
Abstract
Background:
Uterine sarcomas (US) are rare cancer of possible occurrence even in women of childbearing age. To date, total hysterectomy is the standard treatment in the early stages. The possibilities of carrying out fertility-sparing treatments (FST) to save the fertility of women with unfulfilled reproductive desires are described in the literature, but to date, they can only be considered experimental.
Objective:
The aim of this systematic review was to evaluate the oncological and reproductive outcomes of women with different histological types of US undergoing FST.
Design:
Systematic review.
Data sources and methods:
Electronic databases were searched for English-language studies describing FST for US until January 31, 2024.
Results:
Forty-five papers which met the abovementioned inclusion criteria, were included in the qualitative analysis. Quantitative analysis was not possible because of the heterogeneity of the data. A descriptive summary of the results according to the histotype of US was provided. Six hundred forty-one patients of childbearing age with US and undergoing FST. After treatment with FST, 89 (13.9%) disease recurrences and 107 (16.7%) pregnancies were recorded.
Conclusion:
In selected cases of early-stage US, FST may be proposed. However, the patient must be informed of the real possibility of recurrence and potentially difficult achievement of pregnancy. Additional well-designed prospective studies and clinical trials are needed to address the knowledge gaps and enhance clinical decision-making in this population.
Trial registration:
PROSPERO ID: CRD42024509356.
Introduction
Background
Uterine sarcomas (US) represent a rare category of malignant soft tissue tumors, accounting approximately for 1% of all malignancies within the female genital tract and for 3%–7% of uterine cancers overall. 1 The incidence of these heterogeneous groups of tumors is estimated to range from 0.36 to 0.64 cases per 100,000 women annually in the United States. 2 While for some cancers, such as cervical and endometrial cancers, many of the mechanisms and causes leading to the onset of these diseases are known,3 –5 for sarcomas the causes remain unclear. 6
Traditionally, US have been categorized based on their histological characteristics into carcinosarcomas (malignant mesodermal mixed tumors), which represented half of the cases, leiomyosarcomas (LMSs; 30%), endometrial stromal sarcomas (ESSs; 15%), and undifferentiated uterine sarcomas (UUSs; 5%). In recent times, advancements in molecular biology have led to revisions in classification. As an example, uterine carcinosarcomas are presently categorized as dedifferentiated carcinomas due to enhanced comprehension of molecular biological distinctions. 7 According to the Vth edition of the World Health Organization (WHO) classification of female genital tumors, the predominant subtypes of US currently include LMS, succeeded by ESS and UUS.8,9 US are categorized based on their resemblance to normal uterine tissues, with homologous types resembling typical uterine components such as ESS, UUS, fibrosarcoma, and LMS; conversely, heterologous variants exhibit features uncommon in the uterus, displaying sarcomatous elements not typically present, like rhabdomyosarcoma (RMS), chondrosarcoma, osteosarcoma, and liposarcoma.8,10 The diagnosis becomes additionally challenging due to significant variations in immunohistochemistry (IHC) profiles across different types of US. This complexity hinders the utilization of IHC as a definitive method for distinguishing between various US. 11 A pivotal aspect is to accurately differentiate between US and uterine fibroids, with the latter being prevalent in up to 70% of women during their lifetime. 12 Ultrasonographic findings suggestive of US comprise central necrosis or cystic alterations, varied echotexture, and increased vascularity. Nevertheless, these traits are also commonly observed in leiomyomas. 13 At the state of art, differentiating uterine leiomyomas from uncommon sarcomas before surgery remains difficult. Typically, the latter are identified postoperatively, following myomectomy or hysterectomy performed for suspected leiomyoma, and subsequent evaluation by pathology experts. 12 Treatment approaches and follow-up of these tumors have been still controversial. In the past, laparotomy was considered the gold standard for the treatment of uterine masses. Hysterectomy, with or without bilateral salpingo-oophorectomy, is the standard treatment in stage I disease.14 –16 In recent decades, however, minimally invasive techniques have been developed to effectively remove these lesions. The implementation of advanced energy devices, along with the development of new technologies such as lasers, and the creation of new instruments represent innovations, both in laparoscopy and hysteroscopy.17 –19 Nonetheless, these advancements often result in the fragmentation of the operative sample, making the pathologist’s job of differential diagnosis even more challenging.
