
Abstract
Introduction:
Preterm birth, delivery before 37 weeks of gestation, affects 15 million births globally and causes 1.1 million under-five deaths annually. In Somalia, decades of civil war have severely weakened the healthcare infrastructure, posing significant challenges to maternal and neonatal healthcare. However, data on preterm birth and its determinants in Somalia remain limited.
Objective:
This study examines the prevalence and determinants of preterm birth among women delivered at the Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital.
Design:
Retrospective cross-sectional study.
Methods:
A retrospective review of 1900 medical records from January to December 2022 was conducted. Data were analyzed using Stata 17, with logistic regression employed to identify significant determinants of preterm birth. The Hosmer–Lemeshow test (p = 0.64) was used to assess model fit, and statistical significance was determined at p < 0.05.
Results:
The prevalence of preterm birth was 17.5% (95% confidence interval: 15.8%–19.3%), which aligns with similar studies in Ethiopia (16.1%–16.3%) and Malawi (16.3%), but is lower than in Uganda (24.6%) and Kenya (20.2%). Maternal age below 20 years (adjusted odds ratio = 2.4; 95% confidence interval: 1.34–4.17; p = 0.003), absence of antenatal care visits (adjusted odds ratio = 16.4; 95% confidence interval: 10.96–24.48; p < 0.001), and fewer than four antenatal care visits (adjusted odds ratio = 4.1; 95% confidence interval: 2.66–6.47; p < 0.001) were significant predictors of preterm birth. Obstetric complications such as antepartum haemorrhage (adjusted odds ratio = 12.3; 95% confidence interval: 5.75–26.36; p < 0.001), pregnancy-induced hypertension (adjusted odds ratio = 6.0; 95% confidence interval: 3.77–9.56; p < 0.001), and premature rupture of membranes (adjusted odds ratio = 23.2; 95% confidence interval: 12.60–42.71; p < 0.001) were also significant determinants. Additionally, severe anaemia (adjusted odds ratio = 1.8; 95% confidence interval: 1.06–2.97; p = 0.030) and multiple gestations (adjusted odds ratio = 9.7; 95% confidence interval: 4.27–21.97; p < 0.001) were associated with preterm birth.
Conclusion:
The study highlights the high prevalence of preterm birth and identifies significant factors, including inadequate antenatal care visits, pregnancy complications, and multiple gestations. Strengthening antenatal care services, early risk detection, and targeted interventions are critical for reducing preterm birth rates in Somalia.
Introduction
Preterm birth (PTB), defined by the World Health Organization (WHO) as delivery occurring after 24 weeks but before 37 weeks of pregnancy, or 259 days from the first day of a woman’s last menstrual period, is a significant global health concern. 1 PTB is categorized into three groups: extremely preterm (<28 weeks), very preterm (28–32 weeks), and moderate-to-late preterm (32–37 weeks). 2
PTB represents a critical global public health challenge, with ~15 million cases occurring annually, leading to 1.1 million deaths among children under the age of 5. 3 The prevalence of PTB varies significantly across regions, with Africa exhibiting the highest rates worldwide, 11.9% in Africa, 10.6% in North America, and 6.2% in Europe.4,5 Collectively, Southeast Asia and Africa account for over 85% of all PTBs.6,7 Notably, sub-Saharan Africa and South Asia together account for more than 60% of global PTBs and 80% of PTB-related deaths annually.8,9 High PTB rates are reported in Kenya (18.3%), 10 Malawi (16.3%), 11 and the Somali–Ethiopia region (12.3%). 12
Numerous factors, including previous PTBs, multiple pregnancies, cervical insufficiency, smoking, chronic cough, short interpregnancy intervals, anaemia, urinary tract infections (UTIs), and complications such as pregnancy-induced hypertension (PIH), premature rupture of membranes (PROMs), intrauterine growth restriction, and congenital anomalies of the foetus, are associated with increased PTB risk. Lifestyle-related risk factors such as low pregnancy weight and substance use during pregnancy are also known contributors to PTB.13 –17 Identifying these risk factors is crucial for developing public health interventions to reduce PTB rates in low-income countries. 18
Three decades of civil conflict have severely compromised the nation’s healthcare infrastructure, leading to fragmented service delivery and profound implications for maternal and neonatal health outcomes.19,20 Current data indicate an alarming neonatal mortality rate of 26.5%, with prematurity emerging as a primary contributor to these deaths. 21 The healthcare landscape in Somalia faces unique challenges that increase the PTB burden, including critical shortages of skilled healthcare workers, limited access to prenatal services, and inadequate medical infrastructure, particularly in rural areas. 22 Cultural practices such as female genital mutilation, which affects an estimated 98% of Somali women, 23 could influence the PTB rate. Despite these challenges, limited data exist on the prevalence and determinants of PTB, which poses challenges to formulating evidence-based interventions.
