms as community, community health nursing, and homecare services in the search. Hospital was defined as “institutions with an organized medical staff which provide medical care to patients. The branch of medicine concerned with the delivery of comprehensive medical care to hospitalized patients” 30 —and we included terms as hospitals, secondary care, and ambulatory in the search.
We excluded study protocols, pilot studies, and studies published in other languages than English, Danish, Swedish, or Norwegian. We excluded studies of populations with the combination of mental illness and substance use disorder, as the social and medical complexity arising from these combinations were deemed too different from the remaining populations.
Review process
After retrieving identified citations from the three databases, one author screened titles and abstracts for inclusion. To validate the title and abstract screening, a second author rescreened a randomly selected 5% sample of citations; the value of Cohen’s Kappa was 0.66 indicating substantial inter-rater agreement. Two authors independently read the full text of all included citations and reached a consensus about studies to include in the review. Reference lists of included articles were hand-searched to identify additional relevant studies, and all articles included in the previous reviews21,23 were assessed for eligibility. Two authors independently applied the risk of bias criteria established by the Cochrane Effective Practice and Organisation of Care (EPOC) group to each study. 31 We assessed the risk of selective reporting for each article by comparing the primary and secondary outcomes listed in the methods section with primary and secondary outcomes reported in the results section. For each study, a low, unclear, or high risk was assigned for each criterion. Disagreements were resolved by consensus.
Analysis
Data extraction
Study characteristics.


Categorization of models of care—using the Foundation Framework
To gain a detailed and systematic view of the included care models we used the Foundation Framework for Development and Reporting New Models of Care for Multimorbidity to categorize the care models.
19
The framework is developed for models of care in primary care, and according to the framework, the Theoretical Basis, that is the underlying assumptions of how a given model may work, and a defined Target Population are the foundations of the care models. The implemented changes are labeled Model Elements and in total the framework lists and describes 28 specific model elements. These model elements are categorized into three groups: Clinical Focus of Care, Organization of Care Delivery, and Support for Model Delivery. Figure 1 illustrates the model terminology and how a model of care consists of different model elements. Supplemental file 2 provides a list of the 28 specific model elements used in the framework, their definitions, and our considerations, adaptions, and interpretations for applying the framework to community-based care and hospital settings—and not only primary care as the framework originally was intended for. One example for adaption was regarding the model element “Integration with secondary care”—here the original definition was “Primary care working more closely with secondary care”. For care models in community-based care settings and hospital settings this element was changed to “community-based care working more closely with secondary care” and “hospital-based care working more closely with primary care,” respectively. Two authors independently categorized the included care models according to the framework, and disagreements were resolved by consensus. This was done for each of the three settings, separately. Model terminology, inspired by the Foundations Framework (Stokes et al. 2017).
Effectiveness of the models of care
We based our effectiveness assessment on the core outcome set for multimorbidity. 27 We therefore only included studies reporting one of the three primary outcome measures: HRQoL, mental health, or mortality. Next, for each setting, we combined the insight from the data extraction, the categorization of the models, and the results of the outcome measures. Due to the heterogeneity of the included studies according to variation of the study populations, care models, and specific model elements, the synthesis of the results is narrative.
Results
The search strategy yielded 10,808 citations. After removing duplicates and applying language and time restrictions, 7,021 citations remained for the title and abstract screening. Of these, 169 were included in the full-text screening. The full text of an additional 18 articles included in the previous systematic review
22
was also screened. A total of 30 studies were included in the synthesis.25,32–60 Figure 2 depicts the selection process. PRISMA flow diagram.
Study characteristics
Data extraction from studies in primary care settings.

Data extraction from studies in community-based care settings.

Data extraction from studies in hospital settings.

Categorization of models included in the review—using the Foundation Framework
Categorization of models of care located in primary care—using the model elements defined in the Foundation Framework.


Categorization of models of care located in community-based care settings—using the model elements defined in the Foundation Framework.


