
Abstract
Background:
The rising rate of cesarean sections (CSs) has become a global concern due to its implications for maternal and neonatal health. The World Health Organization recommends that CS rates should not exceed 10–15% at the population level. However, many countries report rates well above this threshold.
Objectives:
To evaluate CS rates using the Robson Ten Group Classification System (TGCS) and identify the major contributing groups to develop targeted strategies for reducing unnecessary cesarean deliveries.
Design:
A retrospective clinical audit based on standardized classification and descriptive analysis.
Methods:
This retrospective audit was conducted using hospital delivery records from January 1st to December 31st, 2022, at the Department of Obstetrics and Gynecology, Holy Family Hospital, Karachi, Pakistan. All CSs were categorized into 10 groups using the Robson classification system. Descriptive statistics were used to determine group size, CS rate within each group, relative contribution to the overall CS rate, and absolute group contribution.
Results:
A total of 1464 deliveries occurred during the study period, including 507 CSs. Of these, 48.8% were elective and 51.2% were emergency CS. The major contributors to the CS rate were group 5 (51.9%), group 2 (18.5%), and group 10 (14.4%). The leading indications for cesarean delivery were previous CS (32.3%), non-progress of labor (21.15%), and cephalopelvic disproportion (16.92%).
Conclusion:
Targeted strategies such as promoting vaginal birth after cesarean, implementing standardized labor monitoring protocols, and strengthening antenatal counseling can help reduce unnecessary CS while maintaining maternal and neonatal safety.
Introduction
The increasing rate of cesarean sections (CSs) is a significant concern for healthcare providers worldwide. The World Health Organization (WHO) recommends that CS rates should not exceed 10%–15% at the population level, as there is no evidence that higher rates are associated with better maternal or neonatal outcomes. 1 However, the rate of CS varies widely across different regions, and in many areas, it is significantly higher than the recommended threshold. 2 In 2021, the global rate of CS was 21.1%. Betran et al. projected that the rate of CS would reach 30% by 2030. 3 Over the past three decades, global CS rates have risen substantially, increasing from approximately 7% in 1990. 4 In several middle- and high-income countries, this rate now exceeds 23%, 5 prompting growing concern about unnecessary surgical deliveries. In South Asia, and particularly in urban tertiary care settings in Pakistan, this trend has mirrored global patterns, driven by both clinical and nonclinical factors.
In Pakistan, the rate of CS has been increasing steadily over the past decade, with one study reporting a rate of 40% between 2017 and 2018. 6 This trend is particularly concerning as the country has a high burden of maternal and neonatal mortality and morbidity, and CS is associated with an increased risk of adverse outcomes for both mothers and infants.7,8 With the gradual surge in CS rates, the incidences of Morbidly Adherent Placenta or Placenta Accreta also increase, this results in a bad prognosis and is associated with maternal and fetal death. 9
While CSs can be lifesaving in certain situations, their overuse can lead to increased maternal morbidity and mortality, longer hospital stays, and higher healthcare costs. 10 Gibbons et al. estimated in 2010 that the global excess CS amounted to USD 2.32 billion. 11
In addition, the incidence of neonatal respiratory complications such as transient tachypnea, surfactant deficiency, and pulmonary hypertension is higher, thus indicating an elevated risk. 12 Therefore, it is important to investigate the factors contributing to the increasing rates of CSs and to identify effective strategies for reducing their unnecessary use.