Fertility-sparing treatment (FST) is a conservative reproductive management for gynecologic cancers in women of childbearing age who have not yet realized their reproductive desires and/or still wish to conceive. Treatment involves removal of the neoplastic lesions while preserving the uterus and at least one ovary during surgery. In recent years, many gynecologic cancers, such as those of the endometrium, cervix, and even the ovary, diagnosed at an early stage, have been treated with a fertility-saving approach with good oncologic and reproductive results.20 –25
FST is considered a rare and experimental approach for US because of the rarity of the pathology. In addition, the lack of specific guidelines for physicians to choose the most appropriate treatment and counseling for a woman of childbearing age diagnosed with uterine sarcoma is still a difficult problem to date. In this context, comprehensive, reliable, and currently available data were analyzed to inform the most effective approaches to be carried out to preserve fertility in patients with US.
Objectives
The aim of this study was to evaluate the oncological and reproductive outcomes of women with different histological types of US undergoing FST.
Methods
Eligibility criteria
Only original studies (retrospective or prospective) reporting FST of US were deemed eligible for inclusion in this systematic review.
Studies involving sarcomas in other organs of the gynecological system, studies regarding uterine tumors of different histological origins, or describing only the procedure technique (“step by step” procedure description) were excluded.
Information sources
This study was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 26 available through the Enhancing the Quality and Transparency of Health Research (EQUATOR) network, and the Cochrane Handbook for Systematic Reviews 27 and registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42024509356.
MEDLINE, EMBASE, Global Health, The Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register), Health Technology Assessment Database, Web of Science, and research register (ClinicalTrial.gov) were searched for studies describing surgical procedures for FST of US.
Search strategy
The following medical subject heading (MeSH) and key search terms were used: "Sarcomas" (MeSH Unique ID: D012509) OR "Adenosarcoma of the uterus" (MeSH Unique ID: C538232) OR "Carcinosarcoma" (MeSH Unique ID: D002296) OR "Endometrial stromal sarcoma" (MeSH Unique ID: D018203) OR "Leiomyosarcoma" (MeSH Unique ID: D007890) OR "Rhabdomyosarcoma" (MeSH Unique ID: D012208) OR "Uterine smooth muscle tumors of uncertain malignant" OR "Uterine neoplasms" (MeSH Unique ID: D014594) AND "Assisted reproductive techniques" (MeSH Unique ID: D027724) AND "Conservative treatment" (MeSH Unique ID: D000072700) OR "Fertility-sparing" (MeSH Unique ID: D059247). We selected papers written in English, since the inception of each database until January 31, 2024.
Study selection
Titles and/or abstracts of studies retrieved using the search strategy were screened independently by two review authors (A.E. and A.S.L.) to identify studies that met the inclusion criteria. The full texts of these potentially eligible articles were retrieved and independently assessed for eligibility by two other review team members (A.D. and E.G.). A manual search of the references of the included studies was conducted to prevent the omission of pertinent research. Any disagreement between them over the eligibility of articles was resolved through discussion with a third (external) collaborator. All authors approved the final selection.
Data extraction
Two authors (B.A. and A.G.) independently extracted data from articles about study features, characteristics of included populations, surgical procedures, complications and results/outcomes using a pre-piloted standard form to ensure consistency. One author (V.C.) reviewed the entire data extraction process.
Assessment of risk of bias
Two reviewers (E.C. and E.G.) assessed independently the risk of bias of studies included in this systematic review using a modified version of the “Newcastle-Ottawa Scale.” 28 Quality of studies was evaluated in the following five different domains: “study design and sample representativeness,” “sampling technique,” “description of the fertility-sparing treatment,” “quality of the population description,” “incomplete outcome data” (Supplemental Table S1). Any disagreements between the reviewers were resolved by a third reviewer (A.C.).
Outcomes measures and data synthesis
The primary outcome of this study was to evaluate the oncologic and reproductive outcomes of women with uterine smooth muscle tumors of uncertain malignant and sarcomas undergoing FST.
Quantitative analysis was not possible due to data heterogeneity (including different settings and surgical procedures). We provided a descriptive synthesis of the results in separate sections based on the histological subtype of uterine smooth muscle tumors of uncertain malignant and sarcomas treated by FST.
The body of evidence on the usefulness of FST for uterine smooth muscle tumors of uncertain malignant and sarcomas was assessed by two authors (A.S., V.A.) using the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence (OCEBM). 29
Results
Study selection
Study selection is displayed in Figure 1. After the evaluation of full texts, a total of 45 papers,30 –74 which met the abovementioned inclusion criteria, were included in the present systematic review.