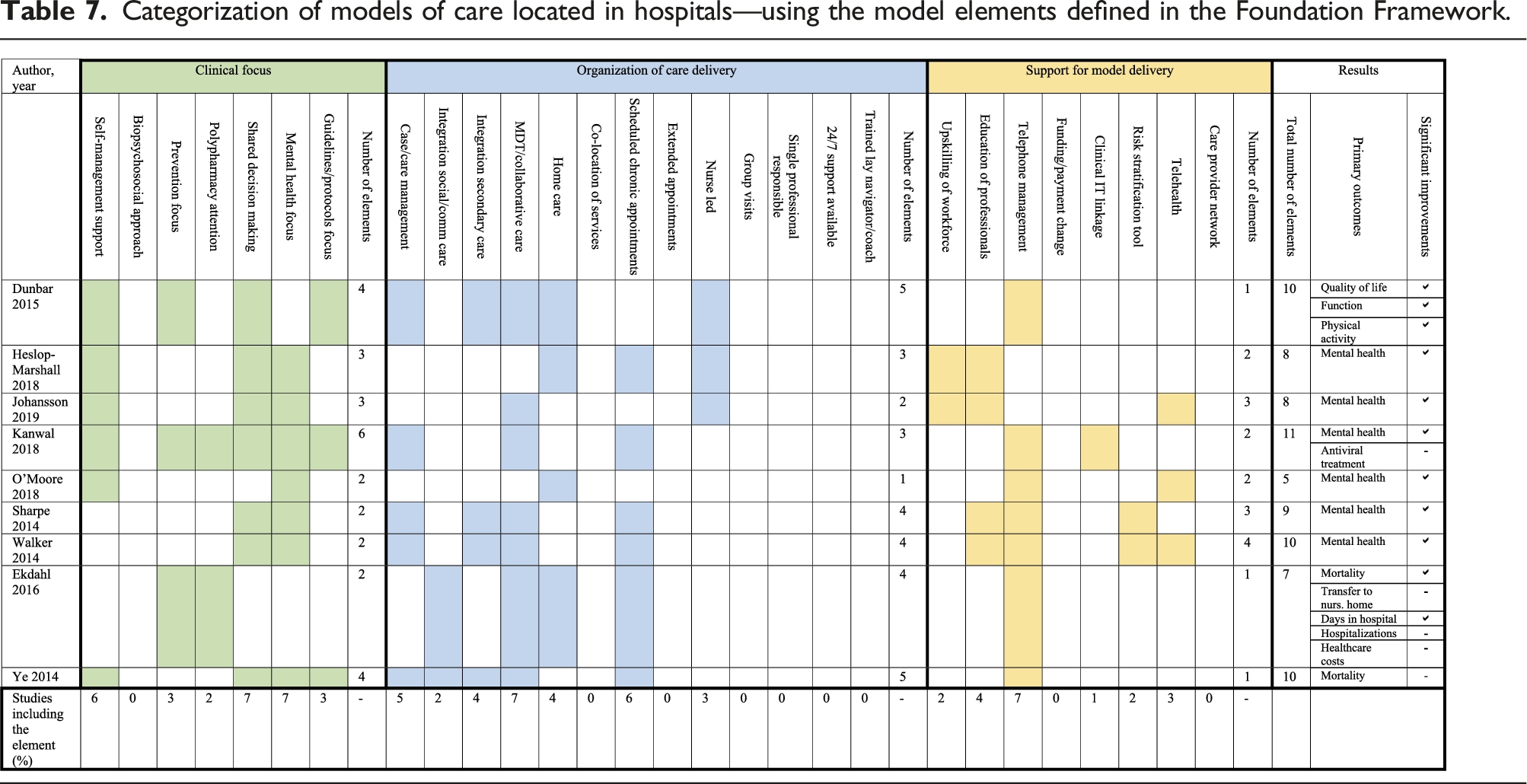
Categorization of models of care located in hospitals—using the model elements defined in the Foundation Framework.

