
Abstract
Objectives:
To explore whether community health worker household-based maternal health visits improve antenatal care and skilled birth attendance among hard-to-reach fishing villages on Lake Victoria, Uganda.
Methods:
This quasi-experimental 18-month prospective study involved 486 consenting women aged 15–49 years, who were pregnant or had a pregnancy outcome in the past 6 months, from 6 island fishing communities. The community health worker household-based intervention (community health workers’ household visits to provide counseling, blood pressure measurement, anemia, and HIV testing) involved 243 women from three fishing communities. Random effects logistic regression was used to determine the association between the community health worker intervention and antenatal care and skilled birth attendance among women who had at least 5 months of pregnancy or childbirth at follow-up.
Results:
Almost all women accepted the community health worker intervention (90.9% (221/243)). Hypertension was at 12.5% (27/216) among those who accepted blood pressure measurements, a third (33.3% (9/27)) were pregnant. HIV prevalence was 23.5% (52/221). Over a third (34.2% (69/202)) of women tested had anemia (hemoglobin levels less than 11 g/dL). The community health worker intervention was associated with attendance of first antenatal care visit within 20 weeks of pregnancy (adjusted odd ratio = 2.1 (95% confidence interval 0.6–7.6)), attendance of at least four antenatal care visits (adjusted odd ratio = 0.9 (95% confidence interval 0.4–2.0)), and skilled birth attendance (adjusted odd ratio = 0.5 (95% confidence interval 0.1–1.5)), though not statistically significant.
Conclusion:
Community health workers have a crucial role in improving early antenatal care attendance, early community-based diagnosis of anemia, hypertensive disorders, and HIV among women in these hard-to-reach fishing communities.
Background
Uganda is still experiencing a critical shortage of health workers who are educated, qualified, and regulated to local and international levels, 1 usually referred to as skilled birth attendants (SBAs). 2 There are about 14.2 skilled health workers per 10,000 population in Uganda, far below the World Health Organization target of 44.5 per 10,000 for sustainable development. 1
SBAs are key in providing comprehensive socially sensitive, human rights-based approach care to women, their babies, families, and communities during pregnancy, childbirth, and after birth.3–5 They identify, manage, or refer women and/or babies with complications for further management. 6 SBAs are vital to support antenatal care (ANC), skilled birth attendance, and postnatal care (PNC), which help in improving maternal-child health outcomes.3–5,7
Over the past 20 years, improvements in the number of births supervised by SBAs in Uganda do not indicate that the country is on course to achieving the reproductive and maternal health-related sustainable development goals (SDGs) targets.8–10
The critical shortage of SBAs is partly contributing to many women dying from pregnancy and childbirth-related causes, at 336 overall deaths per 100,000 live births, much higher than the SDGs target of 70 deaths per 100,000 births.9,10 These maternal deaths could be averted through adequate numbers of SBAs with the necessary equipment, and backing of an effective health system, including transport, and timely referral facilities for emergency care.5,6,11
Having adequate numbers of SBAs is not realizable in the immediate future, especially among rural hard-to-reach island fishing communities (FCs) on Lake Victoria, Uganda. Our work indicates that women in these FCs have a higher proportion not attending ANC, late start of ANC after 20 weeks of being pregnant, and fewer ANC components receipt among those who attend at least four times,12,13 which are precursors for maternal deaths. This may be due to the critical shortage of SBAs in these communities. 14
Task shifting some components of maternal health services to community health workers (CHWs), locally known as village health teams, may improve maternal health services especially ANC and skilled birth attendance in rural hard-to-reach FCs.15–17
CHWs support health, are selected, trained, and work within the communities from which they live. The World Health Organization
18
describes CHWs as ‘‘members of the communities where they work, should be selected by the communities, should be answerable to the communities for their activities, should be supported by the health system but not necessarily a part of its organization, and have a shorter training than professional workers.’’
CHWs provide a wide range of services, including assistance to individuals, families, and communities with disease preventive measures, including facilitating access to health and social services. 19
CHWs have been resourceful in HIV care through engaging individuals and communities to accept and adhere to HIV prevention and treatment interventions, especially in hard-to-reach communities.20–22
The diagnosis and management of non-communicable diseases in rural hard-to-reach settings have been facilitated by the active involvement of CHWs, including counseling, measurement, and linkage to care for diseases like diabetes and hypertension.23,24
CHWs have been in existence following their establishment by the Uganda Ministry of Health in 2001, though serving with challenges. 25
In the presence of an ongoing critical shortage of SBAs, task shifting components of maternal health services may improve maternal health-seeking behavior and avert maternal deaths among island hard-to-reach FCs on Lake Victoria, Uganda.