PRISMA flow diagram.
Study characteristics
The main characteristics of the included studies are summarized in Table 1.
Characteristics of the included studies.

AS, adenosarcoma; ERMS, embryonal rhabdomyosarcoma; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; LG-ESS, low-grade endometrial stromal sarcoma; STUMP, uterine smooth muscle tumors of uncertain malignant potential.
Seventeen studies were retrospective,31,37,43,44,49 –52,56,58,60,61,64,69,70,72,73 8 were case series,32 –34,45,48,59,68 and 21 were case reports.30,35,36,38 –42,46,47,53 –55,57,62,63,65 –67,71,74
Of these, 12 studies were from China,31,39,40,42,44,45,50,56,70 –73 5 were from Korea,36,43,49,63,64 4 were from Italy,48,51,57,74 5 were from the United States,32,37,38,55,66 3 were from Turkey,30,61,69 2 were from the United Kingdom,34,52 2 were from Canada,33,53 2 were from Japan,54,68 2 from Germany,59,67 2 from Poland,58,65 1 from Taiwan, 35 1 from Singapore, 41 1 from India, 46 1 from Czech Republic, 60 1 from Spain, 62 and 1 from France. 47
Risk of bias of included studies
Of the 45 studied included, 30 were at low risk of bias in three or more domains,31,34 –39,41 –43,45 –48,54 –57,59 –61,63,66 –68,70 –74 while 15 were judged at high risk of bias.30,32,33,40,44,49 –53,58,62,64,65,69 A detailed description of the risk of bias in each domain among studies is reported in Supplemental Table S2.
Synthesis of the results
Among the included studies, 22 evaluated the reproductive and oncological outcomes after FST in patients with ESS,31,35,36,38 –40,42,45,47,48,51,52,54,57,58,62,63,66,69 –71,73 13 in patients affected by RMS,30,32 –34,37,46,50,53,55,58,59,65,67 6 in patients with uterine smooth muscle tumors of uncertain malignant potential (STUMP),43,44,56,60,61,64 5 in patients suffering from adenosarcoma (AS),41,49,68,72,74 and 2 in patients with LMS.58, 69
Notably, in the series by Tunc et al. 69 were included patients with both low-grade endometrial stromal sarcoma (LG-ESS) and LMS. Finally, Piątek et al. 58 evaluated the oncological and reproductive outcomes in patients affected by different types of sarcoma, including ESS, RMS, AS, and LMS. As previously mentioned, we discussed the results separately based on the histological subtype of STUMP and sarcomas treated by FST.
We comprehensively included 641 patients of childbearing age with US and undergoing FST were included: 9 (1.4%) with LMS, 222 (34.6%) with ESS, 47 (7.3%) with RMS, 95 (14.8%) with AS, 1 (0.1%) with low-grade myofibroblastic sarcoma (LGMS), 267 (41.6%) with STUMP. Eighty-nine (13.9%) disease recurrences were recorded after FST treatment. Specifically, 6 (66.7%) patients with LMS, 46 (20.7%) patients with ESS, 6 (12.8%) patients with RMS, 4 (4.2%) patients with AS, 1 (100%) of the patients with LGMS, 26 (9.7%) of the patients with STUMP. After FST a total of 107 pregnancies (16.7%) were achieved, namely: 3 (33.3%) for LMS patients, 34 (15.3%) for ESS patients, 6 (12.8%) for RMS patients, 4 (4.2%) for AS patients, 2 (100%) for LGMS patients, and 58 (21.7%) for STUMP patients.
Leiomyosarcoma
Two studies evaluated the oncologic and reproductive outcomes after FST of LMS. Data regarding the included studies are shown in Tables 2a and b.
(a) Oncological outcomes of studies reporting FST for LMS.