To address this issue, healthcare providers must identify the factors contributing to the high rate of CS and develop strategies to reduce unnecessary CS. The Robson classification system is a widely used tool for assessing and comparing CS rates based on the indications and patient population across different hospitals and obstetric populations. It is a simple and standardized classification system that categorizes all deliveries into 10 mutually exclusive groups based on 5 obstetric characteristics: parity, previous CS, onset of labor, fetal presentation, and gestational age. 13 This classification system allows for the identification of groups of women with similar obstetric characteristics and enables comparisons of CS rates within and between groups. The Robson classification system has been adopted by the WHO and is recommended as a valuable tool for evaluating obstetric care practices and improving the quality of care. 1
In this article, we present the results of an audit of the CS rate at an obstetrics and gynecology department in a tertiary care hospital in Karachi, Pakistan, using the Robson classification system. The significance of this audit lies in its potential to provide valuable insights into obstetric care practices and CS rates at this hospital. This audit report can help clinicians identify areas for improvement in their obstetric care practices and facilitate the development of strategies to optimize obstetric care and reduce CS rates, thereby improving maternal and neonatal outcomes. Furthermore, this audit report can serve as a benchmark for other hospitals in the region and beyond to evaluate their own obstetric care practices and CS rates, ultimately contributing to the improvement of obstetric care on a larger scale.
Methods
Study design and participants
A retrospective study utilizing hospital records was conducted from January 1st, 2022, to December 31st, 2022, at the Department of Obstetrics and Gynecology in Holy Family Hospital, Karachi, Pakistan. Ethical clearance for the study was granted by the Institute’s Ethical Review Committee.
As this was a retrospective audit of all cesarean deliveries over a defined 1-year period, no formal sample size calculation or power analysis was performed.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 14
Inclusion and exclusion criteria
The study included all women who underwent cesarean delivery at Holy Family Hospital, Karachi, between January 1, 2022, and December 31, 2022. Women who had a vaginal delivery, including spontaneous and instrumental births, were excluded from the analysis. Only cases with complete medical records documenting the indication for CS and other relevant obstetric characteristics were included.
Study setting
Holy Family Hospital, Karachi, Pakistan is a tertiary care hospital with an obstetrics and gynecology department with over 1000 normal deliveries per year. Holy Family Hospital is a teaching institute with the obstetrics and gynecology department being recognized as a postgraduate training program by the College of Physicians and Surgeons Pakistan.
Study procedure
During the study period of 1 year, a total of 507 cesarean deliveries were conducted at the Department of Obstetrics and Gynecology, Holy Family Hospital, Karachi, Pakistan. These deliveries were classified into the 10 groups of the Robson classification, as presented in Figure 1. The hospital records of the medical record section were reviewed to extract relevant information for each case. The total number of deliveries was matched with the labor room record. A standardized proforma was designed and utilized to record various details of each CS case, including maternal characteristics (age, parity, mode of previous deliveries, gestational age, number of fetuses, fetal presentation, previous CS and its indications, and onset of labor), fetal outcomes (birth weight, APGAR (Appearance, Pulse, Grimace, Activity, and Respiration) score, and fetal complications), and maternal outcomes (postpartum hemorrhage, anemia, wound infection, need for blood transfusion, ruptured uterus, ICU admission, and maternal mortality). All the data was collected and analyzed by the research team in accordance with the guidelines of the Robson classification system. The study adhered to the principles of data confidentiality and patient privacy.

Robson classification system.
Ethical considerations
Ethical approval for this study was obtained from the Ethical Review Board (ERB) of Holy Family Hospital, under reference number HFH/ERB/2021/OBGYN/112, approved on February 10th, 2023. Patient consent was not required as the study involved retrospective anonymized data. All data were anonymized before analysis, and confidentiality was maintained by restricting access to authorized investigators only and storing data in secure, password-protected databases.
The Robson’s classification
The Robson classification system is a tool that enables the evaluation of the obstetric patient population and the CS rates in a standardized and comparable manner across different settings. This system categorizes all deliveries into 10 mutually exclusive groups based on 5 key obstetric characteristics: parity, onset of labor, gestational age, fetal presentation, and number of fetuses (Figure 1). 15 These groups can be used to identify areas of overuse or underuse of CS and to monitor changes in CS rates over time. In our study, we applied the Robson classification system to the study population of the obstetrics and gynecology department at a tertiary care hospital in Karachi, Pakistan to assess the CS rates and to identify potential areas for improvement in clinical practice.
Development of the audit form
The audit form collected patient’s demographic data and specific indicators relevant to the Robson criteria. To ensure its effectiveness, the form was reviewed by statisticians and experienced obstetricians specializing in clinical audits. To validate the form, a pilot test was conducted involving 30 patients, and the feedback from the stakeholders was used to optimize the audit form.
