
Abstract
Background:
Short birth intervals (SBI), defined as intervals of less than 33 months between consecutive live births, are a significant public health concern because of their association with adverse maternal and child health outcomes. Somalia has some of the highest maternal and neonatal mortality rates globally, compounded by limited access to family planning services.
Objectives:
This study aimed to provide a descriptive analysis of the prevalence and patterns of SBI among Somali women across regions, offering insight into maternal health policies.
Design:
A descriptive cross-sectional study design was employed.
Methods:
Data from 9288 women aged 15–49 years drawn from the Somali Demographic and Health Survey were analyzed. Descriptive statistics were used to examine the prevalence and distribution of SBI across regions and sociodemographic groups.
Results:
The overall prevalence of SBI was 77%, with regional disparities ranging from 82% in Togdheer and Hiraan to 74% in the Middle Shabelle. Women with no formal education and those in lower wealth quintiles exhibited a higher SBI prevalence than their counterparts. Rural and nomadic populations reported a higher SBI prevalence than urban residents, reflecting potential barriers to accessing family planning services.
Conclusion:
This study highlights the widespread prevalence of SBI in Somalia, with notable variations according to region, education, and economic status. These findings underscore the need for targeted interventions to address the geographic, educational, and economic barriers to family planning access.
Keywords
Introduction
Maternal and child health outcomes remain critical global health priorities, particularly in low- and middle-income countries, where maternal and neonatal mortality rates are disproportionately high. Short birth intervals (SBIs), defined as intervals of less than 33 months between consecutive live births, are strongly associated with adverse maternal and neonatal outcomes. These include increased risks of preterm birth, low birth weight, neonatal mortality, and maternal complications, such as anemia and uterine rupture.1 –3 Addressing SBI is, therefore, essential for achieving Sustainable Development Goal 3, which seeks to reduce global maternal and neonatal mortality by 2030.4,5
In Somalia, maternal and child health indicators are among the poorest in the world. The maternal mortality ratio stands at 692 deaths per 100,000 live births, and the neonatal mortality rate is 39 deaths per 1000 live births.6 –8 Despite these alarming statistics, access to family planning services remains low. Only about 1% of married Somali women use modern contraceptive methods, and the unmet need for family planning is among the highest in sub-Saharan Africa.9,10 These gaps in reproductive healthcare have contributed to the high prevalence of SBI, limiting progress toward improving maternal and child health outcomes.
Sociodemographic factors, such as education, economic status, and place of residence, are important determinants of reproductive health outcomes.11,12 Education plays a pivotal role in empowering women to make informed decisions about family planning and access to services. However, in Somalia, about 85% of women lack formal education, limiting their ability to utilize family planning services effectively.7,13,14 Similarly, economic disparities exacerbate inequities in access to healthcare. Financial barriers, such as the cost of contraceptives and transportation, often deter women from seeking reproductive healthcare, particularly in rural and nomadic settings.15,16
Geographic disparities further complicate the maternal health challenges in Somalia. Women in rural and nomadic areas face greater barriers to healthcare access, including long travel distances, inadequate transportation, and limited healthcare infrastructure.16,17 These barriers contribute to a higher prevalence of SBI in these populations than in urban women. Similar trends have been observed in other low-resource settings, where geographic isolation significantly hinders healthcare utilization.17 –19 Cultural and religious norms also influence reproductive health behaviors in Somalia. Many communities value large family sizes and perceive contraception as unnecessary or contrary to traditional beliefs. Misconceptions about the effects of contraceptives discourage their use. 20 These cultural barriers, combined with Somalia’s fragile healthcare system, pose significant challenges to improving birth spacing and reproductive health outcomes. 21
This study provides a descriptive analysis of the prevalence and sociodemographic patterns of SBIs among Somali women. Given data constraints, this study uses a descriptive approach to examine the prevalence and patterns of SBI. By highlighting regional variations and patterns across different sociodemographic groups, this study aims to offer actionable insights into the context of birth spacing in Somalia. The findings are intended to inform maternal and child health policies and interventions by identifying key areas where family planning and reproductive health services can be strengthened, ultimately reducing maternal and neonatal mortalities.
Methods
Study setting, data source, and sample
This study utilized data from the 2020 Somali Demographic and Health Survey (SDHS), a nationally representative survey conducted by the Somali Government in collaboration with the ICF (formerly Inner City Fund) and United Nations Population Fund (UNFPA). The SDHS data were collected between February 2018 and January 2019. SDHS collects comprehensive data on various health and demographic indicators, with a particular focus on reproductive health. This study focused on women aged 15–49 years who participated in the 2020 SDHS and provided information on their previous birth intervals. In total, 9288 women were included in the analysis. Access to the SDHS dataset was obtained through the official SDHS portal, ensuring adherence to all ethical guidelines and data usage protocols.