To the best of our knowledge, this study represents the first investigation of PTB in Somalia, focussing on Mogadishu’s Somali Turkish Training and Research Hospital, a major tertiary referral centre. Our research aimed to determine the prevalence of PTB and identify associated risk factors among mothers. The findings provide crucial baseline data to inform evidence-based interventions and policy development for reducing the PTB burden in Somalia. These findings are relevant and vital for achieving Sustainable Development Goal 3, which targets a reduction in neonatal mortality to 12/1000 live births by 2030. 24
Materials and methods
Research design, setting, and period
A retrospective cross-sectional study aimed to effectively utilize existing hospital records to estimate the prevalence and factors associated with PTBs at the Mogadishu Somali Turkey Training and Research Hospital in Mogadishu, Somalia. This hospital serves ~2.7 million individuals from the surrounding region, primarily from lower and middle socioeconomic backgrounds. The maternity ward manages around 150–170 deliveries monthly and provides comprehensive care to mothers and their newborns.
Data for this investigation were obtained from electronic medical records spanning 1 year, from January to December 2022. During this time, 1938 deliveries took place at the hospital. After excluding 38 cases due to incomplete records, the final analysis comprised 1900 cases, yielding a response rate of 98%. In the writing of this study, we referred to the Strengthening Reporting of Observational Studies in Epidemiology guidelines. 25
Inclusion and exclusion criteria
Inclusion criteria: Women who delivered a live neonate before 37 weeks of gestation at the hospital within the study period.
Exclusion criteria: Records with incomplete key variables, stillbirths, and miscarriages were excluded from the study.
Data collection sources and variables
Data were extracted from various hospital records, including medical records, delivery registers, antenatal care (ANC) records, and admission records, encompassing multiple variables across several categories. Specifically, the sociodemographic variables included maternal age, educational level, and residence. Furthermore, maternal and obstetric factors included the number of ANC visits, parity, gravidity, prolonged labour, cord prolapse, mode of delivery, PROM, and the onset of labour. In addition, the medical conditions examined included PIH, antepartum haemorrhage, gestational diabetes mellitus, UTIs, anaemia, and oligohydramnios. Foetal-related factors included birth weight, congenital anomalies, malpresentation, multiple gestations, and neonatal sex. Notably, PTB in this study was defined as a live birth occurring before 37 weeks of gestation.
Outcome definition
In this study, PTB was defined as live birth occurring before 37 completed weeks of gestation, excluding stillbirths and terminations.
Operational definition
Data processing and quality assurance
To ensure data quality, a standardized data extraction form was developed and used for systematic data collection. Data collectors underwent a 1-day training session to familiarize themselves with the extraction form and study objectives. The training emphasized the importance of accuracy, consistency, and completeness in data collection.
Data from the medical records were carefully reviewed for completeness and consistency. Records with missing information were excluded from the analysis. To minimize errors during data transfer, double data entry was performed. Additionally, the researcher rechecked a random sample of 10% of records to ensure data accuracy.