Statistical analysis
The data from individual cases were entered and organized using Microsoft Excel. Categorical variables were expressed as percentages, and descriptive statistics were used to summarize the demographic and obstetric characteristics of the study population. The analysis was based on the Robson Ten Group Classification System (TGCS), including calculations of group size (percentage of total deliveries), CS rate within each group, relative contribution of each group to the overall CS rate, and absolute group contribution to the total CS rate. Proportions and percentages were used to describe categorical variables. No inferential statistical analyses (e.g., chi-square test and regression analysis) were performed, as the primary objective was to conduct an audit using the Robson classification methodology.
Results
During 1st January 2022 and 31st December 2022, 1464 women met the inclusion criteria and were included in the study (Figure 2). A total of 507 deliveries were included in the study, which was our “population of interest.” A total of 967 were spontaneous vaginal deliveries and were excluded from the study. 67.06% (340) of the patients belonged to the main city, whereas 32.94% (167) belonged to the peripheral areas. This yielded a CS rate of 54.2%. Of the CSs performed, 48.8% (247) were elective and 51.2% (260) were emergency.
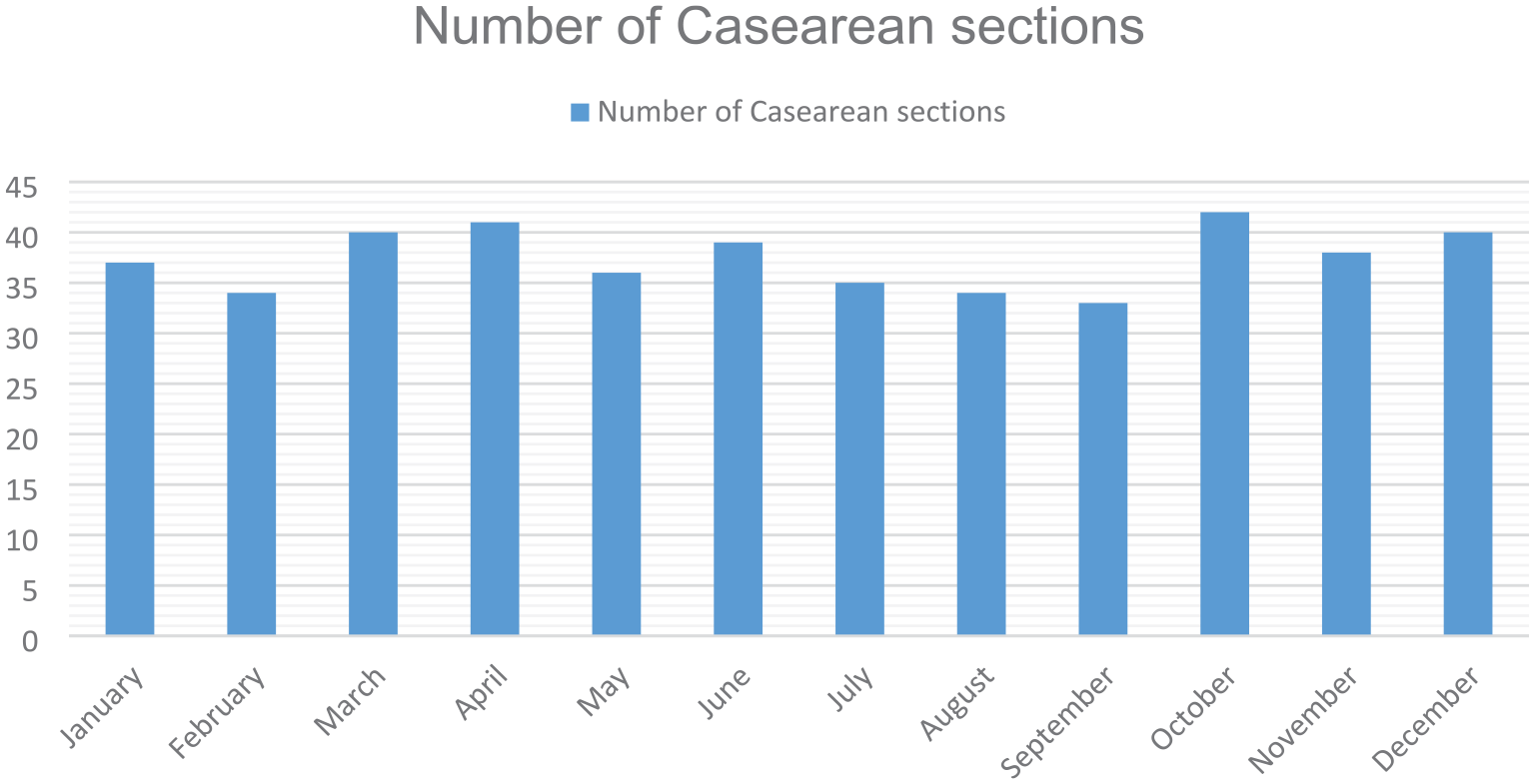
Month-wise distribution of C-sections.