In this regard, the impact of strengthening the capacity of existing CHWs to conduct household-based HIV testing-counseling (HTC), anemia testing, blood pressure (BP) measurement, and counseling on ANC and skilled birth attendance in FCs was explored. It was based on the premise that CHWs’ strengthened capacity to conduct the said activities will free up SBAs’ time for more technically demanding services, and create more awareness for women to attend ANC and skilled births. It would also help in the early diagnosis and management of anemia, hypertensive disorders, and HIV which are major contributors to maternal deaths.
Methods
Study design
This was a quasi-experimental prospective study involving six islands FCs. Three communities were randomly selected for participants to receive the intervention: a CHW home visit package, consisting of household-based CHW HIV testing, anemia testing, BP measurement, and counseling by CHWs on prenatal, natal, and postnatal maternal–child health issues including skilled attendance. Participants from the other three control communities received standard facility-based maternal health services as provided by the Uganda Ministry of Health guidelines. 26 The study involved 486 consenting women aged 15–49 years, who were pregnant or had a pregnancy outcome in the past 6 months, half of the participants (243) were recruited from the intervention communities, while the other 243 were from the control communities.
Study setting
The study was conducted in six FCs of Kalangala district. Kalangala islands district is one of the hard-to-reach areas in Uganda, with the proportion of women in these islands who receive at least four ANC visits and those assisted by a SBA at birth being lower than the average for other regions in Uganda. 9 These FCs also have higher rates of HIV infection which may negatively impact on the elimination of mother-to-child transmission of HIV efforts.27–29 Selection of these islands has been described elsewhere. 13
CHW intervention
Participants from intervention communities received the CHW home visit package (at least four household visits over 18 months, consisting of one-on-one standardized maternal health promotion messages on the importance of ANC, skilled childbirth, mother and newborn danger signs, PNC, exclusive breastfeeding within 6 months after birth, household-based BP measurement, HTC, and anemia testing by pre-trained CHWs. Through the existing active CHWs in the intervention communities, 11 CHWs were recruited. The CHWs received 10 days hands-on training in HIV counseling and testing, anemia testing, measurement of BP, counseling on maternal pregnancy, birth, newborn danger signs, documentation, and making referrals, based on national guidelines. 30 , 31 The training also included key messages that the CHW should provide to study participants and their spouses about birth preparedness, care-seeking for ANC, delivery, and newborn care. Training was conducted by the research team in collaboration with the Kalangala district health team. CHWs received supplies including calibrated automated BP machines, hemoglobin color scale kits, HIV testing kits per Uganda guidelines,31,32 quarterly support supervision, and refresher trainings. Each CHW was allocated an average of 22 participants, following up the same participants throughout the study. CHWs made household visits within their geographical area (village) to study participants at most once every month and at least four times during the 18 months project duration, documenting information collected at visits in structured notebooks (see supplemental material). The study team reviewed each CHW household visit notebook during field supervisions, with entry into open data kit (ODK) software designed screens done only after books were signed off as complete, without error. CHWs received a monthly field expenses reimbursement of €4.465 per woman they visited for project-related issues.
The postulation was that CHW household visits would improve (1) ANC attendance, (2) skilled birth attendance, (3) uptake of household-based BP measurement, (4) anemia testing, and (5) HTC.
To evaluate the relationship between CHW household visits and attendance to health facilities for ANC and skilled births, one-on-one standardized maternal health promotion messages on the importance of skilled ANC, delivery, and PNC services were provided by the trained CHWs to study participants in the intervention communities.
