
Abstract
Background:
In 2020 in sub-Saharan Africa, 25% of new human immunodeficiency virus (HIV) infections occurred among young women (15–24 years). In Uganda, the HIV prevalence is three times higher among young women at 2.9% compared to 0.8% among their male counterparts. HIV status disclosure is a gateway to preventive services.
Objectives:
We set out to estimate the prevalence of HIV status disclosure to current male partners, and the predictors among the adolescent girls and young women living with HIV (AGYWLHIV) in a semi-rural northern Uganda.
Design:
In a cross-sectional study design, a consecutive sample of the AGYWLHIV was recruited from six antiretroviral therapy clinics between November 2022 and April 2023.
Methods:
Participants were administered an interviewer-guided questionnaire. They were asked whether they have ever disclosed their HIV status to their current male partners. They were also asked about their socio-demographics, sexual and reproductive health profiles, knowledge and perceptions of dual protection, and safer conception methods for AGYWLHIV. Percentages to estimate prevalence, Chi-square tests to assess associations, simple and multivariate modified Poisson regression to identify predictors at p < 0.05 and 95% confidence intervals (CI) were considered.
Results:
Overall, 423 participants with a median age of 22 (IQR 4) years participated in the study. The prevalence of HIV status disclosure to the current male partners was found at 73.3% (95% CI 69.0–77.5). The predictors for HIV status disclosure were found to include the women’s knowledge of their HIV status (APR 1.1 (95% CI 1.0–1.2), p 0.032), knowledge of their male partner’s HIV status (APR 0.8 (95% CI 0.7–0.9), p 0.003), and the male partners’ disclosure of their HIV status to the women (APR 0.7 (95% CI 0.5–0.9), p <0.016).
Conclusion:
About three-fourths of the AGYWLHIV in semi-rural northern Uganda disclosed their HIV status to their male partners. The predictors of disclosure included the women’s knowledge of their HIV status, knowledge of their male partner’s HIV status, and the male partner’s reciprocal disclosure of their HIV status. To enhance disclosure rates, post-test, and disclosure counseling for both individuals and couples is recommended as part of the routine HIV testing, treatment, and care programs.
Plain language summary
The world is still experiencing many new HIV infections among young women including adolescent girls. Adolescent girls and young women are more affected than boys and men. Women and girls can get to know of their HIV status because of the HIV counseling and testing during preconception, antenatal, and postnatal care aimed at preventing the transmission of the infection to their babies. Beside that, it is important that women who know their status disclose their HIV status to their male sexual partners so that both partners can seek medical treatments for prevention of the transmission if one partner remained uninfected or for treatment of both partners if both of them are infected. This research estimated the proportion of adolescent girls and young women living with HIV who have disclosed their HIV status to their current male sexual partners and the factors that influence disclosure. To answer the above objectives, we asked 423 adolescent girls and young women living with HIV in rural Uganda whether they disclosed their HIV status to their current male sexual partners. We also collected information about the women’s sociodemographic characteristics, sexual and reproduction related perceptions and behaviors. The research findings reveal that 73.3% of the adolescent girls and young women disclosed their HIV status to their current male sexual partners. The factors that were found to have influenced disclosure were the women’s knowledge of their HIV status, the male partners disclosing their HIV status to the women, the women’s age at initiation of sexual activity and the women’s years of experience in sex. In conclusion, this research conducted in rural Uganda found that not all sexually active young women living with HIV disclose their HIV status to their male sexual partners. Disclose is influenced by the woman’s knowledge of her HIV status, reciprocal disclosure by the male sexual partner, the woman’s age at inititiation of sexual activity and her years of experience in sexual matters. The research calls for couple testing and disclosure counseling.
Introduction
The high human immunodeficiency virus (HIV) burden among young women in sub-Saharan Africa (SSA) is a significant concern. Despite representing only 10% of the population in SSA, adolescent girls and young women aged 15–24 years (AGYW) accounted for 25% of new HIV infections in 2020. 1
Moreover, in SSA, many sexually active adolescent girls and young women living with HIV (AGYWLHIV) do not disclose their HIV status to their partners (76%–100%) or fail to use protection (35%–55%), primarily due to fear of stigma and discrimination.2,3 Previous studies conducted among women living with HIV (WLHIV) in Canada and East Africa found that WLHIV feared disclosing their HIV status to their male sexual partners to avoid the existing gendered power imbalances in sexual relationships such as violence, and rejection or abandonment.3 –5 Other antecedents to women’s nondisclosure of their HIV status to their male sexual partners include women’s low educational attainment, poverty, and fear of being blamed for unfaithfulness which are culturally constructed injustices against women in many SSA settings5,6
The high risk for sexual transmission of HIV among discordant couples involving AGYWLHIV is an obvious consequence of nondisclosure of HIV status, with studies reporting transmission rates ranging from 0.0007 to 0.0082 per coital act.7,8 The risk for sexual transmission of HIV remains in discordant partnerships even when the HIV-infected partner is on antiretroviral therapy (ART), thus undermining the “Undetectable = Untransmissible” (U = U) principle in situations of late ART initiation and inconsistent adherence and all of which are influenced, in part, by mutual disclosure within the partnership.9,10 Other potential consequences of HIV status non-disclosure would be delayed entry into the HIV testing, treatment, and care for the sexual partners and missed opportunities for partner support to the partner living with HIV. 5
While people living with HIV have the right to keep their status private, disclosing HIV status within the context of sexual and reproductive health is crucial for adopting preventive measures against HIV and other sexually transmitted infection’s transmissions and unintended pregnancies. It contributes to the broader goal of preventing new infections and controlling the spread of the virus. This is important because when couples become aware of their respective HIV statuses, they are more likely to adopt consistent condom use and engage in safer sexual practices, 11 utilize pre-exposure prophylaxis (PrEP), 12 adopt post-exposure prophylaxis (PEP),13 –15 use dual protection methods, 16 and consider safer conception methods, 17 thereby reducing the risk of transmission within their relationships and beyond.
