
Abstract
Uterine fibroids, known as leiomyomas, are non-cancerous tumors in women. Uterine fibroids disproportionately affect African American women, as they are more common and severe. Uterine fibroids are the leading cause of hysterectomy in African American women. Over 80% of African American women will receive a uterine fibroids diagnosis before 50. Myomectomies (removal of uterine fibroids) and hysterectomies (removal of the uterus) are more prevalent in African American women due to more significant symptoms. Socioeconomic status, including education and income, influences access to healthcare, with some treatments directly affected by insurance coverage and the cost of the procedure. This review aimed to characterize the socioeconomic disparities and inequities regarding uterine fibroids awareness, perceptions, and treatment and to understand how socioeconomic status impacts knowledge and treatment of uterine fibroids. Recognition of the treatment barriers and decisions due to socioeconomic status is a critical step in ensuring equitable treatment options for women diagnosed with uterine fibroids. A narrative literature review was conducted using PubMed, MedLine, and Google Scholar. A total of 98 articles were returned. After adjusting for the exclusion criteria, 10 articles were included in this review. The review demonstrated the disparities in treatment options based on race and socioeconomic status. Low-income women were more likely to receive more invasive treatment, which resulted in more time off work and increased medical bills. In addition, women in lower-income brackets frequented the emergency department at an increased level. This review underscored the need for additional research to learn about the role of socioeconomic status in uterine fibroid awareness and treatment.
Plain language summary
Uterine fibroids, known as leiomyomas, are non-cancerous tumors in women. Uterine fibroids disproportionately affect African American women, as they are more common and severe. Uterine fibroids are the leading cause of hysterectomy in African American women. Over 80% of African American women will receive a uterine fibroid diagnosis before 50. Myomectomies (removal of fibroids) and hysterectomies (removal of the uterus) are more prevalent in African American women due to more significant symptoms. Socioeconomic status, including education and income, influences access to health care, with some treatments directly affected by insurance coverage and the cost of the procedure. This review aimed to characterize the socioeconomic disparities and inequities regarding uterine fibroid awareness, perceptions, and treatment and to understanding how socioeconomic status impacts knowledge and treatment of uterine fibroids. Recognition of the treatment barriers and decisions due to socioeconomic status is a critical step in ensuring equitable treatment options for women diagnosed with uterine fibroids.
Introduction
Uterine fibroids are non-cancerous (benign) tumors of the uterus. They are also referred to as leiomyomas and myomas, and symptoms include heavy menses, pain, reproductive issues, anemia, and frequent urination. 1 Uterine fibroids are the leading cause of hysterectomies. Throughout the past few decades, research has shown that there is a disproportionate effect on African American women. For instance, one research article revealed that more than 80% of African American women and 70% of white women would receive uterine fibroids diagnosis by age 50. 2 African American women have a higher cumulative risk and a chance of earlier onset of uterine fibroids symptoms and diagnosis. 2 Myomectomies (removal of fibroids) and hysterectomies (removal of the uterus) are more prevalent in African American women due to more significant symptoms. African American women are two to three times more likely to undergo a hysterectomy than white women and 6.8 times as likely to receive a myomectomy. 3 Uterine fibroids are associated with increased financial burdens. There are direct medical costs and lost work-hour costs due to women calling off due to uterine fibroids symptoms. 4 In addition, racial and ethnic minorities and women within lower socioeconomic status (SES) experience poor quality of life compared to women of higher SES. Not much is known about why African American women elect to have hysterectomies instead of the less invasive procedures for dealing with uterine fibroids. Some studies attribute the disparity to differences in socioeconomic or psychosocial factors. Other studies attribute the differences in treatment to differences in access to healthcare, levels of education, and various lifestyle behaviors. 5 One proposed hypothesis is that individuals with lower SES may be less knowledgeable about alternatives to hysterectomy and might subsequently delay seeking care longer until gynecological problems are too severe to pursue other less invasive options.
SES, includes, but is not limited to education, income, occupations, and access to healthcare. SES is known to influence access to healthcare and research has shown that both race and SES impact access to quality care, including access to minimally invasive uterine fibroids treatments. Education is included in SES, and thus there is a known connection between education level and health literacy levels. Limited health literacy is a social determinant that leads to women not understanding treatment options and thus receiving more invasive surgical treatment options. Hysterectomies increase among women of lower SES. As such, women who earned higher incomes and who had more advanced education opted for less invasive treatment. 5
This review aimed to characterize the socioeconomic disparities and inequities regarding uterine fibroids awareness, perceptions, and treatment and to understand how SES impacts knowledge and treatment of uterine fibroids.