AWD, alive with disease; BMI, body mass index; DOD, died of disease; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; IMA, ifosfamide and nimustine; LMS, leiomyosarcoma; LND, lymph node dissection; NED, no evidence of disease; THBSO, total hysterectomy with bilateral salpingo-oophorectomy.
(b) Reproductive outcomes of studies reporting FST for LMS.

ART, assisted reproductive technology; CS, cesarean section; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; LMS, leiomyosarcoma.
Seven patients (53.8%) within the cohort studied by Tunc et al. 69 underwent fertility-preserving surgical procedures. Three patients underwent adjuvant therapy with ifosfamide + nimustine (IMA). Five out of the seven patients relapsed (71.4%). Three of them (60%) subsequently underwent debulking surgery; in one case (20%) a local excision and unilateral inguinofemoral lymph node dissection (LND) were performed due to a inguino-vulvar recurrence; in the remaining patient (20%), a surgical approach was deemed unfeasible. At the last follow-up, three patients were alive (42.9%) and four patients (57.1%) died of disease (DOD). Three live births (42.9%) occurred.
Two out of the 11 patients included in the study by Piątek et al. 58 were treated conservatively for LMS, through hysteroscopic or abdominal mass resection. A recurrence occurred in one patient (50%), requiring a total hysterectomy with bilateral salpingo-oophorectomy (THBSO). No pregnancies were recorded in the two cases.
Quality of evidence: The evidence regarding the safety, effectiveness, and reliability of FST for the treatment of LMS was classified as evidence level 2b.
Endometrial stromal sarcoma
Twenty-two studies assessed the reproductive and oncological results following FST in patients with ESS. Data regarding the included studies are shown in Tables 3a and b.
(a) Oncological outcomes of studies reporting FST for ESS.