To improve HIV disclosure rates to male sexual partners, the World Health Organization (WHO) recommended several programs and policies for WLHIV. First is to link voluntary HIV counseling and testing (VCT) programs to intimate partner violence (IPV) care programs so that women who report barriers to HIV disclosure such as fear of IPV at VCT programs would be referred to IPV care programs in their communities. The second is to conduct cross-training of HIV and domestic violence staff. 18 Cross-training entails providing VCT staff with information on domestic violence so that they acquire the knowledge to identify and refer women who are at risk of IPV, thereby improving the chances of HIV status disclosure. 18 Third is to improve the HIV disclosure skills and self-efficacy among the WLHIV through practical counseling approaches such as role play, scenarios, and other behavioral rehearsal techniques. 18 Fourth is to develop support groups for WLHIV to provide ongoing support during their HIV disclosure process. 18 The fifth WHO programmatic and policy recommendation is to make use of mediators (the HIV counselor, health workers, trusted family members, or friends) to moderate or facilitate the HIV disclosure processes at the health facility or the couple’s homes. 18 The sixth is to encourage couple counseling and testing for HIV instead of testing people in silos and this is thought to help in bypassing the barriers to HIV disclosure. The seventh programmatic and policy recommendation is to develop or link WLHIV to women empowerment programs that address women’s unfavorable gender norms and facilitate HIV disclosure to sexual partners. 18 The eighth programmatic and policy recommendation is to develop or link WLHIV to community-based programs for addressing HIV stigma and discrimination to encourage HIV disclosure. 18 The ninth programmatic and policy recommendation is to develop or link WLHIV to community-based programs that improve communication between partners or couples as they can lead to HIV status disclosure and better outcomes for WLHIV. 18 These WHO programmatic and policy recommendations for improving women’s disclosure of their HIV status to sexual partners have been adapted by many developing countries including Uganda since 2004 and their implementation has been linked to the routine VCT, ART, and adherence counseling programs for persons living with HIV (PLHIV).
Despite the above WHO programmatic and policy recommendations to improve disclosure rates among WLHIV, the prevalence of HIV status disclosure to male sexual partners has remained suboptimal among women in the developing world (average 52%; range: 16%–86%) compared to the developed world (average 71%; range: 42%–100%). 5 Among the studies in the developing countries that reported the prevalence of HIV status disclosure to current or steady male sexual partners, the average prevalence of disclosure was 49%, considerably less than the average prevalence reported from studies conducted in the developed world (79%). 5 Previous studies in Kampala and the regions of central and southwestern Uganda reported the prevalence of HIV status disclosure as ranging from 34.6% to 73.1% among AGYWLHIV attending ART clinics.19 –21 Previous studies in other SSA settings such as Ethiopia and Nigeria that investigated mixed-age and mixed-gender populations of PLHIV attending non-maternal healthcare programs reported the prevalence of HIV status disclosure among women as ranging from 54.7% to 89.3%.22 –24 Studies in other SSA settings such as Togo reported the prevalence of HIV status disclosure among mixed-age and mixed-gender populations of PLHIV attending non-maternal healthcare programs as ranging from 21% to 60.9%, but these studies did not disaggregate the disclosure rates by gender or age groups.25 –28
Previous studies identified some of the predictors for HIV status disclosure among young women but were not explicit on how sexual and reproductive health aptitudes and desires influence disclosure. To exemplify, a systematic review and meta-analysis for the prevalence and predictors for HIV serostatus disclosure among HIV-positive women in the East African region found that WLHIV who knew their partner’s serostatus, and held prior discussions about HIV testing with their male sexual partners were more likely to disclose their HIV serostatus to their male sexual partners compared to their counterparts who did not know their partner HIV status and did not hold prior discussions about HIV testing with their male sexual partners, respectively. 29 Similarly, previous antenatal clinic-based cross-sectional studies conducted among pregnant women in Ethiopia and Uganda receiving prevention of mother-to-child transmission (PMTCT) of HIV services found that pregnant women who had smooth sexual relationships, had planned their pregnancy, had sufficient knowledge of HIV prevention methods, and had ever practiced safer sex methods were more likely to disclose their HIV status to their male sexual partners compared to their counterparts who had violent sexual relationships, did not plan their pregnancies, had insufficient knowledge about HIV prevention methods, and did not practice safer sex methods, respectively.30 –32 Lastly, several ART clinic-based cross-sectional studies conducted among mixed-gender and mixed-age people receiving ART in East and West African countries found that people living with HIV who were members of anti-HIV support groups or clubs, and had no fears of social violence were more likely to disclose their HIV status to their sexual partners compared to their counterparts who were not members of anti-HIV support groups or clubs and were fearful of social violence, respectively.25 –28
The previous studies on the prevalence of HIV status disclosure and the predictors among AGYWLHIV in developing countries, particularly in SSA including Uganda, expose several noteworthy gaps that call for deeper exploration. Primarily, there is a conspicuous absence of studies that thoroughly investigated the intricate sexual and reproductive aptitudes associated with HIV status disclosure among the AGYWLHIV. This gap calls for further research tailored to the sexual and reproductive aptitudes and desires of AGYWLHIV, and how they influence their HIV status disclosure to their male sexual partners.