Most of the study participants (323) were in the age group of 21–30 years (63.7%) (Figure 3). Nulliparous women accounted for 37.3% (188) of the study population, while multiparous women accounted for 62.7%. Women with a history of previous CS constituted 64.09% (323) of the study participants. The majority of the CS (99%) were performed at term between 37 and 40 weeks of gestation.

Age-wise distribution of CS.
The Robson classification (Table 1) showed that group 5 (previous CS, singleton, cephalic, and ⩾37 weeks’ gestation) was the highest contributor to the overall CS rate, contributing 51.9% of all CS and 27.5% in ratio to all deliveries at the hospital. Group 2 (Nulliparous, single cephalic, ⩾ 37 weeks, induced or CS before labor) was the second highest contributor, contributing 18.5% to the overall CS and 9.82% in ratio to all deliveries at the hospital. The third highest contributors were group 10 (All singleton, cephalic, < 37 weeks’ gestation pregnancies (including previous CS)) contributing 14.4% to the overall CS rate and 7.63% in ratio to all deliveries at the hospital. The least contributor to the overall CS rate was group 9 (All women with a single pregnancy in a transverse or oblique lie (including those with previous CS)), contributing 0.39% of all CS and 0.21% in ratio to all deliveries at the hospital. The remaining groups (groups 1, 3, 4, 6, 7, and 8) contributed 15.2% of all CS and 9.05% in ratio to all deliveries at the hospital.
Distribution of CS by different subgroups of TGCS.

CS, cesarean section; TGCS, Ten Group Classification System.
The main indications for CS in the 260 patients who underwent emergency CSs were previous history of cesarean section (32.3%), non-progress of labor (21.15%), cephalopelvic disproportion (16.92%), fetal distress (8.46%), breech presentation (6.54%), pre-eclampsia (6.15%), refusal for vaginal birth after cesarean (VBAC; 5.00%), low-lying placenta (3.09), and transverse lie (0.39%).
Discussion
The present audit report assessed the CS rates using the Robson classification at a tertiary care hospital’s obstetrics and gynecology department in Karachi, Pakistan. Robson’s classification, designed in 2001, is often referred to as the “Ten Group Classification System (TGCS),” as it divides CSs into 10 groups based on the gestational age of the pregnancy, several pregnancy-related characteristics (parity, position, presentation, etc.), prior obstetrical history, and labor and delivery procedures and allows identification of the groups that contributed the most to the overall CS. 13 It was officially endorsed by WHO in 2015 as the gold standard to monitor CSs. 16
Analyzing the CS rate is crucial in determining the quality of maternal healthcare and ensuring the safety of both the mother and the child during childbirth. A high CS rate may suggest overuse of the technique, which might put the mother and infant in needless danger and complicate matters. 17 On the other hand, low CS rates may imply underuse of the operation, which, particularly in some patient populations, may lead to avoidable maternal and newborn morbidity and death. 18 Therefore, analyzing the CS rate is an essential tool for evaluating the effectiveness and efficiency of maternal healthcare systems, identifying areas for improvement, and ensuring that women receive appropriate and timely care during childbirth. The objective of this study is to determine the CS rate investigate the factors contributing to it in tertiary care hospitals and compare it with hospitals in similar settings, with the aim of identifying strategies to improve the quality and safety of maternal healthcare.