Disaggregated data were not available.
AWD, alive with disease; BMI, body mass index; CBDCA, carboplatin; CS, cesarean section; CT, chemotherapy; DOD, died of disease; ESS, endometrial stromal sarcoma; FS, fertility-sparing; FSS, fertility-sparing surgery; GnRHa, gonadotropin-releasing hormone agonist; HR, hysteroscopic resection; HT, hormonal therapy; LND, lymph node dissection; LNG-IUD, levonorgestrel-releasing intrauterine device; MA, megestrol acetate; MPA, medroxyprogesterone acetate; NED, no evidence of disease; PLND, pelvic lymph node dissection; PTX, paclitaxel; RT, radiotherapy; TAH, total abdominal hysterectomy; THBSO, total hysterectomy with bilateral salpingo-oophorectomy.
(b) Reproductive outcomes of studies reporting FST for ESS.
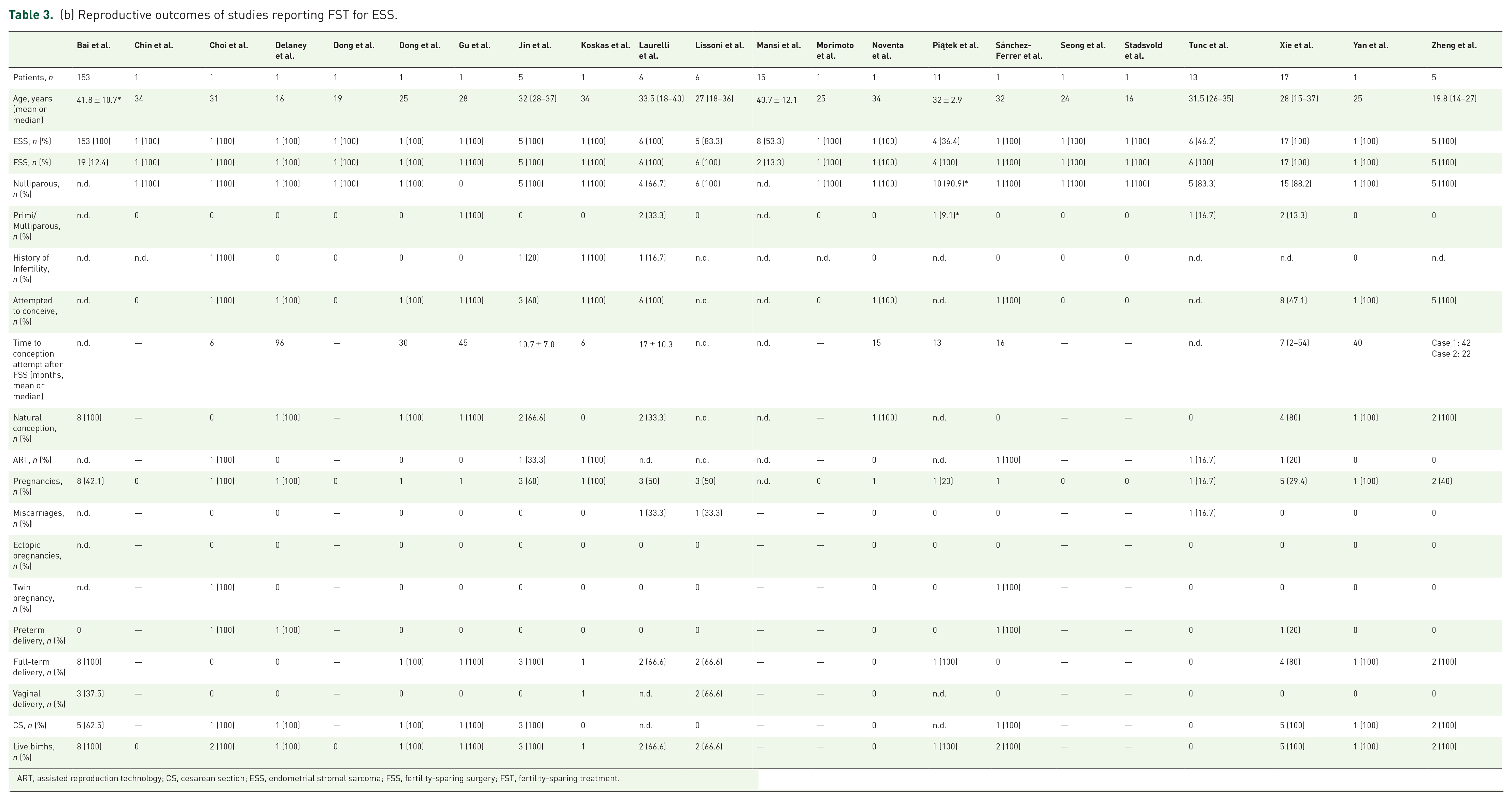
ART, assisted reproduction technology; CS, cesarean section; ESS, endometrial stromal sarcoma; FSS, fertility-sparing surgery; FST, fertility-sparing treatment.
Delaney et al. 38 reported the case of a 16-year-old patient who underwent FST by laparotomic excision of a 17 cm uterine mass. Pathologic examination revealed an LG-ESS. After surgery, the adjuvant regimen involved megestrol acetate (MA) treatment. Eight years later, the patient conceived spontaneously, delivering a late-preterm healthy newborn by cesarean section (CS). Similar results were obtained by Dong et al.,39,40 Gu et al., 42 Lissoni et al., 51 Noventa et al., 57 Piątek et al., 58 Sánchez-Ferrer et al., 62 Yan et al., 71 and Zheng et al. 73 A similar approach was reported also by Seong et al., 63 Stadsvold et al., 66 and Tunc et al., 69 however no pregnancies occurred in their reports.
Bai et al. 31 aimed to assess the optimal management for LG-ESS in one of the study with the largest sample in literature. One hundred fifty-three patients with a diagnosis of LG-ESS were retrospectively included. Of them, 19 (12.4) underwent an FST approach. Eight full-term live births occurred, of which five were by CS and three by spontaneous delivery. Equivalent results were achieved in the series by Xie et al. 70 and Zheng et al. 73
In four studies ESS underwent a conservative treatment through hysteroscopic resection (HR).36,47,48,52 Choi et al. implemented the FST regimen by adding photodynamic therapy and laparoscopic pelvic lymph node dissection (PLND) to HR 36 ; adjuvant therapy with letrozole 2.5 mg daily was administered. The patient did not develop any recurrence and managed to conceive through assisted reproductive technology (ART) 6 months after the end of the treatment, delivering twin newborns via CS. Comparable findings were obtained by Laurelli et al. 48 and Koskas et al., 47 although in the latter a recurrence occurred after delivery.
Quality of evidence: The evidence regarding the safety, effectiveness, and reliability of FST for the treatment of ESS was classified as evidence level 2b.
Rhabdomyosarcoma
Thirteen studies analyzed oncologic and reproductive outcomes after the FST of RMS. Data regarding the included studies are shown in Tables 4a and b.
(a) Oncological outcomes of studies reporting FST for RMS.