Severe anaemia was defined as a haemoglobin level of <7.0 g/dL, by the WHO classification for pregnant women. 26
PIH is defined as the new onset of hypertension (systolic blood pressure ⩾140 mmHg and/or diastolic blood pressure ⩾90 mmHg) occurring after 20 weeks of gestation in a previously normotensive woman, without proteinuria or other signs of preeclampsia. 27
Ethics considerations
The Institutional Ethics Committee of the Mogadishu Somalia Turkish Training and Research Hospital granted ethical approval for this study (ref. no: MSTH/8128). Given the retrospective nature of the study, which involved the use of existing medical records without direct patient contact, the Ethics Committee waived the requirement for written informed consent. All data were anonymized and handled strictly by established ethical research standards.
Statistical analysis
Data analysis was conducted using Stata 17 software (StataCorp LLC, College Station, TX, USA). Descriptive statistics were utilized to summarize the data, including the mean, standard deviation, frequency, and percentage. Logistic regression was employed to examine the associations between PTB and various risk factors, calculating crude odds ratios (ORs) and adjusted ORs (AORs) along with 95% confidence intervals (CIs). Potential confounders were identified through bivariate analyses, wherein variables with a p ⩽ 0.2 were considered for inclusion in the multivariable logistic regression model. These variables were entered simultaneously into the multivariate model to adjust for their potential confounding effects. This approach ensured that the AORs accurately reflected the independent association of each predictor with PTB, while accounting for the influence of other variables within the model. Interaction terms were analyzed for potential confounders, but none were found to be statistically significant (p > 0.05).