Furthermore, in SSA, the responsibility for initiating HIV status disclosure tends to fall on the women, even those who are younger, are new to sexual relationships, and are in less empowered positions. This tendency arises from the HIV prevention services that primarily target women and focus on PMTCT through interventions like dual protection for child spacing, safer conception, HIV testing and ART in pregnancy during antenatal care, postnatal care, and exclusive breastfeeding. These services position women to receive more information, education, and HIV prevention resources than men, who have fewer targeted HIV health services. Further research is therefore needed about HIV status disclosure in the context of the partner’s sexual reproduction desires to support the use of safer conception and dual protection methods, aiming to prevent HIV transmission to both the sexual partners and future children.
Specific objectives
We set out to determine the prevalence of HIV status disclosure and its sexual and reproductive predictors among AGYWLHIV in semi-rural northern Uganda. The potential predictors of focus were the AGYWLHIV’s sexual and reproductive desires, sexual feelings, knowledge of their initial HIV status and that of their male sexual partners, and their knowledge, perceptions, and use of the dual protection and safer conception methods.
Conceptual framework
There was no specific theoretical framework or model that was used to guide the study. Therefore, a conceptual framework was developed specifically for the study using the previous literature.19 –32 In the conceptual framework, we framed the construct of HIV status disclosure as a social and preventive health behavior. As a social and preventive health behavior, the HIV-infected partner’s decision to disclose or not to disclose status would be an intricate balance of two tenets namely knowledge of and perceptions about the existing measures to maintain safer sexual life and reproductive health in the sexual partnerships. Specifically, disclosure is likely to be influenced by the woman’s knowledge of, and perceived benefits of the dual protection and safer conception methods. More so, disclosure may be influenced by the perceptions around the advantages, barriers, or challenges of the dual protection and safer conception methods.
The woman’s socio-demographic characteristics are also influential as they shape her social environment including exposure to and perceptions about the dual protection and safer conception methods, and hence her readiness to share her status. Sexual and reproductive health characteristics, like her age at sexual debut, years of sexual experiences, desire for children, and previous pregnancies or childbirths, also may influence her exposure to and perceptions about the dual protection and safer conception methods and ultimately her likelihood of disclosure.
This framework highlights the need for investigations into the complex interplay of personal, social, and sexual reproductive health-related factors that may influence women’s decision to disclose their HIV status to their male partners.
Methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies. 33 The checklist is followed from the study title and abstract through discussion and other information such as funding.
Study design
The study was a cross-sectional study. 34 Its primary focus was the quantitative estimation of the prevalence of HIV status disclosure (the outcome variable) and the sexual and reproductive health-related predictors (the exposure variables) among the AGYWLHIV in semi-rural Uganda.
Study area and setting
The study was conducted in Lira district and Lira city. It is located in northern Uganda. It is about 340 km from Kampala, the capital city of Uganda. By 2020, the HIV prevalence among people aged 15–49 in the area had reached 7.2%, and this surpassed the national average of 5.4%. 35 The participants were recruited from the ART clinics of six public health facilities within the study area, namely Lira Regional Referral Hospital, Lira University Hospital, Ober Health Center, Ogur Health Center, Amuca Health Center, and Barapwo Health Center. The ART clinics collectively served 1,771 AGYWLHIV aged 15–24 as of September 2022.
Study population
The study population comprised AGYWLHIV aged 15–24. These were attending the ART clinics at public health facilities. The area had an estimated 28,000 PLHIV aged 15 and older. 36 This accounted for about 2% of the 1,400,000 PLHIV in Uganda. 35
Inclusion criteria
An AGYWLHIV aged 15–24 was considered for inclusion in the study if she (a) had lived with HIV for one or more years, (b) reported ever being sexually active (i.e., having had sexual intercourse at least one time within the past 2 years), and (c) was a resident of Lira district or Lira city.
Exclusion criteria
The sexually active AGYWLHIV aged 15–24 years were excluded from the study if they were deaf or mute, and therefore could not communicate in the interviews and or if they were visibly too sick to withstand the study procedures.
Sampling methods and participant recruitment
The study employed a stratified random sampling method. 37 Initially, a comprehensive list of the AGYWLHIV was established from the ART clinic registers. This list was stratified by the three levels of public health facility namely regional referral hospital patients, health center level IV patients, and health center level III patients. Lastly, proportionate to size sampling comprising 182, 126, and 115 participants were recruited from the three strata, respectively (see Table 1).
Socio-demographic characteristics of the study participants.

AGYWLHIV, adolescent girls and young women living with HIV; f, frequency; IQR, interquartile range; km, kilometers; USD, United States Dollars.
Data collection tool
The data collection tool was the questionnaire (Supplemental Appendix 1). It was specifically developed using the existing literature.19 –32 The questionnaire measured the exposure and the outcome variables.
The questionnaire was pre-tested on 10 young women from Lira University Hospital. Adjustments were made to the questionnaire items whose responses yielded limited or no variability.