To understand whether CHW visits improve uptake of household-based measurement of BP, household-based BP measurements were offered by CHWs to participants. BP was measured by a CHW with the participant seated after resting for at least 5 min, using validated OMRON® digital automatic BP machines. The left arm of the participant was placed on a chair or table with the palm facing upward. Three readings, 5 min apart, were then taken. 32 The average of the last two readings (calculated in ODK at data entry) was taken as the final BP reading. Hypertension was defined as an average systolic BP ⩾ 140 mm Hg and/or average diastolic BP ⩾ 90 mm Hg, or currently taking medication for hypertension. 33 The measurements were recorded in the CHW’s notebook (see supplementary material) for each participant and entered in ODK designed data entry forms on computer tablets. Participants with hypertension were referred by CHWs to a health facility level III, IV, or V, of their choice for appropriate management.
To understand whether CHW visits improve household-based anemia testing, anemia testing by CHWs was done using the hemoglobin color scale. 34 Hemoglobin color scale levels less than 11 g/dL were regarded as anemia.34,35 CHWs were trained to refer participants with anemia to the health facilities for further evaluation.
CHWs offered household-based HTC to participants who have voluntarily accepted to be tested, using the finger stick technique in accordance with the national HTC algorithm. 31 The serial HIV testing algorithm was used; where the participant was first tested using the Determine® (Alere Medical Co. Ltd, Chiba, Japan) HIV rapid test kit, if it was negative, the result was reported as negative, and if Determine was positive, STAT-PAK® (Chemo Bio Diagnostic Systems Inc. Medford, NY, USA) HIV rapid test kit was immediately used. If both Determine and STAT-PAK were positive, the result was reported as HIV positive (HIV infected). If the retesting on STAT-PAK showed a negative result, a third tie breaker test, SD Bioline® (Standard Diagnostics Inc. Borahagal-ro, Giheung-gu, Yongin-si, Gyeonggi-do, Republic of Korea, South), was immediately used. If SD Bioline result was negative, the result was reported as negative. If SD Bioline indicated a positive result, the eventual result would be indicated as inconclusive, and a repeat testing would be requested after 14 days. 31 Participants found to be HIV positive were referred to health facilities for further evaluation and management.
Control
Participants from the three control communities received standard maternal health services in any health facility of their choice. There was no training offered to CHWs in the control communities.
Study duration
The study was conducted over 23 months (January 2018 to December 2019); enrollment took 5 months with a follow-up period of 18 months.
Sample size
Calculation was based on individual participant analysis with a two-sided alpha, at 95% confidence level, an 80% power to detect a minimum difference of 14% in the proportion of participants attended to by an SBA during ANC (at least four visits) or childbirth at 18 months, between the intervention and control arms, assuming equal numbers of participants recruited for either arms and a cumulative 24% loss to follow-up, the estimated total sample size was 486 (243 per arm).
Eligibility criteria
Women were eligible if aged 15–49 completed years at enrolment, were pregnant, or had a pregnancy outcome (live birth, still birth, or abortion) in the 6 months prior to enrolment.
Study procedures
Detailed screening and enrolment procedures have been documented elsewhere. 12 Follow-up procedures at 12 and 18 months involved administration of a semi-structured face-to-face questionnaire designed in ODK software, 36 on computer tablets to all participants. The questionnaires were designed using validated tools. 37 Intervention participants were also visited by CHWs during follow-up, measuring their BP, conducting HTC, anemia testing, and counseling on skilled ANC, skilled births, postnatal danger signs, and exclusive breastfeeding during the first 6 months after birth.
Statistical methods
Data management
Direct electronic data capture using ODK software on computer tablets was done, with real-time data review for completeness, accuracy, and subsequent uploading to a cloud-based server. Data were downloaded and aggregated into a data set, re-checked for completeness and accuracy.
Data analysis
This analysis aimed at answering the following research questions:
What proportion of participants in the intervention arm received? CHWs’ household visits CHWs’ household-based BP measurement CHWs’ household-based HIV testing and referral Household-based anemia testing by CHWs
Does the intervention affect the timing of the first ANC visit among those who attend ANC?
Does the intervention improve uptake of Ugandan standard-of-care ANC visit schedule? 26
Does the intervention improve delivery in the presence of a skilled birthing team?
Participants’ baseline and follow-up characteristics were described using counts, percentages, proportions, frequencies, medians, and ranges. Tables were used to make comparisons across intervention and control groups at baseline and at follow-up. The chi-square and Fisher’s exact tests were used to evaluate associations across intervention and control groups in respect to a given characteristic.
