
Abstract
Background:
Contraceptive use is vital in reducing the risk of unintended pregnancies and early motherhood. Despite the well-established benefits, the uptake of modern contraceptive methods among adolescent girls and young women (AGYW) is sub-optimal in sub-Saharan Africa. Furthermore, the discontinuation rate of modern contraceptive use poses a significant challenge to its effectiveness.
Objective:
We aimed to determine a 12-month modern contraceptive discontinuation rate, reasons for discontinuation, and associated factors among AGYW in Tanzania.
Design:
Retrospective nested within the cross-sectional utilizing quantitative approach.
Methods:
We retrospectively analysed calendar data on contraceptive use collected in the 2022 Tanzania Demographic and Health Survey (2022 TDHS). The 2022 TDHS data collection was implemented between February and July 2022. The study population comprised AGYW aged 15–24 years. The unit of analysis was the contraceptive episode of use, defined as the period between the start of use and the termination of the method. Our analysis was mainly based on the discontinuation due to dissatisfaction with the method. We used a life-table method to estimate the contraceptive discontinuation rates. A frailty model was employed to assess the factors associated with the discontinuation rate.
Results:
A total of 668 AGYW with a mean (±standard deviation) age of 21.5 ± 2.1 years were included in the analysis. The overall prevalence of 12-month discontinuation rate due to dissatisfaction with the method was 32.3%. Higher discontinuation rates were observed among injectable and pills. The main reasons for discontinuation were side effects (13.7%) and change in menstrual cycle (8%). Factors associated with higher discontinuation rates included higher age (adjusted hazard ratio (aHR) 1.64, 95% confidence interval (CI) 1.06–2.51 for the 20–24 age group), residing in households headed by a female (aHR 1.40, 95% CI 1.05–1.85), and residing in the western zone (aHR 1.87, 95% CI 1.21–2.90).
Conclusion:
This study revealed a high prevalence rate of modern contraceptive discontinuation among AGYW in Tanzania. The management of side effects needs to be incorporated into programs aimed at promoting the sustained use of modern contraceptive methods.
Plain language summary
Keywords
Introduction
Modern contraceptive use is a vital component of public health and paramount in achieving sustainable development goal (SDG) number 3 (ensuring good health and well-being for all). 1 The utilization of modern contraceptives reduces the risk of unintended pregnancies and unsafe abortions, promotes birth spacing, and enhances economic empowerment among women.2,3 Globally, the utilization of modern contraceptives has shown promising progress, as evidenced by the growing trend of their use. In 2019, 46% of women of reproductive age were using modern contraceptive methods globally. 4 However, in 2022, only 22% of women of reproductive age were users of contraceptive methods in sub-Saharan Africa. 5 This shows a sub-optimal utilization of modern contraceptive methods in sub-Saharan Africa compared to global estimates. In Tanzania, only 25% of women were estimated to be users of modern contraceptive methods in 2022. 6 This calls for interventions to promote the use of modern contraceptive methods.
Although the use of modern contraceptive is a challenge in sub-Saharan Africa, the higher rate of discontinuation rate among users poses even a more threat to the achievements of the intended goals of modern contraceptive programs. In 2023, only half of the users in sub-Saharan Africa continued using modern contraceptives just 1 year after initiation. 7 In Tanzania, a recent report shows that the discontinuation rate of contraceptive use in 2022 was 34%. 6 This high discontinuation rate hinders the achievement of universal access to sexual and reproductive healthcare services, as stipulated in SDG 3.
Adolescent girls and young women (AGYW) are at higher risk of teenage pregnancies, early motherhood, and school dropouts because they face several challenges associated with the transition from childhood to adulthood.8 –10 Effective utilization of modern contraceptive methods can play a crucial role in mitigating these risks. However, in sub-Saharan Africa, AGYW are more likely to discontinue modern contraceptive use than other women of reproductive age. 11 Thus, there is a need for specific considerations to be given among this group when it comes to reproductive health and family planning.