The questionnaire items pulled from the previous literature19 –32 included the participant’s socio-demographic characteristics namely the participant’s age, marital status, educational level, place of residence, religious affiliation, employment or occupation, monthly income, level of health facility for ART attendance, alcohol use, smoking status, parity, number of children, whether the woman has ever gotten pregnant in the past 1 year, woman’s prior knowledge of her own and partner’s initial HIV status before engaging in sexual relationships.6,38 Additional items pulled from the previous literature19 –32 included the woman’s years of living with HIV, knowledge of her initial HIV status and that of her current male sexual partner before their first sexual intercourse, whether the woman desires to bear children or get pregnant, and whether the woman fears HIV stigma, discrimination, or IPV. 39
The questionnaire items the investigators developed specifically for this study included the woman’s knowledge of the male partner’s desire to bear children and his desired number of children, the woman’s knowledge, perceptions, and ever use of the dual protection methods, the woman’s knowledge and perceptions of safer conception methods for WLHIV. After pretesting, the items adjusted were the woman’s number of male sexual partners and whether the woman fears HIV stigma, discrimination, IPV or relationship breakup upon disclosure of her HIV status to her male sexual partner.
The participants aged 15–17 years (legally minors) were equally asked whether they desired to bear children just like the adult participants (aged 18–24 years). This was because the investigators thought that the desire to bear children would negatively influence the woman’s likelihood of disclosing her HIV-positive status to the male partners and vice versa in order not to scare away the male partner from their ongoing sexual relationships. In the context of developing countries including Uganda, younger WLHIV including teenage girls suffer many socio-economic consequences of HIV infection including school dropout, abandonment, and early marriages, and often aspire for pregnancy conceptions and childbirths as a way of securing the social and economic support from their male partners.
Data collection procedures
Data were collected between the 20th of November 2022 and the 30th of April 2023. Data were collected by six female Research Assistants with health backgrounds, one each per ART clinic. The local language (Langi) was used to collect the data. Questionnaires were administered by face-to-face interview. It took about 1 h to complete each questionnaire. The participant’s responses (data) were recorded directly on the questionnaire in ink.
Outcome variables
The primary outcome was the woman’s disclosure of her HIV status to the current male sexual partners. The secondary outcomes included (a) one-way disclosure of the HIV status of the current male sexual partner to the woman, (b) one-way nondisclosure of the HIV status of the woman to the current male sexual partner, (c) two-way disclosure of the HIV status of both partners, and (d) two-way nondisclosure of the HIV status of both partners. HIV status disclosure was regarded as the social and preventive health behavioral outcome of interest.
Measures of the outcome variables
To measure the woman’s one-way disclosure of her HIV status to her current male sexual partners, she was asked whether her HIV status was disclosed to her current male sexual partners and the response options were yes (coded as 1) or no (coded as 0). She was also asked whether the current male sexual partner’s HIV status was disclosed to her. The response options for this were similarly yes (coded as 1) or no (coded as 0). The above two items enabled the measurement of the prevalence of one-way disclosure, one-way nondisclosure, two-way disclosure, and two-way nondisclosure among the participants.
If one of the partner’s HIV statuses was disclosed or undisclosed but not both, this was regarded as one-way disclosure or one-way nondisclosure. If both partners disclosed their HIV status to each other, this was regarded as a two-way disclosure. If neither of the partner’s HIV status was disclosed to the other, this was regarded as a two-way nondisclosure.
The items to measure the above outcome variables are described in detail in the Supplemental Material (Appendix I which was the Questionnaire). The study adapted some of the above measures for HIV status disclosure, and nondisclosure from a previous study conducted in Uganda. 40
Exposure factors and covariates
The exposure factors and covariates for the study were (a) the woman’s age at sexual debut, (b) the woman’s years of sexual experience, (c) the woman’s sexual activity level, (d) the woman’s knowledge of her HIV status before meeting the current male partners, (e) the period of the woman’s knowledge of her HIV status, (f) the woman’s desire to bear children, (g) the male partner’s desire to bear children, (h) the male partner’s disclosure of his HIV status to the woman and hence the woman’s knowledge of the HIV status of her male partner, (i) the woman’s perceptions of the benefits of the dual protection methods, (j) the woman’s knowledge of safer conception methods, (k) the woman’s perceptions of the benefits of the safer conception methods, and (l) the woman’s socio-demographic characteristics, particularly her age, religion, marital status, rural or urban residential address, distance from the nearest health facility, educational level, employment status or occupation, and her monthly income level.
The selection of the above exposure factors and the covariates particularly the sexual and reproductive health-related ones were informed by their plausible relationships to the HIV status disclosure behavior as they received limited consideration in the previous studies on HIV status disclosure among AGYWLHIV.5,17,19 –32 The specific measures for the exposure factors and the covariates in the questionnaire are presented along with the results in Tables 1–3. They are also presented in detail in the Supplemental Material (Appendix I which is the questionnaire). The study adapted some of the measures for the exposure factors and the covariates described in the questionnaire from a previous study conducted in Uganda. 40
The sexual and reproductive characteristics of the study participants.

AGYWLHIV, adolescent girls and young women living with HIV; f, frequency; IQR, the interquartile range; km, kilometers; ART, antiretroviral therapy; ARV, antiretroviral drug; PrEP, pre-exposure prophylaxis; PEP, post-exposure prophylaxis; AI, artificial insemination; IVF, invitro fertilization.
Associations between the socio-demographic, sexual, and reproductive factors and disclosure of HIV status to current male sexual partners.