To assess multicollinearity, variance inflation factors (VIFs) were computed for all variables included in the multivariable model. Since all VIFs were below 5, no significant multicollinearity was detected. A correlation matrix is provided in the Supplemental Appendix 1 for further reference. Model fitness was evaluated using the Hosmer–Lemeshow goodness-of-fit test, confirming the goodness of fit with a p = 0.64, indicating that the model appropriately fits the data. Statistical significance was established at p < 0.05.
Results
Sociodemographic characteristics
The mothers had a mean age of 28.12 years, with a standard deviation of ±0.12 years. Most mothers (60.3%) were aged 21–30 years, followed by those aged 31–40 years (31.5%). For education, 40.3% had a primary education, whereas 30.0% had no formal education. Most mothers (93.3%) were from urban areas (Table 1).
Sociodemographic characteristics of respondents.

CI: confidence interval.
Maternal and obstetrical factors
Among mothers, 54.4% had four or more ANC visits. Most were multipara (75.3%) or multigravida (77.1%). Vaginal delivery was the most common mode of delivery (63.0%). PROM occurred in 4.5% of the cases, and labour was induced in 14.8% (Table 2).
Maternal and obstetrical factors.
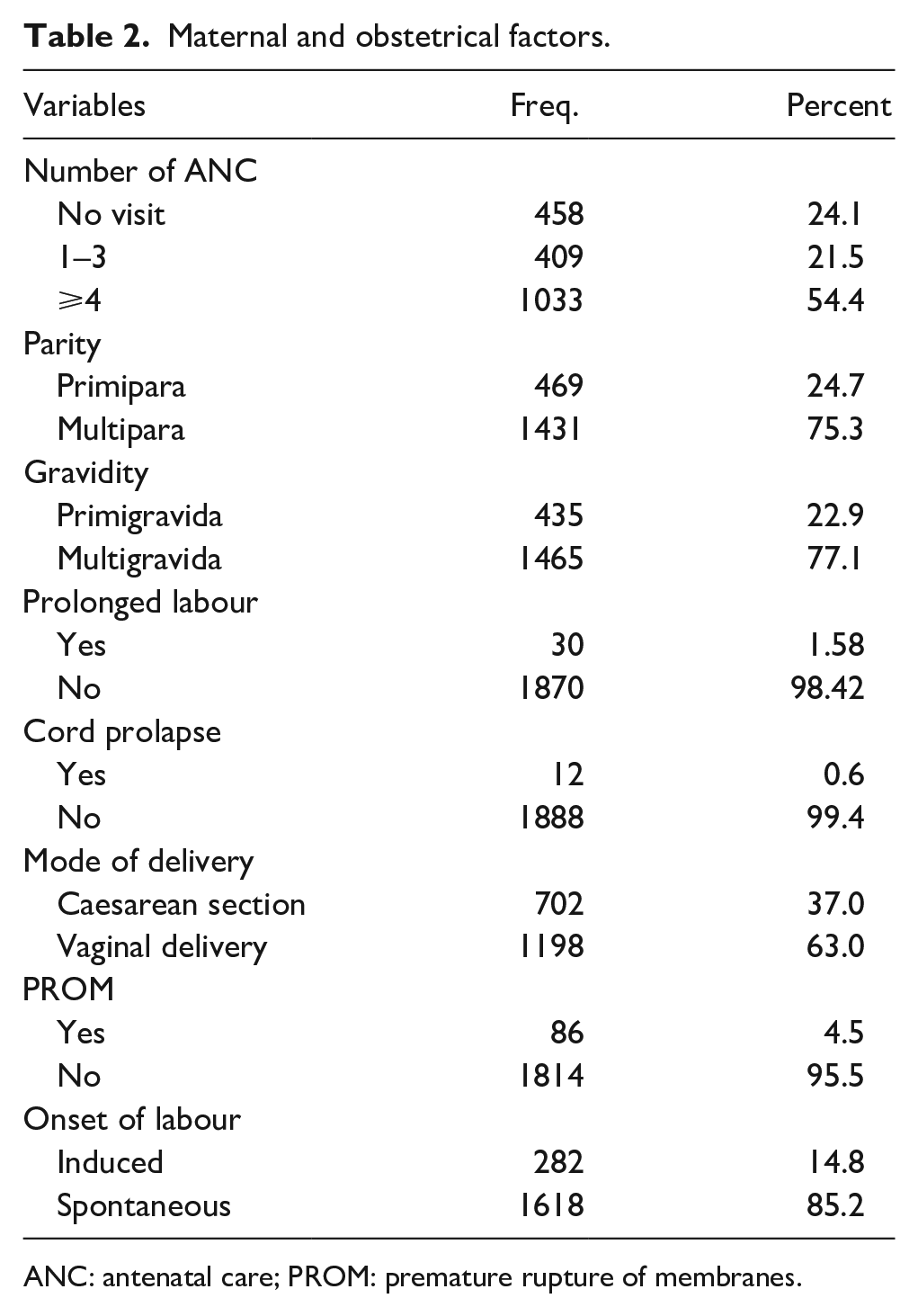
ANC: antenatal care; PROM: premature rupture of membranes.
Medical and foetal-related factors
UTIs were the most prevalent medical condition (21.0%), followed by PIH (7.0%) and anaemia (6.6%). Low birth weight (<2500 g) was observed in 17.3% of the neonates. Multiple gestations occurred in 2.4% of the pregnancies, and 53.3% of the neonates were male (Table 3).
Medical and foetal-related factors.