Risk of bias
Based on the EPOC criteria,
31
we judged the overall risk of bias in the included studies as low (Figure 3). Studies in primary care were primarily cluster-randomized, with the unit of randomization being the practice; thus, there is an overall low risk of the control group being contaminated in those studies. However, the category “incomplete outcome data” were a risk of bias in some of the studies in primary care. Studies in community-based care settings had a high risk of bias for more criteria than studies in other settings because many did not have similar baseline characteristics and had incomplete outcome data or a high risk of control group contamination. We judged the risk of selective reporting to be low; all but three studies reported all results for primary and secondary outcomes described in the methods sections. We also judged studies in hospitals as generally having a low risk of bias except for control group contamination, as most models took place in single hospital departments. Figure 3 provides detailed results of the risk of bias assessment. Risk of bias.
Outcome measures and effectiveness
HRQoL was reported in 10 studies as the primary outcome measure, mental health in 15 studies, and mortality in three studies—two studies reported both HRQoL and mental health as the primary outcomes. HRQoL included specific outcomes such as disease-specific quality of life, health and functional status, physical functioning, and self-rated health. For mental health, specific outcomes included self-reported depression severity, depression and anxiety scores, a composite measure of pain, anxiety, and depression, psychiatric symptom severity, depression improvement (including depression-free days, remission, and treatment response), and psychological distress. Mortality outcomes included standard outcomes for mortality such as survival time. Overall, 20 of the studies showed significant improvement in the primary outcome of interest—seven in primary care, five in communities, and eight in hospitals. Figure 4 shows the effectiveness of the care models for each of the three primary outcome measures HRQoL, mental health, and mortality—and divided for each of the settings primary care, community, and hospital. Effectiveness of the care models for each of the three primary outcome measures health-related quality of life (HRQoL), mental health, and mortality (x-axis)—and divided for each of the settings primary care, community, and hospital. The y-axis indicates numbers of care models. The blue color indicates positive improvements and the gray color indicates no improvements.
In the following sections, the results from the 30 studies are reported separately for primary care, community-based care, and hospital settings (Tables 5–7).
Primary care settings
Overall, seven of the 12 studies taking place in primary care reported significant improvement in the primary outcome. Six studies reported outcomes for HRQoL,25,44–47,60 and significant improvements were reported in only one of these studies. 44 The study, which found significant improvements in HRQoL, included three model elements categorized as Clinical Focuses, six model elements characterized as Organization of Care Delivery, and three model elements characterized as Support for Delivery. Outcomes for mental health were reported in six studies,48–52,60 of which five reported significant improvements.48–51,60 These five studies had between three and six Clinical Focuses and between two and five model elements characterized as Organization of Care Delivery. One of the models included four model elements characterized as Support for Model Delivery, 49 while the four remaining models included two model elements characterized as Support for Model Delivery. The one study reporting mortality found a significant reduction in mortality and had two model elements in Clinical Focus, one model element characterized as Organization of Care Delivery, and two model elements characterized as Support for Model Delivery. 53
Community-based care settings
Overall, five of the nine studies taking place in community-based settings reported significant improvement in the primary outcome. HRQoL measures were reported in five studies32,43,54–56 and the outcome measures improved significantly in three of the studies.32,43,56 The studies that reported significant improvements had between three and five model elements with a Clinical Focus, two or three model elements were characterized as Organization of Care Delivery, and between zero and three model elements were characterized as Support for Model Delivery. However, for two of these studies, improvements were only observed for the mental health aspect of HRQoL.43,56 Mental health was reported in five studies,33,56–59 and in three studies, significant improvements were observed.33,56,58 These care models included between two and four different model elements with a Clinical Focus, between one and three model elements characterized as Organization of Care Delivery, and between one and three model elements characterized as Support for Model Delivery.
Hospital settings
Overall, eight of the nine studies taking place in hospital settings reported significant improvement in the primary outcome. HRQoL was reported in one study and a significant improvement was found. 34 In this study, the care model included four Clinical Focus model elements, five model elements were characterized as Organization of Care Delivery, and one model element as Support for Model Delivery. Six studies reported results for mental health outcomes,35–40 with significant improvements observed for all studies. These care models mostly included two or three Clinical Focus model elements, and one model included six Clinical Focus model elements, between one and four model elements characterized as Organization of Care Delivery, and between two and four model elements characterized as Support for Model Delivery. Two studies reported mortality,41,42 and one of the studies found significant improvements. 41 The study reporting significant improvement in mortality included two model elements with Clinical Focus, four model elements characterized as Organization of Care Delivery, and one model element characterized as Support for Model Delivery.