AGYWLHIV, adolescent girls and young women living with HIV; F, frequency count; %, percentage; ARV, antiretroviral drugs; PrEP, pre-exposure prophylaxis with antiretroviral drugs; PEP, post-exposure prophylaxis with antiretroviral drugs; ART, antiretroviral therapy with antiretroviral drugs; X2, Chi-square value; df, degree of freedom; Na, not applicable; AI, artificial insemination; IVF, invitro fertilization.
Bold values indicate statistical significance at p < 0.05.
Sample size determination
The sample size for the study was calculated using the Kish Leslie (1965) formula. 41 The calculation assumed the Z score at a 95% confidence interval of 1.96, the prevalence of HIV disclosure of 0.731 based on a similar previous study conducted in central Uganda, 19 and the precision of 0.05. This produced an unadjusted sample size of 303 participants. After 1.5 adjustments for design effect, the final sample size was 454 AGYWLHIV.
Data management
The data from the completed questionnaire were double-entered by two data clerks using EpiData Entry, Version 3.1, EpiData, Odense, Denmark. Generally, there was no missing at random data because the interviewers ensured all the applicable questionnaire items were responded to by all the participants. For not missing at random items arising from questionnaire items that were not applicable to some of the participants, they were uniquely coded and excluded from the specific analysis on an item-by-item basis. The double-entry validated dataset was exported from the EpiData to the IBM Statistical Package for Social Sciences (SPSS) Statistics for Windows version 29.0 Armonk, NY: IBM Corp., for statistical analysis.
Statistical analysis
The categorization of each variable is shown in Tables 1 to 4. The participants’ socio-demographic characteristics were summarized into frequency counts and percentages. Point estimates such as median and interquartile range (IQR) were calculated using descriptive statistics. The prevalence of HIV status disclosure was calculated from the univariate analysis (frequency counts and percentages). Bivariate analysis (Chi-square statistics) followed by the bivariate and multivariate modified Poisson regression analyses were performed to identify independent predictors for a woman’s HIV status disclosure. Statistical significance at <0.05 and a 95% confidence interval were considered for all statistical tests.
Predictors of HIV status disclosure to the current male sexual partners.
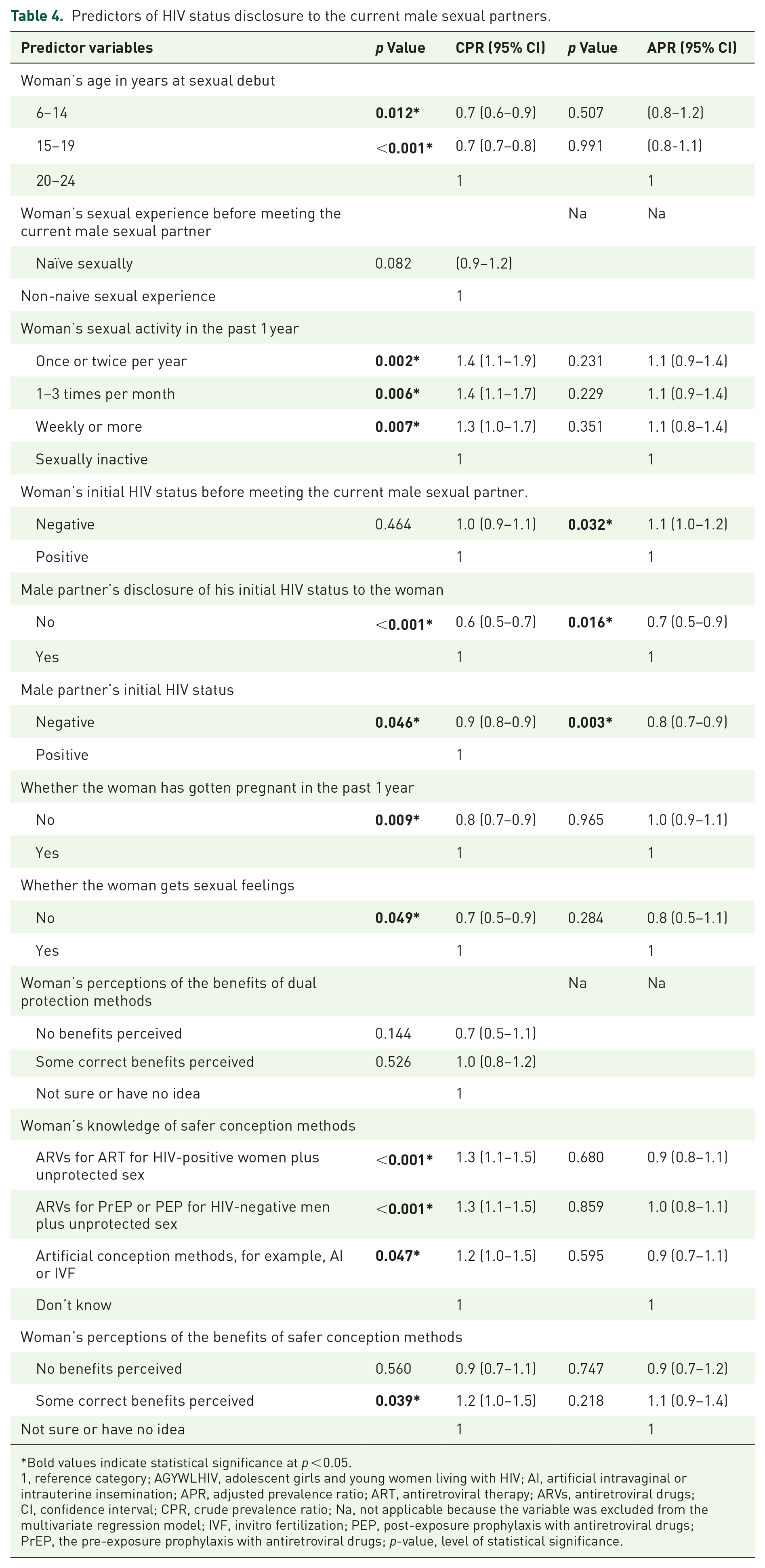
Bold values indicate statistical significance at p < 0.05.