Several studies have investigated factors associated with the use of modern contraceptive methods among women of reproductive age globally.5,12,13 Modern contraceptive use behaviours are shaped by a complex interplay of factors at the individual, interpersonal, community, and societal levels. According to the socio-ecological framework, 14 individual factors pertain to personal characteristics that directly influence behaviour, such as age, education, and health awareness. Interpersonal factors encompass the dynamics within relationships, including family influence and partner communication. At the community level, broader social networks, cultural norms, and environmental contexts play a role. Societal factors refer to structural influences, such as laws, policies, and social conditions that shape overall behaviours. Previous studies have identified several factors such as age,15,16 education attainment, 17 and household characteristics17,18 to be associated with contraceptive use and discontinuation. However, little is known about the modern contraceptive discontinuation rate and associated factors in sub-Saharan Africa. Furthermore, there is scarcity of evidence targeting AGYW who are most vulnerable to the challenges associated with non-use of modern contraceptive methods. To the best of our knowledge, we did not find any study assessing the contraceptive discontinuation among AGYW in Tanzania. Therefore, this study aimed to determine the 12-month discontinuation rate, reasons for discontinuation, and associated factors among AGYW in Tanzania. Specifically, this paper focuses on discontinuation due to dissatisfaction and fertility-related reasons.
Methods
Study design
This was a retrospective study nested within a cross-sectional study design, utilizing secondary data from the 2022 Tanzania Demographic and Health Survey (2022 TDHS). The 2022 TDHS is a nationwide survey conducted to measure various health indicators, such as family planning, maternal and child health, fertility, sexually transmitted infections (STIs) and Human immunodeficiency virus (HIV), gender-based violence, and malaria. In particular, individuals were asked follow-up questions regarding their sexual and reproductive health histories, including pregnancy, birth, termination, and contraceptive use for the past 5 years preceding the survey. In this paper, we retrospectively analysed the contraceptive use calendar data to determine the 12-month discontinuation rate among AGYW in Tanzania. The reporting of this study conforms to strengthening the reporting of observational studies in epidemiology statement. 19
Study population
The participants in this study included AGYW aged 15–24 years. We included AGYW with at least one episode of modern contraceptive use in the past 5 years preceding the interview date. AGYW who reported to be sterilized were excluded from the analysis as there is no probability of discontinuation for this method. Since the main interest was to analyse discontinuation due to method dissatisfaction, individuals who stopped using modern contraceptive methods because they wanted to become pregnant were excluded from the analysis.
The sample design
The sample design for the primary survey has been described in the 2022 TDHS final report. 6 Briefly, the 2022 TDHS employed a two-stage stratified sample design. In the first stage, the probability proportional to size was used to select 629 clusters consisting of enumeration areas constructed from the 2012 Tanzania population and housing census. In the second stage, 26 households were selected systematically from each cluster making a total of 16,354 households. From each household, women of reproductive age (15–49) were interviewed resulting into 15,254 respondents. In this study, a total of 668 eligible AGYW aged 15–24, contributing a total of 787 episodes, were included.
Data extraction procedures
The data for this study were extracted from the calendar data containing reproductive and contraceptive use history in the past 5 years as described in the guide to Demographic and Health Survey (DHS) statistics. 20 We started by creating a dataset of episodes of contraceptive use, each representing one observation or case. This involved creating separate variables for each month in the calendar. The variables included: the date the episode began in century months (CMC), the date the episode ends in CMC, the duration of the episode, the type of method for each episode, and the reason for discontinuation. Specific modern contraceptive methods included were pills, injectables, implants, and male condoms. We did not include the lactational amenorrhea method because this method is used only for six months. Emergency contraceptives were also excluded because the method is not intended to be used continuously.
Study variable
Outcome variable
The outcome variable for this study was modern contraceptive method discontinuation. An individual was considered to have discontinued modern contraceptive use if she or her partner had terminated at least once following the initiation of the method in the calendar. Those who switched to another modern method within 3 months after terminating the previous one were not considered to have discontinued a method.
Independent variables
Independent variables for this study were identified based on different literature on the contraceptive use behaviours. These variables included socio-demographic characteristics, such as age, residence, education level, marital status, sex of household head, geographical zones, occupation, household size, exposure to the internet, and media exposure to family planning; and reproductive health variables: fertility preferences, number of living children, distance from health facility, multiple sex partners, and age at first sex. The variables were then classified at four levels of socio-ecological model, namely individual factors comparing age, education level, and age at first sex; interpersonal factors comprising marital status, household characteristics, children, sexual partners, and fertility preference; community factors comprising place of residence, distance from health facility, and geographical zones; and societal factors comprising internet use and media exposure on family planning. This classification enabled us to understand the multi-faceted levels of factors associated with modern contraceptive discontinuation among AGYW.