Random effects logistic regression was used to determine the association between the intervention (CHW household visits) and attendance of first ANC visit within 20 weeks of being pregnant among those who had an at least 5 months of pregnancy, at least four ANC visit attendance and delivery in the presence of a skilled birthing team as outcomes among women with a childbirth during follow-up. The resulting adjusted odd ratio (AOR) indicates the direction of association, whether the intervention was associated with increased or decreased likelihood of the outcome. Choice of co-variates was based on the measured variables’ relation to the outcomes and intervention from previous literature. These included women’s age groups (15–24 and 25–49 years), highest years of education attained [0 (none), 1–7 years (primary), or 8 or more years (post-primary)], baseline marital status (married and unmarried), main occupation at baseline, duration of community residence (up to 5 years and over 5 years), lifetime births, history of pregnancy loss, presence of a public health (government) facility within the participant community (present or absent), and receipt of components of ANC at attendance.
During estimation of pregnancy incidence, woman years of observation were calculated as reported date of pregnancy by a woman, minus date of enrolment, divided by 365.25. All analyses were done using STATA® version 17 (StataCorp, College Station, TX, USA) software. 38
Results
Participants’ characteristics
At the baseline survey, control participants were older than those in the intervention (mean age, 27.5 versus 26.3 years). There were, however, no differences in study arms by mean age at first pregnancy (17.4 versus 17.4 years, p = 0.63), proportion with at least 8 years of education (46% in the intervention versus 54% for the control, p = 0.49) (see Table 1).
Participants’ baseline characteristics by study arm among 486 women from six island FCs in Kalangala district, Uganda.

Chi-square or Fisher’s exact test.
Standard deviation.
Overall, almost all enrolled participants were followed up at 12 and 18 months, with 91.8% (223/243) from the intervention and 95.1% (231/243) from control communities (see Figure 1).

Study flow diagram.
There were 81 new pregnancies among the 454 participants followed up, with 571.5-woman years of observation, amounting to 14 pregnancies per 100-woman years of observation (95% confidence interval (CI): 12–17).
CHW household visits
Nearly all intervention arm participants (90.9% (221/243)) were visited by CHWs at least once. Over three-quarters (76.1% (185/243)) of these participants received at least four CHW visits. Participants reported 1818 household visits by 11 CHWs during the 18-month period, ranging from 1 to 18 with a median of eight (see Table 2).
Participant characteristics at 18 months among 454 women followed up from six island FCs in Kalangala district, Uganda.

CHW: community health worker; BP: blood pressure.
CHWs’ household-based blood pressure measurement
Almost all participants (97.7% (216/221)) visited by CHWs at least once received household-based BP measurement from CHWs. Over a tenth (12.5% (27/216)) of participants had hypertension, of whom over a quarter (26%, 7/27) were on medication. A third (33.3% (9/27)) of those with hypertension were pregnant during follow-up. Those with hypertension were referred by the CHWs to health facilities for further assessment and management (see Table 2).
CHWs’ household-based HIV testing and referral
Majority of intervention participants (90.5% (200/221)) underwent CHW household-based HTC during the 18 months follow-up, with over a fifth (21% (42/200)) being positive and were referred for further assessment and management. Nearly half of participants who refused to undergo CHW HIV testing throughout the follow-up period were already on antiretroviral therapy (47.6% (10/21)). Overall HIV prevalence among women who received CHW household-based HTC was 23.5% (52/221) (see Table 2).
Household-based anemia testing by CHWs
Anemia testing by CHWs was accepted by almost all intervention participants (91.4% (202/221)) throughout the follow-up period. Hemoglobin (hb) levels among tested participants ranged from 6 to 15 g/dL with a median of 12 g/dL. Over a third of all tested participants (34.2% (69/202)) had anemia (hb less than 11 g/dL). Participants with anemia were counseled by CHWs and referred for further investigation (see Table 2).
Effect of the CHW intervention on ANC and skilled birth attendance
The proportion of intervention versus control participants who had their first ANC visit within 20 weeks of being pregnant increased (from 84.3% (140/166) versus 80.7% (121/150), p = 0.39 at baseline to 87.4% (90/103) versus 77.5 % (86/111), p = 0.06) at 18 months follow-up (see Table 3). The intervention was associated with increased likelihood of first ANC visit attendance within 20 weeks of pregnancy at follow-up (AOR = 2.1 (95% CI: 0.6–7.6)), though not statistically significant (see Table 4 and Supplemental Table 5).