Across the three settings, no given number or combination of model elements was linked to improvements in the three outcomes.
Discussion
In this review, we included 30 studies assessing the effectiveness of care models for persons with multimorbidity; 12 studies took place in primary care, nine in community settings, and nine in hospitals. Totally, 9,777 participants with multimorbidity were included in the studies. The studies included between five and 14 different model elements—with self-management support, mental health focus, case management, scheduled chronic appointments, and telephone management being the most frequent. The content of the care models showed a very high heterogeneity according to the defined multimorbidity populations and to the complexity of the care models. Twenty of the studies showed significant improvement in the primary outcome of interest; these were fairly evenly distributed across settings. However, the variations in target populations regarding type of conditions, number of conditions, the model elements, settings, and outcome measures are some of the topics that complicate drawing conclusions of the effectiveness of the care models for people with multimorbidity.
This is the first study to report effectiveness of care models in patients with multimorbidity in hospital settings—and the results indicate a strong tendency for studies taking place in hospital settings to show positive results. As previous reviews21,23 only included studies performed in primary care and community settings, the studies from the hospital settings add important evidence to the field regarding effectiveness of care models in hospital settings. Further, there was a tendency for studies with mental health as the primary outcome to show positive results. This was in contrast to the previous review by Smith and colleges in which they found “little or no difference to the main outcomes of mental health.” 23 However, most of included hospital setting studies in this review were not included in the Smith review because they were characterized as comorbidity studies—with patients having an index disease and any additional disease. 61 As all the included studies from the hospital setting reported positive improvements, the dissimilar results regarding mental health might be explained by reporting results from these studies, which are not included in previous reviews. Our findings concerning the outcome measure HRQoL were mixed, although we found a potential beneficial effect on HRQoL for some community-based care models. Overall, our results indicate that in many cases, the health outcomes, HRQoL, mental health, or mortality, among people with multimorbidity can be improved if something beyond the usual care is provided. Despite the fact that 20 of the 30 studies reported improvement in the primary outcome, there is still no clear evidence to guide healthcare professionals in which care models or model elements to implement to improve effectiveness of care. The mixed results are in line with the results from the previous reviews of Smith et al., in which it was concluded that the effectiveness of models of care for multimorbidity is uncertain.21,23 Only, three of the 30 included studies reported on mortality as primary outcome measure. This is not that surprising since it is challenging to improve mortality rates and often it requires a longer follow-up time for assessment.
The use of the Foundation Framework clarified the variety of the included model elements—regarding types, number, and combinations—which complicated conclusions regarding which elements were effective. We found that self-management support was the model element (Clinical Focus) most used in the care models—included in 25 of the 30 studies in this review. This agrees well with the fact that self-management has been assessed as one of the most effective elements in models of chronic care. 62 Further, case management and scheduled chronic appointments were most often used in the category Organization of Care Delivery. It is well-documented that patients with multimorbidity often describe care as fragmented, meeting many health professionals in different organizations, and challenges with information transfer between organizations.13,63,64 Case management is expected to improve integrated care and supposedly, the patients’ perception of the care as more integrated, with one healthcare profession having the overall responsibility for the care plan, which might be the reason why case management is so often included in the care models. Interestingly, the newest review highlighted that self-management support and care coordination interventions may improve patients’ experience of care. 23 We found no obvious association between the number and types of model elements used in the models of care and the results of the outcome measures. None of the studies reported the implementation level of the model elements, which also complicates comparison of the model elements and their effectiveness. Process evaluation could be a valuable method to improve the understanding of which model elements are effective for whom under which circumstances. 65 Some studies mentioned parallel qualitative process assessment but also included key care processes as secondary outcomes, to open the “black box”. 25 This is, however, beyond the scope of this review but could be relevant to review in future work.