Statistical analyses
The unit of analysis for this study was the episode of use of modern contraceptive methods. Data were weighted and adjusted for clustering and stratification before analysis. We started by summarizing the participants’ characteristics using means and standard deviation for continuous variables and frequency and percentages for categorical variables. Using a life-table approach, we calculated the discontinuation rate within a 12-month follow-up period, disaggregated by specific methods and reasons for discontinuation. We used a shared frailty model, with Weibull distribution and a Gamma frailty to examine the factors associated with a 12-month discontinuation rate among AGYW. The frailty model allowed to account for unobserved heterogeneity among individuals with more than one episode (shared individual characteristics for different episodes).21 –23 All analyses were performed using STATA (StataCorp LLC, College Statation, Texas 77845, USA) version 17. 24
Results
Participants’ characteristics
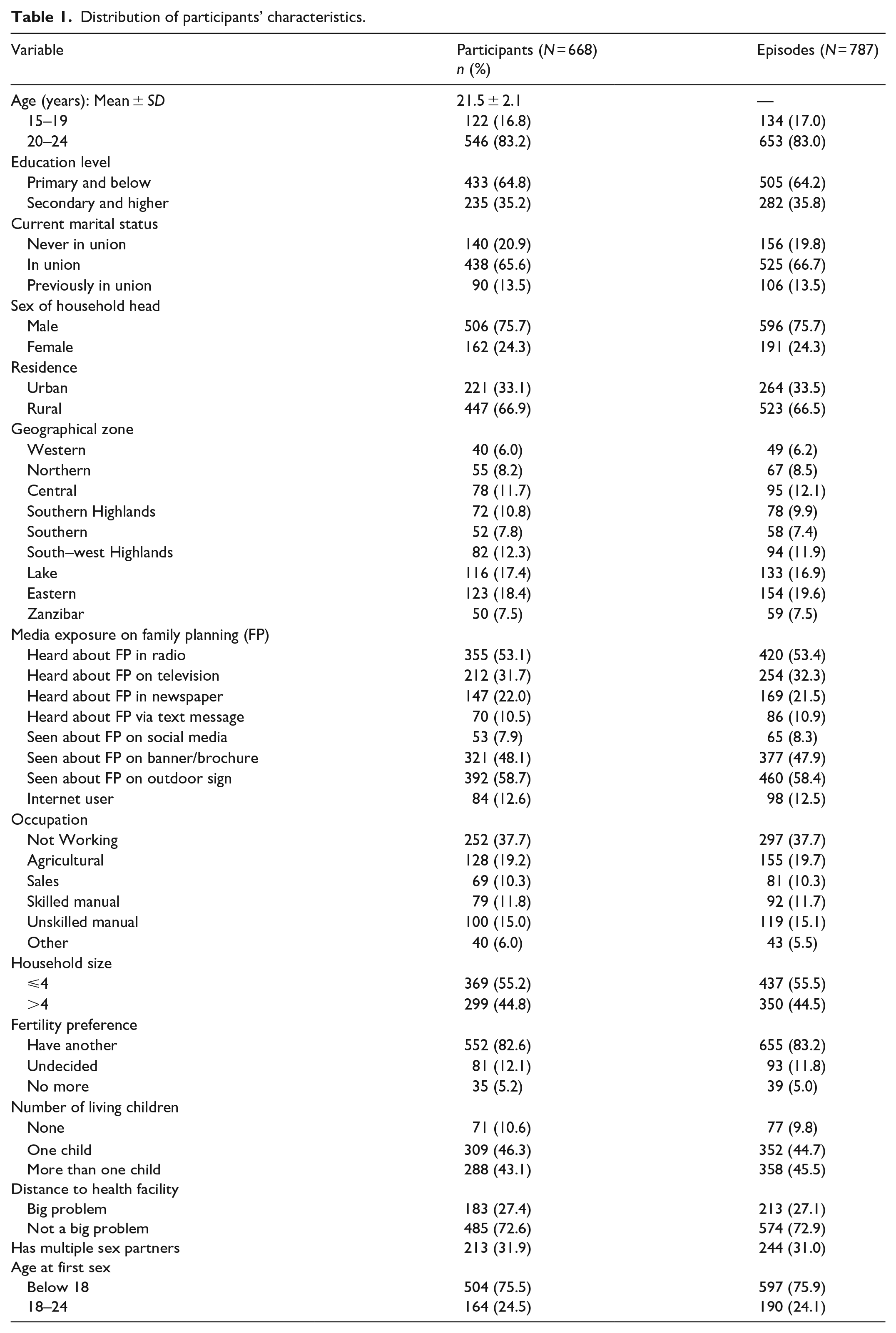
A total of 668 AGYW with mean (±SD) age of 21.5 ± 2.1 years were included in this analysis. The total episodes contributed by all participants and included in the analysis were 787. Majority of them were aged 20–24 (546, 81.7%), had primary or below education (433, 64.8%), were married/living with partners (438, 65.6%), and residing in rural areas (447, 66.9%; Table 1).