Materials and methods
This narrative review investigated the available data regarding the association between SES and uterine fibroids. PubMed, Google Scholar, and Medline were used to search the literature for articles published between 2013 and 2023. The goal was to assess the current literature; therefore, only 10 years of worth of literature was reviewed. The search used the following keywords: uterine fibroids, fibroids, uterine leiomyomas, myomas, income, and SES. There were a total of 98 articles screened. A total of 88 articles were excluded due to publication date, non-US, having a primary focus other than uterine fibroids, and being abstract only (Figure 1). In addition, duplicate articles or similar articles by the same authors were excluded. After exclusion, a total of 10 articles were included in this review.
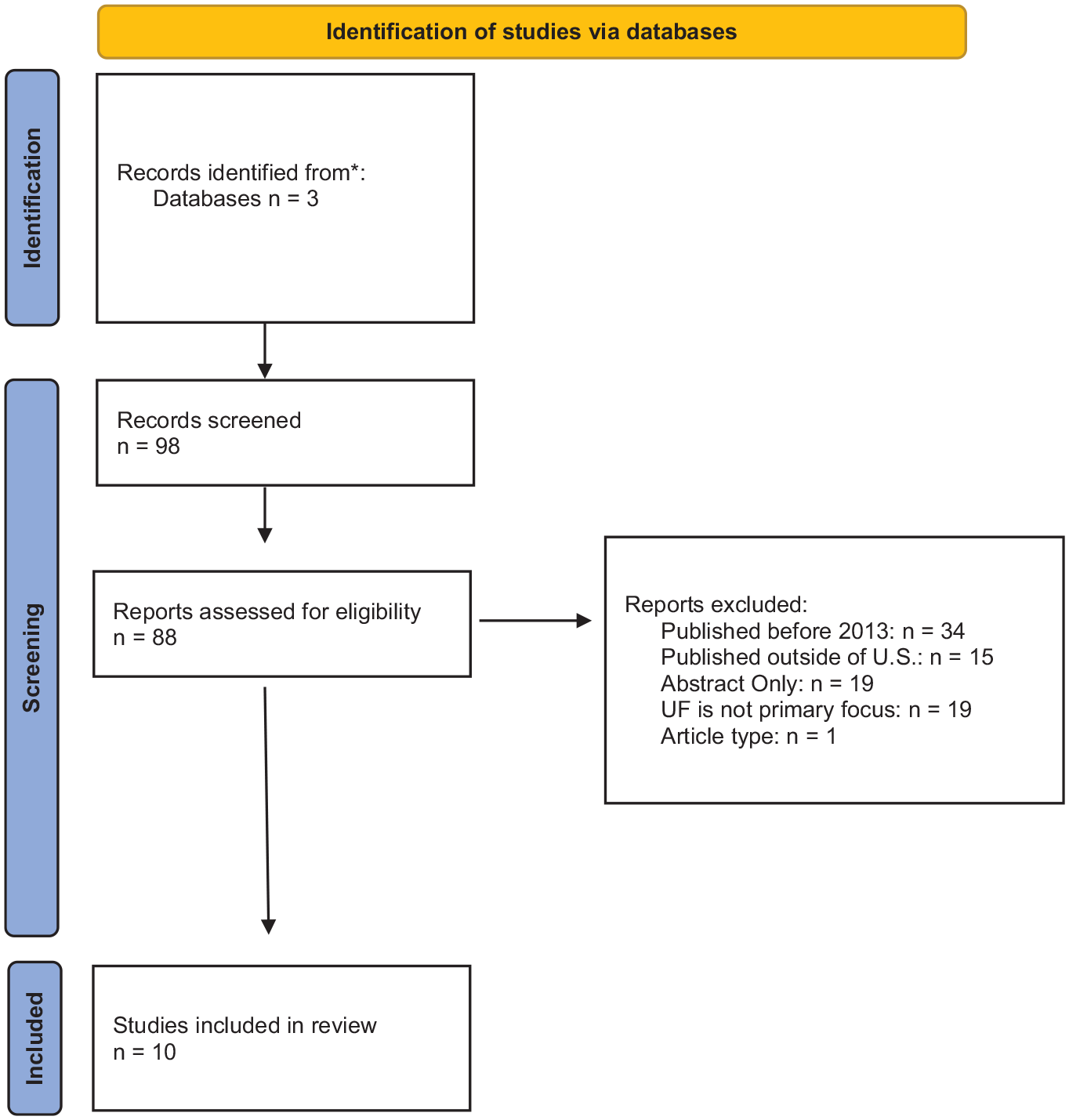
Identification of studies.