Participant pre- and post-intervention characteristics by study arms.
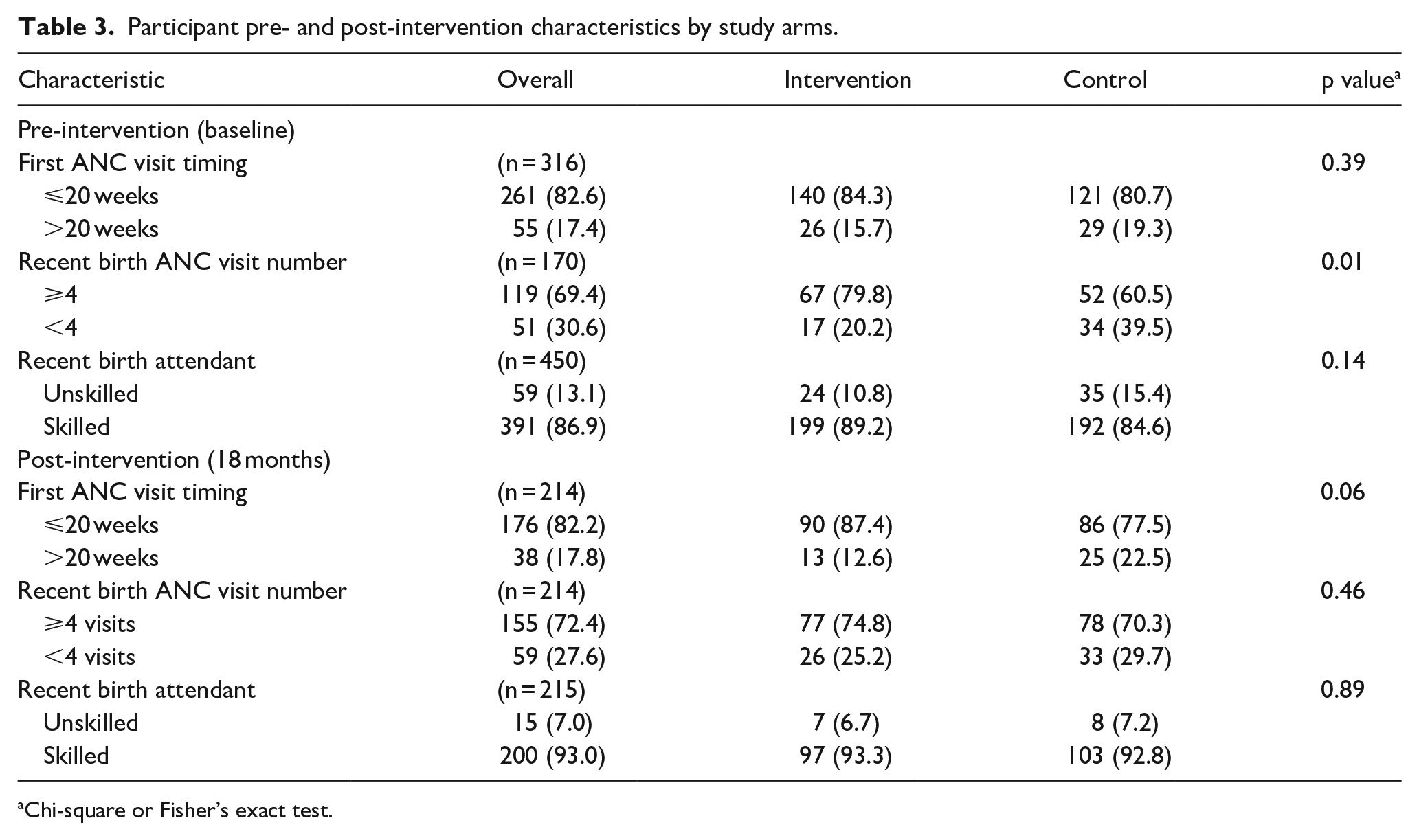
Chi-square or Fisher’s exact test.
Effects of CHW visits among women with a childbirth at 12 months follow-up, after logistic regression.

AOR: adjusted odd ratio; CI: confidence interval.
Among women with at least 5 months of pregnancy.