The findings indicate a CS rate of 54.2%, which is higher than the WHO’s recommended rate of 10%–15%. 1 Several institutional and regional factors may have contributed to this elevated rate. As a tertiary care referral center, our hospital frequently receives high-risk obstetric cases from peripheral facilities, which likely skews the case mix toward more complex deliveries requiring CS. 19 Additionally, a substantial proportion of women presenting had a history of previous CS, reducing eligibility for the trial of labor. 20 Clinical practices such as lower thresholds for elective CSs in cases of suspected cephalopelvic disproportion, non-progress of labor, and fetal distress—often based on subjective clinical judgment—also contribute. 21 Furthermore, medicolegal concerns, limited VBAC protocols, lack of midwifery-led care models, and insufficient labor monitoring infrastructure may further encourage clinicians to opt for cesarean delivery. These findings align with patterns observed in other tertiary care centers, as highlighted in recent literature.2,22,23 Therefore, contextual factors must be considered when interpreting CS rates in high-volume referral hospitals. 8 It is essential that local strategies be designed keeping in view these institutional realities to promote rational CS use without compromising maternal or neonatal outcomes.
Robson group 5 (previous CS, singleton, cephalic, ⩾37 weeks) contributed the largest proportion to the overall CS rate in our study. This trend is consistent with several national and international audits where repeat cesarean is a major contributor to rising CS rates.8,22,23 Majority of the sections happened due to the history of previous cesarean sections, which was similar to other studies.22 –24 A commonality in all these studies including ours22 –24 was the low rate or absence of CS due to refusal for VBAC, this indicates that the doctors in developing regions are not promoting the use of VBAC. There is a need to investigate the causes of doctors not offering VBAC options to patients but possible reasons might include the recent literature showing decreased success rates of VBAC, 25 concerns about uterine rupture, lack of emergency response protocols, absence of clear institutional guidelines, and increased risk of legal proceedings over failure of VBAC. 26 To improve VBAC rates, hospitals should implement standardized antenatal counseling checklists, develop VBAC eligibility criteria, and ensure round-the-clock access to emergency obstetric care. Previous history of CS being the major indication for CS highlights the importance of promoting VBAC in eligible women to reduce the rate of repeat CS. The American College of Obstetricians and Gynecologists recommends VBAC as a safe and appropriate option for most women with a previous CS. 27
The second highest contributor was group 2, which consisted of nulliparous, single cephalic, ⩾ 37 weeks who were either induced or had CS before labor. This finding is consistent with the findings by Ansari et al. at a tertiary care hospital in Pakistan, 24 but the other studies didn’t have group 2 as a major contributor.22,23 This is troubling since nulliparous women having a high likelihood of CS can result in needless risks such as greater maternal morbidity and death, lengthier hospital stays, and higher healthcare expenses. 28 Therefore, it is crucial to implement policies to reduce the rate of CS in this group.
The percentage of elective CSs was very high, this indicates either the community is ill-informed about CSs and their implications or that they are not being counseled well by the admitting doctors. Hence, there is a need to conduct an awareness campaign about the benefits and pitfalls of CSs. The junior doctors should be trained to conduct the counseling of the expecting mothers and be well-versed in indications for CSs.
In addition to clinical and institutional factors, medicolegal concerns have increasingly influenced the decision to perform CSs. In many settings, obstetricians may opt for CS over vaginal delivery to minimize the risk of litigation in the event of adverse maternal or neonatal outcomes. This defensive medical practice, while intended to safeguard practitioners, can inadvertently contribute to unnecessary cesarean procedures, further driving up the overall CS rate.