1, reference category; AGYWLHIV, adolescent girls and young women living with HIV; AI, artificial intravaginal or intrauterine insemination; APR, adjusted prevalence ratio; ART, antiretroviral therapy; ARVs, antiretroviral drugs; CI, confidence interval; CPR, crude prevalence ratio; Na, not applicable because the variable was excluded from the multivariate regression model; IVF, invitro fertilization; PEP, post-exposure prophylaxis with antiretroviral drugs; PrEP, the pre-exposure prophylaxis with antiretroviral drugs; p-value, level of statistical significance.
Multi-collinearity analyses among exposure factors and the covariates that were associated with the women’s HIV status disclosure from the bivariate analysis were conducted and no multi-collinearity was found.
The potential predictors were selected for regression analysis based on their plausibility, more so their statistically significant associations with the outcome variable from the bivariate analysis. Eight potential predictors were entered into the bivariate and multivariate modified Poisson regression analyses. These included the woman’s age at sexual debut, the woman’s sexual activity level, the woman’s knowledge of her initial HIV status, the male partner’s disclosure and hence the woman’s knowledge of his initial HIV status, the male partner’s initial HIV status, whether the woman has gotten pregnant in the past 1 year, whether the woman gets sexual feelings, the woman’s knowledge of the safer conception methods, and the woman’s perceptions of the safer conception methods.
Two variables were excluded from the multivariate modified Poisson regression model. They included the woman’s sexual experience before meeting the current male partner and the woman’s perceptions of the benefits of the dual protection methods. These two factors were excluded from the multivariate regression analysis because of their insignificant associations with the women’s HIV status disclosure from the bivariate analysis.
The modified Poisson regression analyses were ran at both bivariate and multivariate levels. For each analysis, models were built for estimating the main effect. The parameter estimation method of choice was hybrid with a robust variance estimator. The convergence criteria were specified as absolute change in parameter estimates with a minimum of 0.0001. The modified Poisson regression was also used in a previous study in Uganda for identifying factors associated with outcomes with high prevalence such as pregnancy termination among women of reproductive age. 42
Results
Response rate
A total of 423 AGYWLHIV out of the targeted 454 sample size were successfully recruited and participated in the study, giving an overall response rate of 93.2%. Thirty-one potential participants (6.8%) were invited but declined to participate in the study mainly because of their poor health status at the time of the study which could not allow them to withstand the study procedures. There were no statistically significant differences in the socio-demographic characteristics of the AGYWLHIV who participated in the study and those who declined to participate in the study.
Socio-demographic characteristics of the study participants
The age of the participants ranges from 15 to 24 years with a median age of 22.0 (IQR 4.0) years. The socio-demographic characteristics of the participants are shown in Table 1. Most of the participants were adults aged 19–24 who were married (living with the current male partners), had attained a primary level of education, were low-income earners relying on domestic remittances, and resided within a 5-km radius of a public health facility.
Sexual and reproductive characteristics of the study participants
The sexual and reproductive characteristics of the participants are shown in Table 2. The findings indicate that all the participants were in active sexual relationships with a recent sexual activity reported within 8.0 ± 15.7 days. The participants started sexual activity with their current male partners within 2.4 ± 2.4 years at an age of 19.0 ± 2.6 years, and 91.7% of them were unaware of their initial HIV status at the onset of the sexual relationships with the current male partners.
Prevalence of HIV status disclosure
The overall prevalence of disclosure of HIV status of the young women to their current male partners was found at 73.3% (95% CI: 69.0–77.5). Figure 1 shows the prevalence of the various forms of HIV status disclosure among the young women and their current male partners. The prevalence of one-way disclosure of the HIV status of young women to their current male partners was 18.9% (95% CI 15.1–2.6). The overall prevalence of disclosure of the HIV status of the current male partners to the young women was 64.5% (95% CI 59.9–69.0). Figure 1 further shows that the prevalence of one-way disclosure of the HIV status of the current male partners to the young women was 10.2% (95% CI 7.3–3.0). The specific prevalence of HIV status disclosure to the young women by the current male partners who knew they were initially HIV negative was higher (92.0% (95% CI 88.2–95.7)) but slightly lower (78% (95% CI 69.8–86.1)) among the current male partners who knew they were initially HIV positive. The prevalence of two-way disclosure of HIV status was 54.4% (95% CI 49.6–59.1) among the couples.

Prevalence of HIV status disclosure among YWLHIV and their male partners.