Results
Socioeconomic status
The American Psychological Association (APA) defines SES as “the position of an individual or group on the socioeconomic scale, which is determined by a combination of social and economic factors such as income, amount and kind of education, type, and prestige of occupation, place of residence, and—in some societies or parts of society—ethnic origin or religious background.” The APA goes on to state that numerous examinations of SES reveal inequities concerning access to resources and care. SES, including education and income, influences access to healthcare, with some treatments directly affected by insurance coverage and the cost of the procedure. SES and race are known to impact access to adequate and quality healthcare, and access to some forms of uterine fibroid treatments is affected by insurance type and insurance status. The inequities associated with uterine fibroids treatment are a concern, and more studies are needed on diagnosis as well as treatment decisions among African American women, especially those of lower SES.
Historically, women are paid less than men, and many have fewer work benefits. Over 25% of women diagnosed with uterine fibroids reported that symptoms keep them from reaching their full potential in their careers. Results from the National Institute of Environmental Health Sciences Sister Study revealed that education levels and being poor were associated with an increased incidence of uterine fibroids. SES and race impact women’s access to appropriate healthcare and treatment. Stewart et al. reported results from an online survey conducted from December 1, 2011, to January 16, 2012. There were 841 women, 268 African American, and 573 white. 4 Approximately 55% of the participants earned an annual income of less than $50,000, and about 45% earned more than $50,000. Approximately 31% graduated from college or had some graduate-level education. The results revealed that African American women were more stressed about employment due to missed work days. African American women were 77% more likely to call off from work, and 61% had concerns regarding loss of income. 4
Emergency department visits continue to increase among women with uterine fibroids. Fortin et al. examined the trends in emergency department utilization among women with fibroids. The researchers retrospectively reviewed the Healthcare Cost and Utilization Project Nationwide Emergency Department Sample database from 2006 to 2017. There were a total of 533,963 emergency department visits during the period. 5 The study showed that emergency visits increased from 28,732 in 2006 to 65,685 in 2017. Most women seeking care in the emergency department were in the lowest income bracket (36.1%) and most likely to be from the South region (46.2%). Income was not a predictor of admission. However, uterine fibroids are a chronic condition, and many women seek treatment in the emergency department. Fortin et al. demonstrated that the increased emergency department visits among lower-income women tend to occur due to a lack of primary care physicians and access to primary care services. This presents a challenge due to the cost of emergency visit charges doubling from $2586 to $6193 during the study period. 6 Consequently, the number of admissions for uterine fibroid-related symptoms or issues decreased. The study was consistent with other studies reporting that hospital admissions increase based on the woman’s age, with a peak admission rate among women 40–54. 6
Awareness and perceptions
Marsh et al. analyzed data from the online uterine fibroids patient survey between June 30 and September 6, 2016. 1 Over 1440 women completed the study and were divided into three groups: at-risk at 300, diagnosed at 871, and hysterectomy at 272. Almost half of the women in the study reported having heard of uterine fibroids. Women in the study with an annual income of over $60,000 had a greater awareness of uterine fibroids than women with a yearly income between $24,000 and $59,000 and women with an income less than $24,000 (60% vs 44% vs 43%). 1
VanNoy et al. conducted semi-structured interviews with African American women undergoing uterine fibroids surgery. 7 Most of the interview participants were college-educated and had health insurance. Approximately 57% of the participants reported being aware of uterine fibroids before diagnosis. The women who reported being college graduates were more aware of uterine fibroids than those with less than a college degree (76%). By contrast, a study with participants of a similar demographic reported that approximately 48% reported no knowledge of fibroids. 8 The participants had at least a 4-year college degree, insurance, and an income >$50,000. The study showed that women delayed seeking medical attention because they felt their experiences were typical. Stewart et al. stated that the African American women in the study reported more issues with the quality of life due to uterine fibroids. More than 67% of African American women said they waited more than 2–3 years before seeking treatment. 4
Uterine fibroid symptoms are a burden among women, with abnormal bleeding, pelvic pain, bloating, and frequent urination noted the most. African American women experience more severe symptoms than white women. Fuldeore and Soliman conducted an online survey of women aged 18–54. A total of 53,741 participants were included in the results. Similar to other studies, the results showed that the prevalence of uterine fibroids increased as women aged, and the prevalence was more significant in African American women. Consequently, the study did not include data or information regarding SES in the results. 9