Even though the Foundation Framework originally was developed to characterize care models in primary care settings, 19 we applied the framework for care models implemented in community and hospital settings. We adapted few of the model elements in the framework, before using them for the community-care and hospital settings. We found it reasonable to use the model elements defined in the framework for studies taking place in all three settings. The framework is based on the best available evidence, and it provides specific definitions of model elements constituting the care models. Using the framework ensured a systematic description of the care models and a nuanced categorization of the models based on their model elements.
Less than half of the included studies reported a theoretical basic of the care models of which Collaborative Care and the Chronic Care Model were the two most frequently used theoretical models.14,15 None of the studies applied care models developed for multimorbidity, such as the WHO model, the SELFIE model, or the Multimorbidity Care Model.16–18 This is problematic, as these frameworks for care models are developed to support the complex care provision needed in patient populations with multimorbidity. The models are expected to support integrated patient-centered care and so provide higher quality of care. The reason for not using the WHO, the SELFIE model, or the Multimorbidity Care Model can supposedly be explained by the fact that these models did not exist when many of he included studies were designed. Future research should benefit from these models when designing new studies to improve outcomes in patients with multimorbidity.
In the current review, we used the widely used definition of multimorbidity, namely, the coexistence of two or more chronic conditions in the same individual.1,2 Despite all included studies met the inclusion criteria about referring to multimorbidity or two or more specific chronic conditions in the title or abstract, the included multimorbidity populations were very heterogeneous across the studies. Some of the studies in the present review included populations with specific chronic conditions; other studies had no condition-specific inclusion criteria and others again included populations with both somatic and psychiatric conditions. This variety in the definition of multimorbidity is a well-known problem in the research area of multimorbidity3–5 and is a general challenge when comparing outcomes from studies in multimorbidity populations. 4 Furthermore, an ongoing discussion about a necessary distinction between the two closely related concepts multimorbidity and comorbidity is evolving. 61 In this distinction, comorbidity is seen as the co-occurrence of any additional disease entity in a patient who has the index disease, and multimorbidity is seen as the coexistence of two or more chronic conditions, where one is not necessarily more central than the others. 61 Multimorbidity is the more general term and individuals with comorbidity also have multimorbidity, but the reverse does not necessarily apply. Therefore, we choose not to consider comorbidity separately in our study. However, the varying definitions—and the distinction between the two concepts—make the overall evaluation of outcomes of models of care for multimorbidity difficult because observed effects are likely specific to the conditions and the combinations of conditions being studied. Moving forward, there is a need to establish consensus about clinically meaningful definitions of multimorbidity—both for consensus in the research area and for the daily clinical work with patients. 4 We found that patients with depression in combination with other conditions were the most used targeted population in the included studies. This is not that surprising since this population includes patients known to have poor health—among other aspects, reflected in the significantly poorer HRQoL and higher mortality compared to the general population.66,67 However, it is a difficult population to target because people with mental illness often have difficulties in receiving somatic care as needed for several reasons—and integrated care will be even more important for this patient group. Furthermore, for most included studies, particularly those in primary care and hospitals, participants were over the age of 50 years. The prevalence of multimorbidity is also high among younger individuals, 68 and the feasibility and effectiveness of models of care among younger populations merit investigation.
The difficulty of drawing conclusions on the effectiveness of complexity that characterize the care models of this study is a well-known problem. 65 Understanding the effect of models of care in patients with multimorbidity is, however, further complicated due to the different combinations of conditions with varying duration, levels of severity, and activity of the conditions, and with varying impact on patients’ perception of their health status. In addition, it is becoming increasingly acknowledged that the single-disease approaches to measuring the quality of care for patients with multimorbidity do not capture the complexity of the processes involved in meeting the more multifaceted needs for this population. 64 The study from Smith et al. 27 is one of the first attempts to characterize a core outcome set for multimorbidity research and HRQoL, mental health, and mortality were the highest-ranked outcomes between 17 outcome measures; wherefore we focused on those three outcomes in this review.