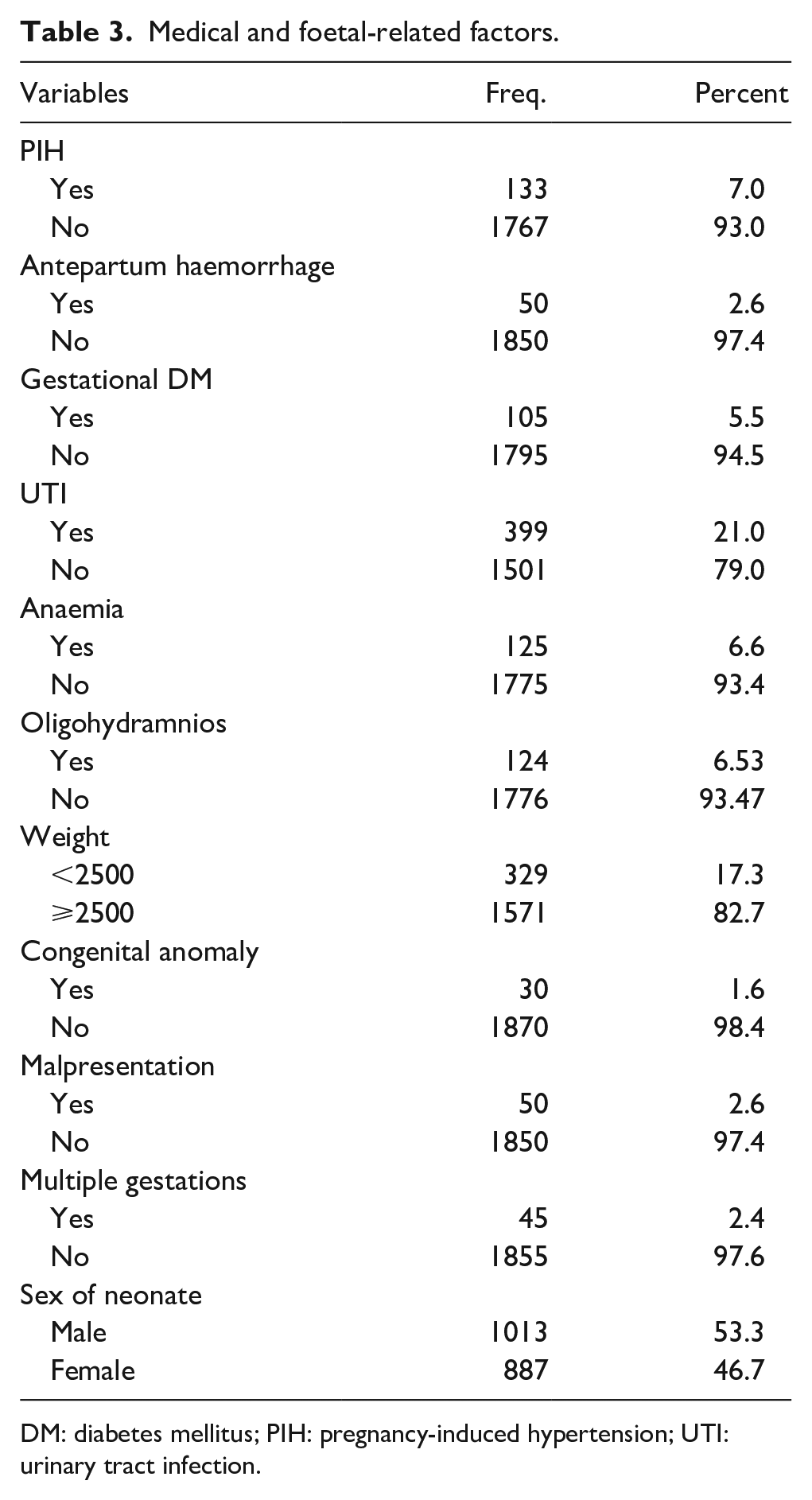
DM: diabetes mellitus; PIH: pregnancy-induced hypertension; UTI: urinary tract infection.
Prevalence of PTBs
In this study, the prevalence of PTB was 17.5%, with a 95% CI of 15.8%–19.3% (Figure 1).

Prevalence of preterm birth among deliveries at Mogadishu Somali Turkey Recep Tayyip Erdogan Hospital (N = 1,900).