AWD, alive with disease; BMI, body mass index; BLM, bleomycin; CT, chemotherapy; CTX, cyclophosphamide; DDP, cis-platin; ERMS, embryonal rhabdomyosarcoma; DOX, doxorubicin; DTIC, dacarbazine; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; HR, hysteroscopic resection; IFO, ifosfamide; KSM, kengsengmycin; LEEP, loop electrosurgical excision procedure; LTF, lost to follow-up; MESNA, sodium 2-mercaptoethane sulfonate; NACT, neoadjuvant chemotherapy; NED, no evidence of disease; PLND, pelvic lymph node dissection; RHBSO, robotic hysterectomy with bilateral salpingo-oophorectomy; VAC, vincristine, actinomycin D and cyclophosphamide; VCR, vincristine; VIA, VP-16, ifosfamide and cytarabine.
(b) Reproductive outcomes of studies reporting FST for RMS.

ART, assisted reproductive technology; CS, cesarean section; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; RMS, rhabdomyosarcoma.
Moufarrij et al. 55 described the case of a 17-year-old patient who underwent trans-cervical excision of an intrauterine polyp with atypical features which was diagnosed as embryonal rhabdomyosarcoma (ERMS) after definitive pathological analysis. Adjuvant regimen involved chemotherapy (CT) with doxorubicin (DOX), dacarbazine, cyclophosphamide, and vincristine for three courses. The patient showed a complete response (CR), and 96 months after the treatment conceived naturally and achieved a full-term uncomplicated delivery. Similar outcomes were obtained by Ayas, 30 Sobiczewski et al., 65 and Piątek et al. 58
In the series by Ricciardi et al., 59 5 out of 15 patients diagnosed with RMS were treated conservatively with local excision of the neoplasm. Adjuvant CT regimen with DOX + ifosfamide (IFO) was administered to two patients (40%). Twi recurrences occurred (40%), one of whom was treated by THBSO. All five patients showed NED at the last follow-up (median 186 months, range 23–282). One ongoing pregnancy was described (20%), but no live births occurred. A similar rate of recurrences was reported within the dataset from Dehner et al., 37 including 14 patients with ERMS.
A positive oncologic outcome was achieved in the experience of Bell et al., 32 Bouchard-Fortier et al., 33 Buruiana et al., 34 John et al., 46 Li et al., 50 May et al., 53 and Strahl et al., 67 with a CR after FST with trans-cervical resection or radical trachelectomy and subsequent adjuvant treatment with different CT protocols. However, these authors did not reported any pregnancies.
Quality of evidence: The evidence regarding the safety, effectiveness, and reliability of FST for the treatment of RMS was classified as evidence level 2b.
Adenosarcoma
In five of the included studies, a FST approach was employed for the treatment of AS. Data regarding the included studies are shown in Tables 5a and b.
(a) Oncological outcomes of studies reporting FST for AS.