Strengths and limitations
A major strength of the current review is the systematic approach to identifying and including studies. Furthermore, the selection process is in accordance with PRISMA-guidelines and the use of the Foundation Framework secured detailed descriptions and comparisons of the models of care. Additionally, it is a strength that the review includes studies conducted in primary care, community care, and hospital—and not, as previous reviews, only primary care and community care. However, some limitations deserve attention as well. By using the three highest-ranked outcomes from the core outcome set for multimorbidity, we excluded 11 studies (Figure 2). We are aware of the importance of this selection and for such, we could have included other outcomes and showed other results. However, we chose these three outcomes because it was the highest-ranked outcomes in the Delphi panel study by Smith et al. In the assessment of bias, we used the risk of bias criteria established by the Cochrane Effective Practice and Organisation of Care (EPOC) group, which is a recognized tool for assessment of bias. Assessment of Certainty through a specific GRADE assessment could have been considered. Due to the heterogeneity of the included studies, we used a narrative nature of our synthesis; this makes it difficult to draw conclusions about the potential effects of models of care. We addressed this by discussing the findings of the studies for each of the three settings when forming conclusions.
Conclusion and implications
This review highlights the heterogeneity in the research area of multimorbidity. Due to different populations with different conditions, different settings, and use of different models and model elements, it is difficult to conclude and attain valuable evidence regarding effective care models and model elements. Despite the growing number of randomized controlled trials, the evidence regarding effectiveness of care models for people with multimorbidity remains unclear. In this review, 20 of the 30 included studies reported significant improvements in the primary outcome measure; however, it is still not clear which model elements are effective. The results indicate that “doing something” is better than doing nothing. This review has highlighted the need for further research in the area of effective care models for persons with multimorbidity and in multimorbidity in general. It is necessary to design investigations to clinically relevant manifestations of multiple chronic conditions. Further, more research is needed to clarify which model elements are effective and which elements are effective in combination.
Supplemental Material
sj-pdf-1-cob-10.1177_26335565221134017 – Supplemental Material for Models of care for improving health-related quality of life, mental health, or mortality in persons with multimorbidity: A systematic review of randomized controlled trials
Supplemental Material, sj-pdf-1-cob-10.1177_26335565221134017 for Models of care for improving health-related quality of life, mental health, or mortality in persons with multimorbidity: A systematic review of randomized controlled trials by Christian U Eriksen, Nina Kamstrup–Larsen, Hanne Birke, Sofie A L Helding, Nermin Ghith, John S Andersen, and Anne Frølich in Journal of Comorbidity
Supplemental Material
sj-pdf-2-cob-10.1177_26335565221134017 – Supplemental Material for Models of care for improving health-related quality of life, mental health, or mortality in persons with multimorbidity: A systematic review of randomized controlled trials
Supplemental Material, sj-pdf-2-cob-10.1177_26335565221134017 for Models of care for improving health-related quality of life, mental health, or mortality in persons with multimorbidity: A systematic review of randomized controlled trials by Christian U Eriksen, Nina Kamstrup–Larsen, Hanne Birke, Sofie A L Helding, Nermin Ghith, John S Andersen, and Anne Frølich in Journal of Comorbidity
Footnotes
Acknowledgments
We thank Anne Jung, specialist, Charlotte Weiling Appel, registered nurse, and Finn Thomsen Nielsen, specialist, who provided clinical insight and expertise that greatly assisted the research.
Contributor and guarantor information
CUE is the guarantor of the submitted work. AF is the senior author. CUE planned the searches in collaboration with AF; conducted the searches; carried out study selection in collaboration with NKL, NG, and AF; assessed methodological quality in collaboration with SALH and HB; and extracted and synthesized findings in collaboration with AF, NKL, and JSA. CUE and NKL wrote the manuscript. All authors critically revised the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Declaration of conflicting interests
All authors have completed the ICMJE uniform disclosure form at ![]() and declare: CUE and SALH received financial support from the Danish Health Authority; no authors had financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
and declare: CUE and SALH received financial support from the Danish Health Authority; no authors had financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Danish Health Authority. No funding body has influenced the study design; data collection, analysis, and interpretation of data; the writing of the report; and in the decision to submit the article for publication.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Transparency declaration
The guarantor affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned have been explained.
Prospero registration number
CRD42019119490.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.