Distribution of participants’ characteristics.
Prevalence of modern contraceptive method discontinuation
Figure 1 shows the prevalence rate of discontinuation by method type. The rates for intrauterine devices (IUD) and female condoms were not estimated due to the small number of episodes (4 for IUD and 2 for female condoms). The overall proportion of AGYW discontinued at 12 month was 32.3%. The highest discontinuation proportion injectables (53.3% based on 354 episodes), followed by pill (52.0% based on 76 episodes). Implants and male condoms had a discontinuation rate of 19.8% (based on 554 episodes) and 19.2% (based on 112 episodes), respectively (Figure 1).

Discontinuation rate per method.
Reasons for 12-month modern contraceptive discontinuation
Figure 2 shows the reasons for 12-month discontinuation of modern contraceptive use. The most prevalent reason was side effects or health concerns, accounting for 13.7%, followed by change in the menstrual cycle accounting for 8%. Other reasons included a desire for a more effective method (3.9%) and other method-related issues such as cost, lack of access, inconvenience, and fatalism, which accounted for 3.5% of all reasons. Furthermore, fertility- and relationship-related factors such as infrequent sex, husband or partner disapproval, and marital dissolution or separation accounted for 1.8%. Method failure, defined as becoming pregnant while using contraception, accounted for 1.5% of all reasons.

Reasons for discontinuations.
Factors associated with modern contraceptive discontinuation
Table 2 summarizes the results from the frailty model of factors associated with contraceptive use (both bivariate and multivariable models).
Results of the shared frailty model for the factors associated with modern contraceptive discontinuation.
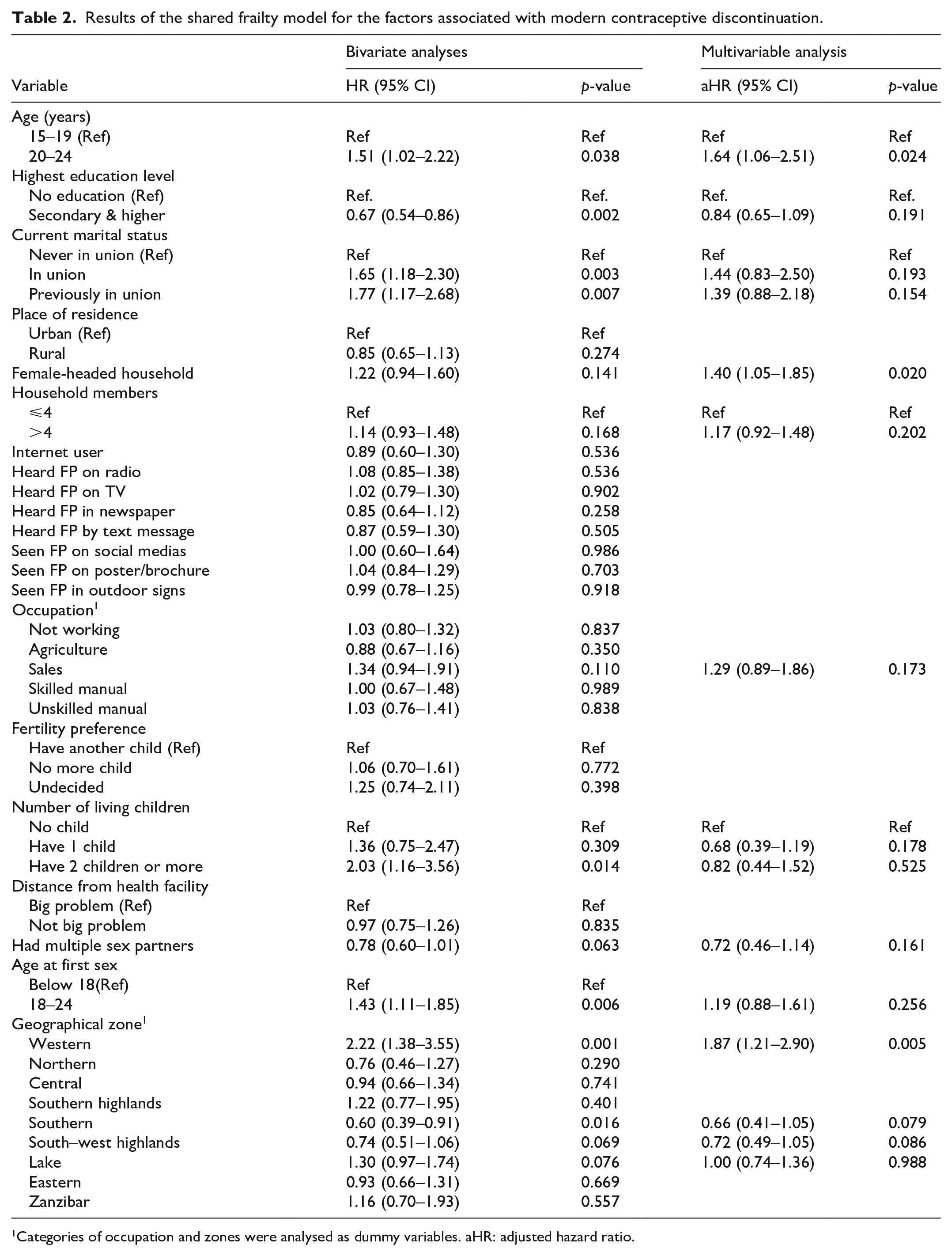
Categories of occupation and zones were analysed as dummy variables. aHR: adjusted hazard ratio.