Study variables
The primary outcome variable of this study was Inter-birth interval (IBI), defined as the time elapsed between two consecutive live births. To align with WHO recommendations, IBI was categorized into two groups: SBIs of less than 33 months and optimal interbirth intervals of 33 months or more. This categorization is based on the WHO’s recommendation of a minimum 24-month birth-to-pregnancy interval, which, when accounting for a typical 9-month gestation period, corresponds to a 33-month IBI. 22
This study considered a range of sociodemographic factors as the independent variables. These included the woman’s age, education level, wealth index, employment status, distance to the nearest health facility, number of births in the past 5 years, marital status, place of residence (urban or rural), and region. The wealth index variable was derived using principal component analysis based on household asset ownership, as per DHS methodology. 23 Distance to the nearest health facility was categorized based on the women’s self-reported perception. “Big problem” refers to the woman’s perception that the distance to a health facility is a major barrier, based on the standard DHS response category.
Data processing and management
The data were processed and analyzed using Stata 17 statistical software. To account for the complex survey design, sampling weights, primary sampling units, and stratum variables were incorporated into the analysis. Geographic visualization of the prevalence of SBIs across regions was performed using GeoPandas in Python (version 3.10) and GADM shape files. No imputation was required, as the dataset was filtered to include only cases with valid SBI data. All independent variables were complete within this subset, and only complete records were analyzed.
Statistical analysis
Descriptive statistics were employed to characterize the study population and assess the prevalence of SBI across the Somali regions. This included calculating the frequencies and percentages of the categorical variables. Visualizations, such as bar charts and geographical maps, were created to illustrate the distribution of SBIs across different regions. Initial attempts to perform inferential analysis (e.g., logistic regression) were limited by small subgroup sizes and skewed distributions, which yielded statistically insignificant or unstable estimates. As a result, the analysis remained descriptive. Sensitivity analyses were not conducted, as the study was descriptive in nature and relied on complete-case data from a nationally representative sample. This study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies. A completed STROBE checklist is included as Supplemental File 1.
Sociodemographic characteristics of women