Factors associated with PTB
Compared with mothers aged 31–40 years, mothers under 20 years were 2.4 times more likely to have a PTB (AOR = 2.4; 95% CI: 1.34–4.17; p = 0.003). Additionally, those who did not attend any ANC visits were significantly more likely to experience PTBs, with a 16.4-fold increase in risk compared with mothers who attended four or more visits (AOR = 16.4; 95% CI: 10.96–24.48; p < 0.001). Induced labour also contributed to an elevated risk, making mothers nearly 2.9 times more likely to deliver preterm than those with spontaneous labour onset (AOR = 2.9; 95% CI: 1.99–4.20; p < 0.001). Mothers who experienced antepartum haemorrhage had a substantially greater risk of PTB, with a 12.4-fold greater likelihood than those without haemorrhage (AOR = 12.3; 95% CI: 5.75–26.36; p < 0.001). Severe anaemia was another factor, anaemic mothers were 1.8 times more likely to deliver preterm than non-anaemic mothers (AOR = 1.8; 95% CI: 1.06–2.97; p = 0.030). PIH was associated with a sixfold increase in the likelihood of PTB (AOR = 6.0; 95% CI: 3.77–9.56; p < 0.001), and mothers with PROM were 23.32 times more likely to deliver preterm than those without PROM (AOR = 23.2; 95% CI: 12.60–42.71; p < 0.001). Finally, multiple gestations were a significant risk factor, with mothers with multiple gestations being 9.7 times more likely to have a PTB than those with singleton pregnancies (AOR = 9.7; 95% CI: 4.27–21.97; p < 0.001; Table 4).
Factors associated with preterm birth.
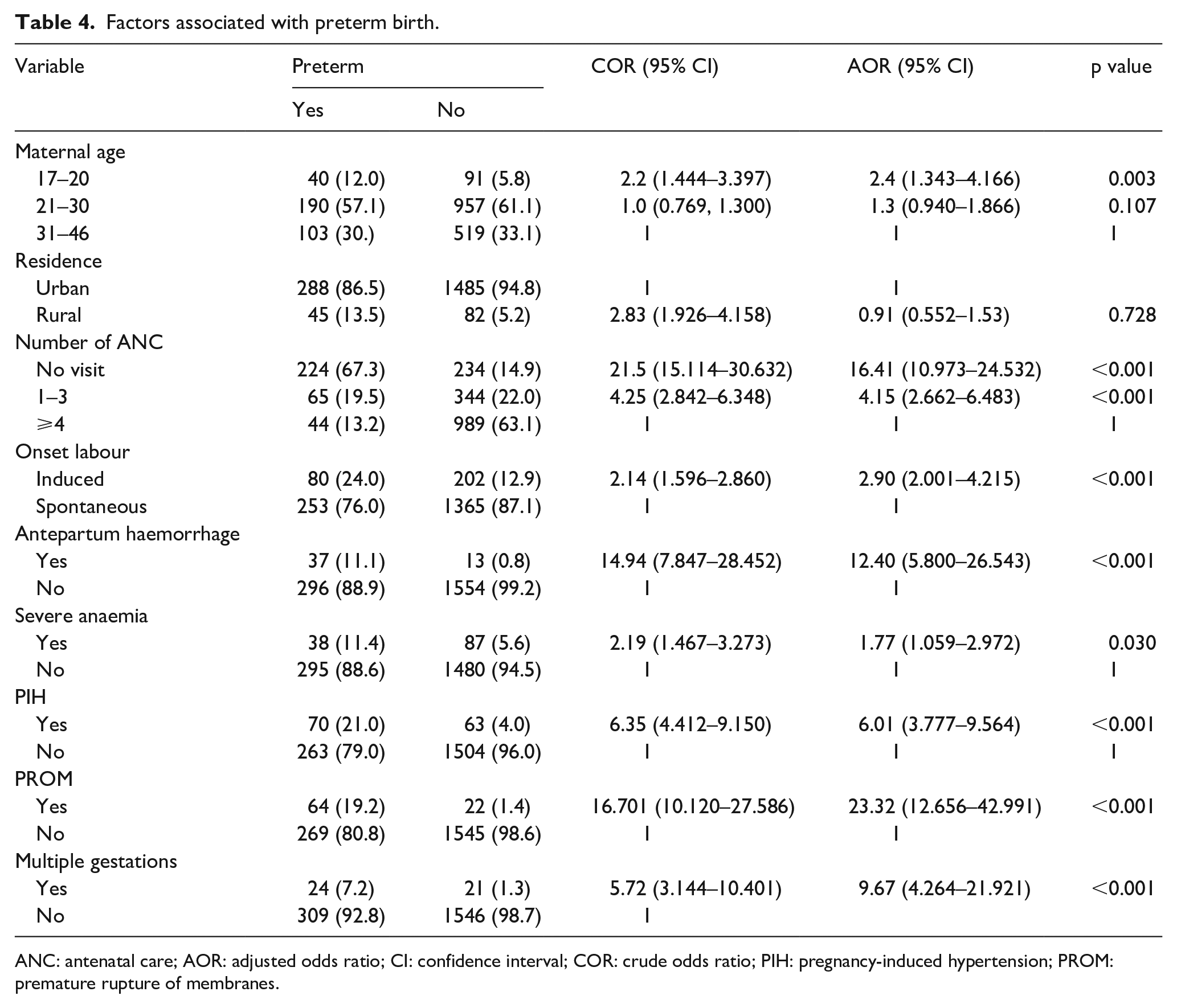
ANC: antenatal care; AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; PIH: pregnancy-induced hypertension; PROM: premature rupture of membranes.