Bivariate analyses
In the bivariate analyses, the factors associated with a high hazard of discontinuation were: older age (HR 1.51, 95% CI 1.02–2.22 for the 20–24 age group), being in marital union (HR 1.65, 95% CI 1.18–2.30) or previously in union (HR 1.77, 95% CI 1.17–2.68), having at least two living children (HR 2.03, 95% CI 1.16–3.56), history of pregnancy termination (HR 1.74, 95% CI 1.26–2.39), and late age at sexual intercourse (HR 1.43, 95% CI 1.11–1.85 for those who had first sexual encounter at age 18 and above). On the other hand, education attainment (HR 0.67, 95% CI 0.54–0.86 for secondary education and higher) was associated with lower hazard of discontinuation. Furthermore, there was also a variation of hazards of modern contraceptive discontinuation by geographical zones with Western zone (HR 2.22, 95% CI 1.38–3.55) and Lake zone (HR 1.30, 95% CI 0.97–1.74) having higher hazard, while those residing in Southern zone exhibited lower hazard of discontinuation (HR 0.60, 95% CI 0.39–0.91).
Multivariable analysis
In the multivariable shared frailty model, three factors (age, female-headed households, and geographical zones) were associated with independent associated with modern method discontinuation among AGYW. Higher hazards of discontinuation were observed among older AGYW (aHR 1.64, 95% CI 1.06–2.51 for the 20–24 age group), those residing in households headed by a female (aHR 1.40, 95% CI 1.05–1.85), and those residing in the western zone (aHR 1.87, 95% CI 1.21–2.90).
Discussion
The high rate of modern contraceptive discontinuation is one of the major challenges to achieving universal access to reproductive health and family planning. In this paper, we examined the 12-month modern contraceptive discontinuation rate and associated factors among AGYW in Tanzania. The findings from this study may be used to inform different policies and strategic plans on reproductive health and family planning.
Overall, the 12-month prevalence rate of discontinuation of modern methods due to dissatisfaction and other fertility-related reasons among AGYW was 32.3%. This presents a significant high discontinuation rate among this subgroup. The estimated prevalence rate in this study was much lower than the pooled estimate of 68.7% discontinuation rate among AGYW in three countries in West Africa (Niger, Burkina Faso, and Mali). 11 However, our estimate was much higher than the discontinuation rate of 20% estimated among adolescents in Nigeria in 2018. 25 This disparity in the findings highlights the need for country specific studies to understand the modern contraceptive use challenges among AGYW.
The findings from this study showed a variation in the rate of modern contraceptive use by method type, with the highest rates observed for injectable and pills, each with over 50% of users discontinuing within 12 months following initiation for each. The high rate of discontinuation for these two methods may be attributed to the burden of regular use, with injectables requiring administration every three months and pills requiring daily intake, unlike long-acting methods. Furthermore, AGYW may face several challenges, such as stigma and access barriers to methods with a high frequency of use, which increases the likelihood of discontinuation. Similar findings were reported in Myanmar and Kenya.26,27 These findings underscore a need for continuous contraceptive counselling and support especially for methods with increased frequency of use, such as injectables and pills. Furthermore, long-acting methods may be the best option for AGYW especially in the settings with high social stigma and access barriers.