This study included 9288 women aged 15–49 years (Table 1). The largest proportion of women was 25–29 years (25.3%), followed by 30–34 years (20.6%). A substantial majority (85.2%) had no formal education, and most (89.1%) were married. The fourth wealth quintile was the largest (20.9%), with the lowest at 23.7%. A considerable proportion (63.7%) reported distance to health facilities as a major problem. Most women were not working (91.4%), and 36.7% had given birth to two children in the last 5 years. The distribution across urban (35.8%), rural (30.7%), and nomadic (33.5%) settings was relatively balanced. Mudug (13.0%) and Galgaduud (10.9%) had the highest regional representation.
Sociodemographic characteristics.
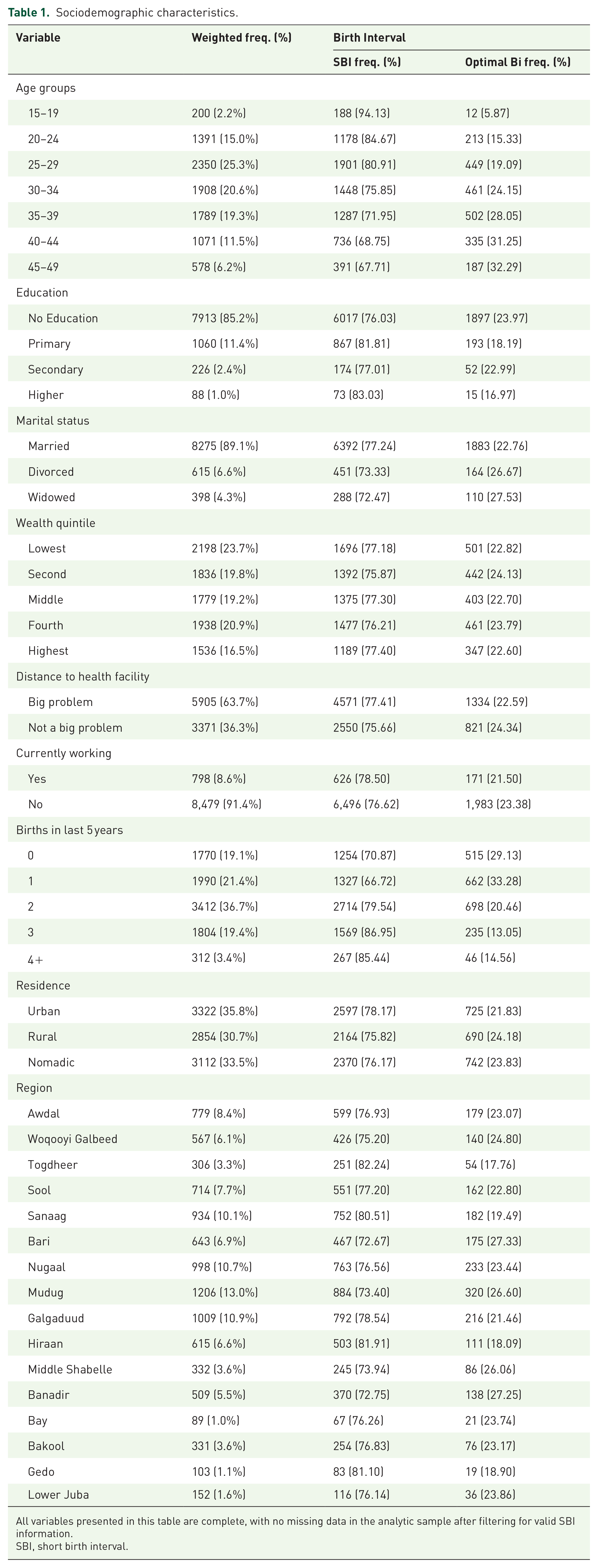
All variables presented in this table are complete, with no missing data in the analytic sample after filtering for valid SBI information.
SBI, short birth interval.
Prevalence of SBI
The overall prevalence of SBIs was 77% (Figure 1), indicating that a significant majority of women in Somalia experience birth intervals of less than 33 months.

Prevalence of SBI.
Regional disparities in SBI
The prevalence of SBI varied across different regions (Figure 2). Several regions exhibited a high prevalence of SBI, including Hiraan (82%), Sanaag (81%), Togdheer (82%), and Gedo (81%). In contrast, regions such as Bari (73%), Mudug (73%), and Banadir (73%) showed a relatively lower prevalence. The geographical distribution of optimal birth intervals across Somalia is shown in Figure 3.

Regional disparities in SBI across Somali regions.

Map of Somalia showing proportion of optimal BI across the regions.
Sociodemographic factors and SBI
Cross-tabulations revealed several associations between sociodemographic factors and SBI prevalence. Younger women, particularly those aged 15–19 years, had a high SBI prevalence (94.13%), with SBI prevalence generally decreasing with increasing age. Women with no formal education exhibited a higher SBI prevalence (76.03%) compared to women with primary (81.81%), secondary (77.01%), or higher education (83.03%). Married women had a higher SBI prevalence (77.24%) than divorced (73.33%) or widowed (72.47%) women. The prevalence of SBI was relatively consistent across wealth quintiles, ranging from 77.18% in the lowest quintile to 77.40% in the highest. Women who reported distance to a health facility as a major problem had a slightly higher SBI prevalence (77.41%) than those who did not (75.66%). Women who were not currently working had a slightly higher SBI prevalence (76.62%) compared to those who were working (78.50%). Women who had given birth to two children in the last 5 years had the highest SBI prevalence (79.54%). SBI prevalence varied by residence, with nomadic women showing the highest prevalence (76.17%), followed by urban (78.17%) and rural (75.82%) residents.
Discussion
This study provides a descriptive analysis of the prevalence and sociodemographic patterns of SBIs among Somali women, highlighting regional disparities and variations across sociodemographic groups. The findings revealed that 77% of women experience SBI, a prevalence consistent with other studies conducted in resource-constrained settings across sub-Saharan Africa.24 –26 These high rates underscore the need for targeted interventions to address the gaps in family planning and maternal healthcare services in Somalia.