The CHW household visit intervention was associated with less likelihood of at least four ANC visit attendance (AOR = 0.9 (95% CI 0.4–2.0)). Effect was not statistically significant (see Table 4 and Supplemental Table 6).
The proportion of intervention versus control participants who had a skilled attendant during the most recent childbirth increased (from 89.2% (199/223) versus 84.6% (192/227), p = 0.14) at baseline to 93.3% (97/104) versus 92.8% (103/111), p = 0.89) at 18 months follow-up (see Table 3). The CHW visit intervention was associated with less skilled births attendance among women with a childbirth at follow-up (AOR = 0.5 (95% CI 0.1–1.5)), though not statistically significant (see Table 4 and Supplemental Table 7).
Discussion
This study uniquely highlights the role of CHWs in improving early ANC attendance among women in these hard-to-reach island FCs, though their role in improving the national standard of care ANC visit schedule and skilled births still needs further evaluation.
As is often the case in these FCs, majority of study participants had lower levels of education, not having formally studied beyond 7 years. 39 Education is related to access to maternal health services.40,41
Almost all participants adhered to study follow-up visits at 12 and 18 months despite noted as being mobile. 42 Only a tenth of the participants did not make it for their follow-up visits. This may imply that women in these FCs can be followed up for maternal health interventions. Incidence of pregnancies among participants in the study was higher than in other rural settings, 43 probably due to limited access to contraceptive services, as it has been noted that there is low contraceptive use among these communities. 44
Most participants in the intervention communities agreed to be visited by CHWs for maternal health-related issues, probably because CHWs were well known, having been previously volunteering to provide some services. CHWs’ services have also been found acceptable in similar settings. 45
CHWs’ household-based BP measurements were able to identify participants with hypertension, majority of whom were not on medication, with some being pregnant and were referred for further investigation and management. This facilitated early diagnosis and management of hypertensive disorders among these women. Involvement of CHWs in home-based early diagnosis and management of hypertensive disorders have been shown to cost effectively improve health in other settings.23,24,46
Despite availability of an array of HIV prevention options, the study found that HIV prevalence among participants assessed by CHWs was high. This calls for concerted implementation programs efforts to further dampen the HIV burden in these islands FCs. Household-based HTC by CHWs is feasible and could be an additional healthcare service for prevention of HIV in these hard-to-reach rural areas. CHWs have been previously found to be effective in improving HIV prevention and care in low-income settings.47,48
Anemia was found to be prevalent among study women, comparable to work in other settings, 49 though lower than the national average of 35.7% for islands. 9 This highlights that CHWs could play a crucial role in the early diagnosis and management of anemia among women if trained to do so using less technical equipment, especially in these hard-to-reach communities.
Women who received the CHW household visit intervention were likely to attend the first ANC visit within 20 weeks of pregnancy during follow-up. The intervention seemed to have had a negative impact on attendance of four ANC visits and skilled births among women with a childbirth at follow-up. These findings are in keeping with previous work in other settings which highlighted that CHWs improved ANC, and maternal health.16,50–52 However, others also found no effect of CHWs’ intervention on timing of first ANC visit and attendance of at least four visits. 53 These findings further support evidence on community-based interventions, including active involvement of CHWs to improve early ANC attendance that has been linked to improved maternal health outcomes.51,53–55 The role of CHWs in improving adherence to national ANC visit schedule and skilled births needs further evaluation in these FCs.
The study had some limitations, including the lack of statistical significance of these findings could be that the duration of time for the intervention (18 months), was short, more participants might have had the intention to attend ANC, and have a skilled birth following CHWs’ household visits, but this did not result in statistically significant changes in ANC and skilled births behavior. 56 The intricate synergistic variety of environmental, ecological, political, physical, psychological, economic, social, and cultural issues that could not exhaustively be accounted for in the design of the CHW intervention might have had an impact on the decisions to seek and access ANC more frequently or skilled birth attendance and could be responsible for the findings.57,58 Control participants could have also been motivated to change their behavior during follow-up visits by the study team, though no counseling or healthcare provision was made; although study teams were trained on all study procedures, spill-over bias may have affected our results. Study results might also have been affected by a poor adherence to the positive maternal health behaviors, 57 with the CHW intervention focusing on the reductionist epistemological paradigm to health rather than a much broader consideration of the several complex interlinked factors that might affect adherence to the positive maternal health behaviors. 58 Incentivizing positive maternal health behaviors for different interventions in future studies among these FCs might be more effective in producing significant effects. The study relied on participants’ self-reports for some of the outcomes, which might have been affected by recall bias. Such bias was minimized through using a shorter recall duration during interviews.