Borah et al. surveyed women with self-reported symptomatic uterine fibroids. The participants comprised 64% White, 28% African American, and 8% of other backgrounds or mixed races. Seventy-two percent had completed some college education, and 66% were employed full time. Of those employed full time, approximately 23% had an annual income of less than $35,000, while 39% reported a revenue of over $75,000. The majority of women reported being scared and fearful of the diagnosis and that the uterine fibroids would grow. Approximately 63% of respondents believed they would experience additional uterine fibroids symptoms and eventually need a hysterectomy. Over 42% of the participants indicated that they visited at least two or more providers before receiving a uterine fibroids diagnosis. The mean reported time since diagnosis was 8.7 years. The participants perceived that uterine fibroids impacted their career progress, with approximately 28% reporting that uterine fibroids symptoms caused them to miss work within the 3 months before the survey. 10
Treatment
The treatment options for uterine fibroids vary from medication to surgery. The treatment options vary depending on the age, size, and location of the uterine fibroids, symptoms, and fertility desires. The medication options include treating the symptoms and can consist of iron supplements, birth control, pain medications, and oral therapies. The surgical options include myomectomy, which involves the removal of uterine fibroids. There are three types of myomectomies: hysteroscopy (scope through vagina and cervix), laparoscopy (inserting a scope by placing a few small incisions in the abdomen), and laparotomy (abdominal incision).
By contrast, a hysterectomy is the removal of the uterus. There are minimally invasive options for myomectomy. Other minimally invasive procedures are uterine artery embolization (UAE) and ablation. Hysterectomy, uterine fibroid embolization, and radiofrequency ablation are not recommended when women plan future pregnancies.
The rates of hysterectomies increase among women of lower SES. Findings reveal that women in the United States with lower SES tend not to seek care until the later stages of uterine fibroids diagnosis, sometimes resulting in more extensive tumors and, thus, greater hysterectomies. When income and education levels were increased, there was a greater chance of women selecting less invasive treatment options such as myomectomy, UAE, or endometrial ablation. 5 The study by Marsh et al. revealed that the average age of women who underwent a hysterectomy for fibroids was 41. The average age was regardless of income. Of the main reasons women reported opting for a hysterectomy, 58% said it was a healthcare provider recommendation. In comparison, 55% indicated pain, and 47% stated distress due to other symptoms from the fibroids. Furthermore, approximately 33% of women who underwent a hysterectomy said they were “somewhat to extremely” interested in uterus preservation, with 50% wanting to maintain the ability and option to have children later. 1
Insurance status and type influence the type of treatment options. A US-based study conducted in 2005 revealed that women with an income of less than $61,000 and without private health insurance were less likely to receive minimally invasive surgeries. Women with higher incomes were 12%–18% more likely to have a minimally invasive procedure for uterine fibroids. In addition, a 2009 study reported that Medicaid and self-pay patients were 20%–30% more likely to have a laparotomy or abdominal hysterectomy instead of minimally invasive procedures. 11 Eltoukhi et al. further validate this stance by reporting that white women and women with private insurance are more likely to undergo laparoscopic procedures. By contrast, Hispanics, African Americans, and women with Medicare are more likely to undergo open-abdominal procedures. 2
Similarly, Frost conducted a cross-sectional study using National Inpatient Sample database data. Women who received open and minimally invasive myomectomies from January 1, 2010, to December 31, 2014, were reviewed. The data indicated that African American women accounted for the most myomectomies; however, two-thirds were open procedures. African American women had lower odds of minimally invasive myomectomies than white women across all country regions. This further shows the racial disparities that exist among uterine fibroid treatments. In contrast to many national studies, Frost reports that in the West region, women in the highest income brackets had lower odds of having a minimally invasive myomectomy than the other income brackets (OR 0.65). 12
Borah et al. conducted a retrospective analysis using the insurance claims database and reviewed procedures from 2004 to 2009. The study analyzed patient characteristics and the chances of patients undergoing uterine-sparing procedures such as endometrial ablation, myomectomy, and UAE. The sample included 96,852 patients between the ages of 25 and 54. The study concluded that women with the highest income and education (based on zip code) opted for uterine-sparing procedures at higher rates. It is important to note that the only patients in this study were those who carried commercial insurance. The study does not take into account women without insurance or with government insurance. 13
Younger African American women are at risk of needing surgery that may affect their future fertility. To further this concern, Laughlin-Tommaso and Jacoby report that uterine fibroids lead to increased rates of miscarriage, cesarean section, and premature births.5,11 Since African American women develop uterine fibroids earlier than white women, there is a greater risk for reproductive complications, especially for women with uterine fibroids that distort the endometrium. Due to the high costs of fertility treatments, African American women and low-income women, in general, are less likely to access fertility services. African Americans have an increased chance of surgical complications, mortality, and extended inpatient stays.