Discussion
This study assessed the prevalence of PTB and associated factors. During the study period, the overall prevalence of PTBs was 17.5% (95% CI: 15.8%–19.3%). This finding is consistent with studies from other sub-Saharan countries such as Ethiopia,2,28 and Malawi, 11 but it is higher than the rate reported in Brazil. 29 This difference is likely attributed to study settings, geographic area variations, and differences in service quality.
Mothers under 20 years of age had two and a half times greater odds of having a PTB than those aged 31–40 years. This finding is in line with those of studies from East Africa, 30 Ethiopia, 31 India, 32 and Canada. 33 The increased risk of PTB in younger mothers may be linked to the underdevelopment of their reproductive organs.
Additionally, those who did not attend ANC visits were significantly more likely to experience PTBs. This finding is comparable to the results of studies conducted in Iran, 34 Ghana, 35 and Ethiopia.36,37 This might be because having ANC enhances health promotion and detects and prevents complications related to preterm delivery at the earliest point. In Somalia, the provision of ANC services faces significant challenges due to cultural traditions, financial constraints, and ongoing conflict. Customs, such as early marriage and preference for traditional birth attendants, deter women from accessing medical care. Additionally, the scarcity of trained healthcare professionals, especially in rural regions, further limits the availability of high-quality ANC services.
Induced labour also contributes to an elevated risk, making mothers nearly 2.9 times more likely to deliver preterm than those with spontaneous labour onset. This finding is consistent with similar studies conducted in Ethiopia38,39 which may be because induced labour is often necessary owing to maternal or foetal complications, which increase the risk of PTB.
Mothers who experienced antepartum haemorrhage had a substantially greater risk of PTB. This finding is consistent with that of a study conducted in East Africa, 30 Kenya, 10 and Ethiopia.10,30,40,41 This could be due to decreased placental blood flow, which affects the exchange of nutrients and oxygen between the mother and foetus. As a result, foetal growth restriction occurs, increasing the likelihood of PTB.
This study revealed that PIH was significantly associated with an increased likelihood of PTB. This finding is supported by studies conducted in East Africa, 30 Somalia, 42 Kenya, 43 Ethiopia,36,44 Nigeria, 45 Ghana, 35 and Iran. 46 This might be due to vascular damage to the placenta caused by PIH, which results in preterm labour and delivery.
Mothers with anaemia were found to have a greater likelihood of preterm delivery than those without anaemia. This observation aligns with the findings of other studies in Ethiopia, 28 Tanzania, and Nepal. 47 This may be due to a reduced blood supply to the placenta, resulting in placental insufficiency. Under normal physiological conditions, the placenta facilitates the transfer of oxygen and essential nutrients from the mother to the foetus via maternal haemoglobin. However, when the blood supply decreases, the placenta detaches from the uterine wall, leading to premature labour and delivery.