Notwithstanding the limitations, this study provides particularly important insights into the role of CHWs in early ANC attendance, early identification of hypertension, anemia, and HTC among women in these hard-to-reach FCs, which might inform the design of maternal healthcare interventions in these settings.
Conclusion
These study findings highlight the importance of CHWs in improving maternal health outcomes in hard-to-reach rural islands on Lake Victoria. CHWs have a crucial role in the improving first ANC visit attendance among island FCs. CHWs could help in the early community-based diagnosis of hypertensive disorders, anemia, and HIV among women in these hard-to-reach island FCs.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221103993 – Supplemental material for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers
Supplemental material, sj-docx-1-whe-10.1177_17455057221103993 for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers by Ali Ssetaala, Julius Ssempiira, Mathias Wambuzi, Gertrude Nanyonjo, Brenda Okech, Kundai Chinyenze, Bernard Bagaya, Matt A Price, Noah Kiwanuka and Olivier Degomme in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221103993 – Supplemental material for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers
Supplemental material, sj-docx-2-whe-10.1177_17455057221103993 for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers by Ali Ssetaala, Julius Ssempiira, Mathias Wambuzi, Gertrude Nanyonjo, Brenda Okech, Kundai Chinyenze, Bernard Bagaya, Matt A Price, Noah Kiwanuka and Olivier Degomme in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057221103993 – Supplemental material for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers
Supplemental material, sj-docx-3-whe-10.1177_17455057221103993 for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers by Ali Ssetaala, Julius Ssempiira, Mathias Wambuzi, Gertrude Nanyonjo, Brenda Okech, Kundai Chinyenze, Bernard Bagaya, Matt A Price, Noah Kiwanuka and Olivier Degomme in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057221103993 – Supplemental material for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers
Supplemental material, sj-docx-4-whe-10.1177_17455057221103993 for Improving access to maternal health services among rural hard-to-reach fishing communities in Uganda, the role of community health workers by Ali Ssetaala, Julius Ssempiira, Mathias Wambuzi, Gertrude Nanyonjo, Brenda Okech, Kundai Chinyenze, Bernard Bagaya, Matt A Price, Noah Kiwanuka and Olivier Degomme in Women’s Health
Footnotes
Acknowledgements
The VIMBA study team (Phiona Nalubega, Gideon Matovu, Judith Namugga, Nusula Nakiragga, Henry Kaluuma, and Joan Nabawanuka) for their contribution. Dr. Francis Xavier Kasujja provided guidance during implementation and writing up of the study. The Uganda Virus Research Institute and UVRI-IAVI HIV Vaccine Program provided administrative and institutional support.
Author contribution(s)
Availability of data and material
The data sets used and analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study and consent methods were approved by Uganda Virus Research Institute Research Ethics Committee, reference number GC/127/17/09/622 and the Uganda National Council of Science and Technology, reference number SS 4444. Women 18 years or older provided documented informed consent prior to participation. Adolescents aged 15 to17 years, if emancipated minors, they provided documented emancipated minor consent and if not emancipated minors, assent, with documented consent from guardians was sought.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the IAVI. IAVI’s work is made possible by the generous support of many donors including: the Bill & Melinda Gates Foundation; the Ministry of Foreign Affairs of Denmark; Irish Aid; the Ministry of Finance of Japan in partnership with The World Bank; the Ministry of Foreign Affairs of the Netherlands; the Norwegian Agency for Development Cooperation (NORAD); the United Kingdom Department for International Development (DFID), and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development (USAID). The full list of IAVI donors is available at ![]() . This study article is made possible by the support of the American People through PEPFAR and USAID. The contents of this article are the sole responsibility of IAVI and co-authors and do not necessarily reflect the views of PEPFAR, USAID, or the United States Government.
. This study article is made possible by the support of the American People through PEPFAR and USAID. The contents of this article are the sole responsibility of IAVI and co-authors and do not necessarily reflect the views of PEPFAR, USAID, or the United States Government.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.