Several reasons for 12-month discontinuation of modern contraceptive use were revealed in this study. Side effects were the most prevalent reason, followed by change in menstrual cycle, all together contributing for over 20% of all reasons. This cements on different literature that has cited side effects as the main reason for discontinuation of modern contraceptive methods.28 –30 The failure rate accounted for 1.5%, which is lower compared to the estimated method failure rate of 8% in sub-Saharan Africa. 31 This failure rate is of a public health concern as it raises the question of effectiveness of modern contraceptive methods. This calls for continuous counselling and support to the users on the management of side effects and other health concerns, which may help to reduce the discontinuation rates among AGYW.
In this study, the discontinuation rate was associated with some factors ranging from individual to interpersonal to community factors. At the individual level, older age was associated with higher discontinuation rate. At the interpersonal level, female-headed household was associated with a higher rate of discontinuation. At the community level, we found the disparity in discontinuation rates among geographical zones. None of the variables at the societal level was associated with modern contraceptive discontinuation among AGYW.
Individuals aged 20–24 had higher rate of discontinuation compared to those aged 15–19. This could be due to several factors, such as changes in reproductive goals, or shifts in relationship status as they grow older. This finding aligns with the findings reported in Kenya in 2022 15 and in Guinea in 2022. 32 This association emphasizes the necessity for age-specific interventions and support mechanisms to address the distinct challenges and requirements of older AGYW in contraceptive decision-making and continuation.
AGYW residing in households headed by females showed higher rate of discontinuation compared with those in the household headed by males. Our findings are in line with the study conducted in Ethiopia in 2019, which found that female-headed households had lower odds of using modern contraceptive methods. 17 In patriarchal societies, male-headed households are typically associated with decision-making authority, especially in areas like financial and reproductive matters. However, when women head households, they often face unique socioeconomic challenges, such as lower income and limited access to resources, which can affect their overall empowerment. 18 This economic vulnerability may limit their ability to consistently access and use modern contraceptives. While female household heads may have greater autonomy in making reproductive health decisions, this autonomy does not always translate into better outcomes due to these underlying challenges. The findings underscore the importance of understanding the dynamics within households and their impact on reproductive health decisions.
In the context of geographical zones, AGYW from the Western zone demonstrated higher rate of discontinuation. This could be due to limited access to healthcare facilities, cultural attitudes (such as religion beliefs) towards contraceptive use, lower socioeconomic status, or insufficient education and awareness about modern contraceptive methods in the Western zone. 33 Our findings cement to previous study conducted in the North-Western of Tanzania where by about one-third of women of reproductive age discontinued contraceptive use within 12 months. 34 Our findings are comparable to the study in Papua New Guinea which found the geographical disparities in modern contraceptive discontinuation among women of reproductive age in 2018. 35 This regional disparity emphasizes the importance of regional specific interventions tailored to context situation.
Strengths and limitations
The main strength of this study is the use of nationally representative data, which ensured the robust estimates of the discontinuation rate at country level. Furthermore, the use of a shared frailty model enabled us to take care for the heterogeneity of the individuals with several episodes of discontinuation, hence improving the precision of the hazard rate estimates.
This study has some limitations. First, we used retrospective data on the calendar for the past 5 years, which is likely to suffer from the recall bias. Second, since this was the analysis of secondary data, we were limited to only variables collected during the main survey. Variables such as religion and other culturally related factors, which play a key role in influencing the use of modern contraceptive methods, are not collected in Tanzanian demographic surveys and, therefore, could not be captured in our analysis. However, the inclusion of Tanzanian zones in the analysis may have accounted for some cultural variation, especially at the community level. Further studies are warranted to explore the role of cultural aspects, such as religion, in influencing modern contraceptive use among AGYW. Third, we did not account for time-varying covariates, which might affect the interpretation and generalizability of the findings. Future studies should consider utilizing prospective design to track time-varying covariates, allowing for the assessment of how changes in these factors influence contraceptive use and discontinuation among AGYW.
Conclusion
This study revealed a high prevalence rate of modern method discontinuation among AGYW in Tanzania. The methods with higher discontinuation rates were injectables and pills. The main reasons of discontinuation were side effects and change in menstrual cycle. Factors such as older age, female-headed household, and living in western zone were associated with higher discontinuation rate. The findings highlight a significant challenge in modern contraceptive use among AGYW, emphasizing the need for targeted interventions to promote the continuous use. Addressing this issue is essential in improving reproductive health outcomes among AGYW.