Women’s socio-demographic characteristics and their associations with their HIV status disclosure
The findings from the bivariate analysis for the associations between the women’s socio-demographic characteristics and their disclosure of their HIV status to their current male partners revealed four significant factors. First, the women who knew their initial HIV status were almost three times more likely to disclose their status compared to those who did not know their initial HIV status (X2 23.050, df 2, p <
Women’s sexual and reproductive profiles and their associations with their HIV status disclosure
The women’s sexual and reproductive factors associated with disclosure of their HIV status to their current male partners are shown in Table 3. Several directions of associations were revealed. First, the women who debuted sexual activity at a younger age (<19 years) were significantly 30% less likely to disclose their HIV status compared to those who debuted sexual activity at an older age (20–24 years). Second, women who reported more frequent sexual activities were significantly less likely to disclose their HIV status compared to those who reported less frequent sexual activities. Third, women who had many years of sexual experience before meeting their current male partners were significantly less likely to disclose their HIV status compared to those who were sexually novices.
In the line of reproductive goals, women who desired to bear children were significantly less likely to disclose their HIV status compared to their counterparts who did not desire children. Meanwhile, women who knew that their current male partners desired to bear children were significantly twice as likely to disclose their HIV status compared to those who did not know or were unsure. Conversely, women who conceived pregnancy in the past 1 year were significantly 20% less likely to disclose their HIV status compared to their counterparts who did not conceive pregnancy in the past 1 year. In addition, women who were not getting sexual feelings were significantly 30% less likely to disclose their HIV status compared to their counterparts who were getting sexual feelings. Finally, the women who correctly perceived some of the correct benefits of the dual protection methods and those who demonstrated correct knowledge of safer conception methods and a perception of their benefits were significantly twice more likely to disclose their HIV status compared to their counterparts who did not perceive any benefit of the dual protection methods and those who did not know about the safer conception methods, respectively.
Predictors of women’s disclosure of their HIV status to male partners
The findings from the bivariate and multivariate modified Poisson regression analyses for independent predictors of women’s disclosure of their HIV status to their current male partners are shown in Table 4. Three significant independent predictors of women’s HIV status disclosure to the current male partners were identified. First was the women’s knowledge of their initial HIV status whereby women who knew they were initially HIV negative were more likely to disclose their HIV status to their current male partners compared to those who knew they were initially HIV positive. The second significant independent predictor was the women’s knowledge of their current male partner’s HIV status whereby those who knew their current male partners were HIV negative were less likely to disclose their HIV status to them compared to those who knew their current male partners were HIV positive. The third and last significant independent predictor was the current male partner’s disclosure of his HIV status to the women whereby the women who received disclosure of the current male partner’s HIV status were also significantly more likely to reciprocally disclose their HIV status to them compared to those who did not receive disclosure of their current male partner’s HIV status.
Discussion
This study conducted in semi-rural northern Uganda found a 73.3%, 18.9%, and 54.4% prevalence of overall disclosure, one-way disclosure by the young women, and two-way disclosure by both partners of each other’s HIV status, respectively (Figure 1). The 73.3% overall prevalence of HIV status disclosure found among young women in northern Uganda is below the 100% expected disclosure rate. It is, however, higher than the 49% disclosure rate for developing countries. 5 It is also higher than the disclosure rate for other SSA settings such as South Africa, Tanzania, Nigeria, and Ethiopia.22 –24,43,44 The disclosure rates from northern Uganda are nonetheless consistent with the previous studies in central Uganda and southwestern Uganda that also found a 73%–73.1%, 23.9%, and 48.7% prevalence of overall disclosure, one-way disclosure by the young women, and two-way disclosure by both partners, respectively.19,20 The 73% or higher HIV disclosure rates highlight higher disclosure rates among young women in both semi-rural northern Uganda and central Uganda compared to the rate (52%) for other developing countries. The high disclosure rates demonstrated in this study are success stories for Ugandan young women. The success may imply that the existing HIV post-test counseling and disclosure counseling within the VCT and ART programs are reaching and having positive outcomes for young people. These programs, their services, and their integrated delivery approach should therefore be maintained and scaled up to other settings where they are not available.
This study in semi-rural northern Uganda also found that the male partner’s disclosure of their HIV status to the young women was associated with a higher likelihood of reciprocal disclosure of the HIV status of the young women (Tables 3 and 4). This finding is consistent with the previous studies conducted in other SSA settings namely South Africa and Ethiopia.22,27,29,43 A male partner’s disclosure of his HIV status provides the opportunity and motivation for young women who already know their HIV status to compare whether they are concordant or discordant, and such comparison facilitates counter-disclosure of the women’s HIV status. These findings support the current policy on couple counseling and testing for HIV, post-test, and continuous disclosure counseling for individuals and couples attending HIV testing, treatment, and care programs. 45
This study also found that young women who know they are HIV negative are more likely to disclose their HIV status to their male partners compared to those who know they are HIV positive (Tables 3 and 4). This finding is consistent with previous studies conducted in the West African setting of Togo. 28 Previous studies have argued that disclosing an HIV-negative status is not as stigmatizing and challenging as disclosing an HIV-positive status due to fears of consequences like family misunderstandings, stigma, or loss of the relationships. 45 Policy and program-wise, this finding calls for more programmatic innovations to address stigma to improve disclosure rates among HIV-positive individuals.
Lastly, this study revealed that young women who knew their male partners were HIV negative (discordant) were less likely to disclose their HIV-positive status to them. 19 This finding concurs with the previous studies that found barriers to HIV-positive status disclosure such as fear of stigma and loss of the sexual partners (through separation or divorce) which affected disclosure.18,19,45 Disclosing an HIV-positive status to a sexual partner can be challenging especially if the partner is HIV negative as it may lead to family misunderstandings such as blame for infidelity. 45 With disclosure counseling focusing on the advantages and benefits of HIV status disclosure such as receiving social care and support from the partner, young women who fear disclosing their HIV-positive status can be helped to disclose. Policy and program-wise, this finding further calls for the integration of disclosure screening, counseling, and support into the routine HIV treatment and care programs for PLHIV.