Regional disparities were prominent, with Togdheer and Hiraan reporting the highest prevalence of SBI (82%), whereas Bari, Mudug, and Banadir recorded the lowest prevalence (74%). Such variations may reflect differences in the healthcare infrastructure, access to family planning services, and sociocultural practices across regions. These findings align with previous research showing that geographic disparities significantly influence reproductive health outcomes, particularly in low-resource settings, where rural and underserved regions face greater barriers.24,27 –29 The high prevalence of SBI in the central and northern regions may also be associated with the mobility of nomadic populations who face challenges in accessing consistent healthcare services. 16
These descriptive patterns also suggest that education plays a critical role in shaping birth intervals. Women with no formal education exhibited a higher prevalence of SBI than those with some level of education. Education is widely recognized as a determinant of reproductive health, as it enhances women’s knowledge, decision-making capacity, and ability to utilize family planning services.30 –32 However, in this study, 85.2% of the women lacked formal education. Lack of education limits women’s knowledge and use of contraceptives, and is also a proxy for lower autonomy in decision-making. Educated women are more likely to understand and access health services, as well as to negotiate reproductive decisions within their households. This reflects a systematic barrier to improving birth spacing. Similar patterns have been observed in sub-Saharan Africa, where educational attainment is strongly associated with better maternal health outcomes. 26
Unlike education, wealth status showed a relatively consistent SBI prevalence across quintiles. This finding suggests that financial barriers alone may not fully explain birth spacing patterns in this context, especially where access to services is uniformly limited. While this study did not find significant disparities based on wealth quintiles, poverty can still act as a significant barrier to healthcare access in Somalia, potentially limiting women’s ability to afford contraceptives and seek family planning services. Previous research has also highlighted that financial constraints are a key factor contributing to poor reproductive health outcomes in low-income countries.12,33,34 Therefore, addressing broader financial barriers through programs like subsidies for contraceptives or transportation vouchers remains important to improve access to family planning services.
Economic disparities were evident, with women in the lowest wealth quintile reporting SBI more frequently than their wealthier counterparts did. Poverty is a significant barrier to healthcare access in Somalia, limiting women’s ability to afford contraceptives and seek family planning services. Previous research has highlighted that financial constraints are a key factor contributing to poor reproductive health outcomes in low-income countries.12,35,36 Addressing these disparities through financial support programs, such as subsidies for contraceptives or transportation vouchers, could help reduce the economic barriers to family planning.
Place of residence was another critical factor, with a higher SBI prevalence observed among nomadic women compared to rural and urban populations. Nomadic populations face unique challenges, including mobility, cultural resistance to contraception, and limited access to healthcare infrastructure.16,34 Expanding mobile health services and community-based family planning programs can help bridge the healthcare gap in these populations. Cultural and religious norms likely play a significant role in influencing attitudes toward birth spacing. In Somali communities, large families are often culturally valued, and contraception may be stigmatized or viewed as contrary to religious teachings. 37 Similar barriers have been documented in other predominantly Muslim settings, where traditional norms and misconceptions about contraception hinder family planning.38,39 Engaging religious and community leaders in culturally sensitive family planning campaigns could help address these challenges and promote optimal birth spacing. 40 In addition, cultural practices such as male-dominated decision-making (paternalism) and religious beliefs may restrict women’s access to family planning. In some Somali communities, women’s participation in education is limited due to these norms, reducing their autonomy in reproductive decisions. 41 Addressing SBIs must therefore consider social norms that disempower women.
These findings emphasize the need for regionally tailored, community-centered interventions to address the high prevalence of SBI in Somalia. While this study provides a descriptive overview, further research is needed to explore the underlying factors influencing birth intervals and design effective, evidence-based interventions. It is important to acknowledge certain limitations of this study. Although the use of DHS data minimizes selection bias through standardized sampling methods, potential recall bias cannot be entirely ruled out, especially in women’s reports of birth dates. However, the reliance on complete records and standardized DHS data collection enhances the validity of findings. Nonresponse and missing data were handled by restricting the analysis to cases with complete SBI and sociodemographic information. Despite these limitations, this study provides critical baseline information to inform maternal health policies and interventions.
Conclusion
SBIs are highly prevalent in Somalia, especially among women with no education, in poor households, and in rural or nomadic settings. Expanding family planning access through targeted interventions, such as prioritizing mobile health services for nomadic populations (with 76% SBI prevalence) and implementing education programs in regions, such as Mudug and Hiraan, where low literacy and high SBI co-occur, is essential to improving maternal and child health outcomes.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251364403 – Supplemental material for Prevalence and regional patterns of short birth intervals among women in Somalia
Supplemental material, sj-docx-1-reh-10.1177_26334941251364403 for Prevalence and regional patterns of short birth intervals among women in Somalia by Salad Halane, Abdiwali Mohamed Ahmed, Mohamed Mustaf Ahmed, Jamilu Sani, Jamal Hassan Mohamoud, Abdihakim Elmi Abdishakur, Mustaf Mohamed Ibrahim and Najib Isse Dirie in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
The authors acknowledge the Somalia National Bureau of Statistics for providing the data available for this study.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.