Discussion
Uterine fibroids are a debilitating and chronic condition. There is substantial research on the pathology and epidemiology of uterine fibroids. However, little is known about the specific impact of income and SES on uterine fibroids awareness and treatment. In this narrative review, we found consistency with articles regarding the devastating effects on African American women and women with lower incomes. 14 This historical information dates back to 2005 and aligns with the literature regarding how common uterine fibroids are in African American women and at a younger age. The data show that race and income are significant predictors of increased hysterectomies. Despite the many benefits of minimally invasive procedures, there was an underutilization. The research showed that women with higher incomes had more minimally invasive procedures.2,11 The review data demonstrate the disparities that exist in awareness, perception, and treatment of low-income women with uterine fibroids. The inadequate health insurance, daily costs associated with hygiene products, and costs of diagnostic testing add additional barriers to women of lower SES. In addition, there is a lack of understanding regarding predictors that differentiate between symptomatic and asymptomatic uterine fibroids, which acts as another barrier to prevention, screening, and possible treatment options, likely exacerbating the delay and severity of treatment options used within African American women.1,5,9
Due to the high rate of hysterectomies, there is a need for further discussion regarding fertility consequences and the costs associated with fertility treatments and egg preservation among women who still desire to have children. This is an additional burden and barrier to low-income women who do not have the knowledge, financial resources, or insurance to consider future contraception. For those women who have access to assisted reproductive technology, the research showed a decreased rate of success for women who had uterine fibroids and an increase in spontaneous abortion among African American women.15,16
The review highlights the need for practitioners to ensure adequate patient education and understanding. Ensuring that patients understand all their options and clearly explain their pros and cons is necessary. 17 A study conducted by Ghant et al. concluded that a limited understanding of uterine fibroids led to treatment delays. 8 In addition, there is the implication for professionals to ensure that their recommendation is not based on insurance status, insurance type, income level, or education. Instead, providing equitable recommendations is critical.
Another consideration when discussing SES and uterine fibroids is the role of digital health technologies. Providers cannot assume that all patients have access to smartphones and computers, or that they are technologically savvy. Some patients cannot afford phones or internet services. Therefore, there is a need to understand that populations with low SES are also likely to have challenges with digital information and digital technologies. 17
Strengths and limitations
The article’s strengths include a comprehensive review of the relevant and recent literature. In addition, the inclusion of articles from experts in the obstetrics and gynecology field added credibility to the findings. The main limitation is that only articles from the last decade were included. It is possible that key information was missed with older articles. In addition, only articles published in peer-reviewed journals were included. There may be additional gray literature that contains pertinent information, such as dissertations. Lastly, while there are many uterine fibroid articles, SES or income articles are limited, highlighting the need for additional research.
Conclusion
Health disparities and inequities significantly impact the quality of life of women diagnosed with uterine fibroids. This review demonstrates the differences in treatment options based on SES. Given the disproportionate rate of African American women having hysterectomies and reporting poor quality of life, investigating the rationale behind decisions becomes increasingly important. Hysterectomy rates remain elevated among women from lower socioeconomic backgrounds, suggesting a potential gap in knowledge regarding alternative treatments that may result in delayed care-seeking until uterine fibroids-related symptoms become severe. Numerous factors have been projected in this context to elucidate the relationship between SES and health outcomes. The review underscores the critical need for improved uterine fibroid education and treatment options among minority women and all women with low SES.