Women who experienced PROM had a greater likelihood of delivering PTBs than those without PROM. These findings align with research conducted in various African countries, including Ethiopia, 36 Kenya, 10 and Nigeria. 45 A possible explanation for this phenomenon is that extended PROM creates conditions favourable for microorganisms to travel upwards into the uterus, potentially leading to intrauterine infections.
This study revealed that multiple gestations are strongly associated with PTB. This finding was corroborated by the results of studies conducted in Ethiopia,28,36 Kenya, 10 and Malaysia. 48 Multiple pregnancies are associated with an increased risk of premature birth due to uterine overdistension, which may contribute to mechanical and hormonal changes that increase the likelihood of spontaneous preterm labour. However, the exact mechanisms remain a subject of ongoing research, with evidence suggesting a combination of mechanical stretch, inflammatory processes, and hormonal signalling. This study has significant strengths, including its large sample size. This study provides valuable insights into the occurrence and risk factors of PTB in Mogadishu.
Limitations
This study has several limitations that should be considered when interpreting the findings. Firstly, its retrospective design relied on pre-existing medical records, which limited control over data quality and completeness. Secondly, there is a potential for information bias, as certain variables may have been underreported or misclassified due to inconsistent documentation practices. Thirdly, selection bias is a concern, as the study was conducted in a single tertiary hospital, which limits the generalizability of the results. Although utilizing medical records reduced recall bias compared to participant interviews, the possibility of data gaps and entry errors persists. Lastly, the study included all available records (1900 cases), but a formal power analysis was not conducted to determine the optimal sample size. This may have affected the statistical power of some associations, potentially leading to underestimation or overestimation of certain effects.
Conclusion
The PTB rates reported in this study were higher than those reported for sub-Saharan Africa and other study regions, highlighting a substantial burden in the Somali context. Factors such as inadequate ANC, PROM, young mothers, pregnancies with multiple gestations, PIH, and antepartum haemorrhage were significantly associated with the risk of PTB. Addressing these risks requires strengthening ANC coverage, improving healthcare providers’ capacity to detect and manage pregnancy complications, and overcoming sociocultural and systemic barriers to maternal healthcare access. The study emphasizes the need for enhanced ANC services by implementing community outreach programmes, providing midwifery nursing training, and promoting public health education to raise awareness of pregnancy risk and timely utilization of services. These interventions are essential not only for improving maternal and neonatal outcomes but also for advancing progress towards achieving Sustainable Development Goal 3, which aims to reduce neonatal mortality by 2030. Furthermore, the findings of this study provide a foundation for future research aimed at identifying context-specific barriers to care and evaluating innovative, community-based, and technology-driven interventions. Multicentre and longitudinal studies are recommended to validate these findings and support the development of comprehensive, evidence-based maternal and neonatal health policies.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251350529 – Supplemental material for Preterm birth in Mogadishu, Somalia: Burden and determinants from a retrospective cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057251350529 for Preterm birth in Mogadishu, Somalia: Burden and determinants from a retrospective cross-sectional study by Hiba Bashir Hassan, Yasmin Bashir Hassan, Yahye Sheikh Abdulle Hassan, Rahma Yusuf Haji Mohamud, Abdirahman Mohamed Hassan Dirie, Ibrahim Mohamed Hirsi and Asha Abdullahi Barud in Women’s Health
Footnotes
Acknowledgements
The authors would like to thank the administration and staff of the Somali Turkey Training and Research Hospital for their support and cooperation during the study. Special thanks go to the research assistants and participants who made this study possible.
ORCID iDs
Ethical considerations
The Institutional Ethics Committee of the Mogadishu Somalia Turkish Training and Research Hospital granted ethical approval for this study (ref. no: MSTH/8128). All data were anonymized and handled strictly by established ethical research standards.
Consent to participate
Given the retrospective nature of the study, which involved the use of existing medical records without direct patient contact, the Ethics Committee waived the requirement for written informed consent.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.