Study strengths and limitations
This study possesses many strengths. The first strength is the unique phenomenon and population it investigated, which were the sexual and reproductive factors among AGYWLHIV in semi-rural SSA setting and how these factors predict the disclosure of their HIV status to their male partners. The large sample size and diverse subgroups of the AGYWLHIV allows for the generalization of the study findings. Likewise, the use of the semi-structured questionnaire allowed for the standardization of the data collection.
The study was not without limitations. First, the study did not make use of any of the theoretical frameworks for disclosure such as the disclosure process model (DPM). This affected investigations into the HIV status disclosure decision-making process, events, mediators, and outcomes. This limitation was minimized using a conceptual framework developed specifically for the study using the existing literature, statistical association and predictor analyses methods to identify the mediators (exposure factors and the covariates) associated with disclosure. Nonetheless, future studies preferably using qualitative methods should explore the HIV disclosure process using the DPM.
The use of the face-to-face interview data collection method for administering the questionnaire to the participants carried the risk of social desirability bias, particularly in relation to sensitive topics such as sexual and reproductive health behaviors. 46 This potential bias was minimized by engaging female research assistants with nursing and midwifery backgrounds who administered the questionnaire in private and confidential settings within the participating public health facilities. To further minimize the social desirability bias, the research assistants received comprehensive training on how to apply skillful probing and clarification techniques in interviews.
Another potential study limitation was the risk of measurement errors caused by participants having to recall their HIV status disclosure experiences, particularly for those who disclosed their status many years ago. To minimize this potential error, the research assistants received training on how to apply skillful probing and paraphrasing techniques in interviews.
Notably, there was no psychometric information for the questionnaire items adapted from the previous literature and those developed by the investigators. The assessment for the psychometric information was omitted because none of the questionnaire items were in the form of composite scale.
Furthermore, it is important to acknowledge that the study lacked data on some of the risk factors for HIV transmission such as the male partner’s age and number of sexual partners which could have been accurately collected by including the male partners as co-participants. Future studies on disclosure dynamics that collect data from both the AGYWLHIV and their male partners are highly recommended. A study design of such nature will provide an opportunity for cross-validation and triangulation of the data.
Also missing in this study are data on the AGYWLHIV’s motivations for disclosing or fears for concealing their HIV status. To address these, future research studies on the motivations for status disclosure among the AGYWLHIV preferably using qualitative or mixed-methods research approaches are highly recommended.
Given the absence of analyses for the predictors for nondisclosure of HIV status in this manuscript, future research studies should analyze the predictors for nondisclosure and preferably gather insights from both sides of the relationship to gain a more complete understanding of the HIV status nondisclosure dynamics in the SSA settings.
This current study’s findings present more of the HIV status disclosure dynamics for lowly educated and low-income AGYWLHIV in semi-rural settings of SSA. Therefore, the study is limited in representing the disclosure dynamics for purely urban settings where the AGYWLHIV are more likely to be of higher educational attainment, higher income, self-reliant, and with access to various communication channels including the mobile phones and social media for disclosing their HIV status.
Conclusion
The study reveals that the prevalence of HIV status disclosure to the current male partners among the AGYWLHIV in semi-rural northern Uganda is as high as 73.3%. The predictors of disclosure included the women’s knowledge of their HIV status, knowledge of their male partner’s HIV status, and the male partner’s disclosure of their HIV status. The high disclosure rate is a success story for Ugandan AGYWLHIV. It underscores the need for further investigations into the disclosure process, mediators, and outcomes to inform future capacity-building initiatives for health workers in developing countries. The high disclosure rate further underscores the need for deeper qualitative exploration of the contextual factors facilitating HIV status disclosure among young women in Uganda whether it is derived from religious beliefs to save the life of the loved ones (partners) or the ongoing Uganda government and civil society’s initiatives to recognize and engage AGYWLHIV as peer educators, HIV prevention activists, or champions in the fight against HIV/AIDS in Uganda.
To further provide opportunities and motivations for disclosure among AGYWLHIV, health workers working in HIV counseling, testing, treatment, and care programs should counsel the male partners of AGYWLHIV to test and also disclose their HIV status. Furthermore, innovative strategies that enable women, men, or couples who have tested for HIV can receive their test results and become knowledgeable about their status to disclose to each other are highly desirable.
Given the role of the male partner’s HIV status disclosure in providing the opportunity and motivations for the AGYWLHIV to counter-disclose their HIV status as revealed in this study, couple counseling and HIV testing should be a key component of all HIV testing, prevention, treatment, and care programs.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251317079 – Supplemental material for HIV status disclosure to male sexual partners and predictors among young women living with HIV in rural Uganda: a cross-sectional study
Supplemental material, sj-docx-1-reh-10.1177_26334941251317079 for HIV status disclosure to male sexual partners and predictors among young women living with HIV in rural Uganda: a cross-sectional study by Edward Kumakech, Deo Benyumiza, Marvin Musinguzi, Wilfred Inzama, Ebong Doryn, James Okello, Lydia Kabiri, Vanja Berggren and Jasper Watson Ogwal-Okeng in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We would like to acknowledge the study participants. Pre-Publication Support Service (PREPSS) that supported the development of this manuscript by providing author training as well as pre-publication peer-review and copy editing.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.