The findings of this study suggest that there is a need for strategies to optimize the use of CS and reduce the overall CS rate in the hospital’s obstetrics and gynecology department. To address rising CS rates, a multifaceted approach is essential. Strategies include promoting evidence-based labor management protocols, enhancing patient education and informed decision-making, encouraging VBAC where appropriate, implementing audit and feedback mechanisms such as Robson classification monitoring, and improving clinical confidence in managing vaginal deliveries. In addition, institutional support and medicolegal reform can help alleviate defensive obstetric practices.
Strategies for improving labor management include the appropriate use of induction of labor and fetal monitoring, to reduce the rate of non-progress of labor and fetal distress, which were among the top indications for CS in this study. In addition, increasing access to VBAC and implementing VBAC-friendly policies may help to reduce the rate of repeat CS. These strategies should be implemented with caution and should take into account the individual needs and preferences of women and their families.
The study has multiple limitations, the study utilized a standardized protocol for data collection and a validated classification system (the Robson classification) to evaluate the CS rates in a comparable manner across different settings and had a large sample size of 507 cesarean deliveries in 1 year, which provides a good representation of the population in the study setting. However, this study was conducted in only one hospital in Karachi, Pakistan, which limits the generalizability of the findings to other settings. The study did not include vaginal deliveries in the analysis, which may have provided a more comprehensive picture of the overall obstetric population. The study was retrospective in nature, which may lead to incomplete or missing data, which limits the ability to control for confounding variables. The study did not record information about the reasons for the high CS rates individually in each Robson group, which limits the ability to identify specific areas for improvement in clinical practice. The study did not collect information on some potentially important variables, such as BMI, and fetal weight, which may have influenced the CS rate. Additionally, since no formal sample size calculation was conducted, the findings are descriptive in nature and may not be generalizable beyond the study population.
In the future, we will be designing strategies based on the above-given results, and post-implementation we will repeat this audit to look at the results after the implementation, which will indicate the success of the interventions and give directions for future interventions.
Conclusion
The analysis of the CS rate revealed that the CS rate was more than threefold higher than the recommended threshold set by the WHO. The primary indication for CS was the previous history of CS. Our audit highlights the need for targeted, evidence-based strategies to address the rising CS rates, particularly among repeat cesarean deliveries. Actionable measures such as promoting VBAC, strengthening antenatal counseling protocols, implementing standardized labor management guidelines, and regular clinical audits based on the Robson classification system can contribute significantly to reducing unnecessary CS while ensuring maternal and neonatal safety. Further research and policy-level interventions are warranted to optimize obstetric care and balance the risks and benefits of cesarean delivery in resource-limited settings. The implementation of these strategies may lead to improved maternal and fetal outcomes, reduced healthcare costs, and increased patient satisfaction.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251339710 – Supplemental material for Application of the Robson classification in assessing cesarean section rates: an audit of a tertiary care hospital’s gynecology department in Karachi, Pakistan
Supplemental material, sj-docx-1-reh-10.1177_26334941251339710 for Application of the Robson classification in assessing cesarean section rates: an audit of a tertiary care hospital’s gynecology department in Karachi, Pakistan by Syed Muhammad Aqeel Abidi, Syeda Namayah Fatima Hussain, Shahida Abbas, Syeda Tayyaba Fatima Abidi and Sonia Haresh in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
None.
Author’s note
A preprint version of this manuscript was previously published on medRxiv, available at: ![]() . The authors declare that data supporting the findings of this study are available within the article. The article is the author(s) original work. The article has not received prior publication and is not under consideration for publication elsewhere. All the authors have seen and approved the manuscript being submitted. The author(s) abide by the copyright terms and conditions of publishing the journal.
. The authors declare that data supporting the findings of this study are available within the article. The article is the author(s) original work. The article has not received prior publication and is not under consideration for publication elsewhere. All the authors have seen and approved the manuscript being submitted. The author(s) abide by the copyright terms and conditions of publishing the journal.
Disclaimer
The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of any organization or institution with which they may be affiliated. The information presented in this paper is intended for academic and research purposes only and should not be construed as professional advice or recommendations.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.