AWD, alive with disease; AS, adenosarcoma; BMI, body mass index; CT, chemotherapy; DDP, cis-platin; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; HR, hysteroscopic resection; IFO, ifosfamide; MA, megestrol acetate; MPA, medroxyprogesterone acetate; NED, no evidence of disease; PLND, pelvic lymph node dissection; THBS, total hysterectomy with bilateral salpingectomy; THBSO, total hysterectomy with bilateral salpingo-oophorectomy.
(b) Reproductive outcomes of studies reporting FST for AS.

ART, assisted reproductive technology; AS, adenosarcoma; CS, cesarean section; FSS, fertility-sparing surgery; FST, fertility-sparing treatment.
The neoplasms were excised in almost all cases through HR. In the series by Lee et al., 49 7 (22.6%) out of 31 patients with AS underwent FST. Adjuvant therapy was started in two patients (28.6); one patient started an oral progestin regimen with medroxyprogesterone acetate; the other patient underwent CT with IFO + cis-platin. Recurrences occurred in two patients; one of them underwent radical debulking surgery, the other one refused surgery. Two patients showed a persistent disease (PD) after FST. One live birth (14.3%) occurred in the series. A similar approach led to slightly better oncologic outcomes in the study by Yuan et al. 72
Zizolfi et al. 74 reported the case of a 23-year-old patient conservatively treated with HR for AS. An adjuvant regimen with MA 160 mg daily was started after surgery. The patient achieved a CR and conceived spontaneously 51 months after FST. In the end, a healthy newborn was delivered through a full-term vaginal birth.
A similar case was reported by Goh et al. 41 ; however, 96 months after the delivery, a recurrence occurred, and patient underwent THBSO + PLND. Piątek et al. 58 successfully treated three patients with AS through hysteroscopic or abdominal resection of the mass. No patient recurred, showing no evidence of disease (NED; mean follow-up time was 46 ± 22.6 months). No pregnancies occurred, as in the case report by Togami et al. 68
Quality of evidence: The evidence regarding the safety, effectiveness, and reliability of FST for the treatment of AS was classified as evidence level 2b.
Low-grade myofibroblastic sarcoma
One patient in the cohort analyzed by Piątek et al. 58 underwent a FST for LGMS. Reproductive and oncologic outcomes were further summarized in Tables 6a and b. The patient managed to deliver two healthy newborns, respectively 12 and 34 months after surgery. However, 90 months after surgery, a recurrence was diagnosed, and the patient underwent THBSO.
(a) Oncological outcomes of studies reporting FST for LGMS.

BMI, body mass index; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; LGMS, low-grade myofibroblastic sarcoma; NED, no evidence of disease; THBSO, total hysterectomy with bilateral salpingo-oophorectomy.
(b) Reproductive outcomes of studies reporting FST for LGMS.

ART, assisted reproductive technology; CS, cesarean section; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; LGMS, low-grade myofibroblastic sarcoma.
Quality of evidence: The evidence regarding the safety, effectiveness, and reliability of FST for the treatment of LGMS was classified as evidence level 4.
Uterine smooth muscle tumors of uncertain malignant potential
Six studies evaluated the outcomes after FST for STUMP. Data regarding the included studies are shown in Tables 7a and b.
(a) Oncological outcomes of studies reporting FST for STUMP.

AWD, alive with disease; BMI, body mass index; CT, chemotherapy; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; HR, hysteroscopic resection; LND, lymph node dissection; NED, no evidence of disease; STUMP, uterine smooth muscle tumors of uncertain malignant potential; TAH, total abdominal hysterectomy; TAHBSO, total abdominal hysterectomy with bilateral salpingo-oophorectomy; THBS, total hysterectomy with bilateral salpingectomy; TLVHBS, total laparoscopic vaginal hysterectomy with bilateral salpingectomy.
(b) Reproductive outcomes of studies reporting FST for STUMP.

ART, assisted reproductive technology; CS, cesarean section; FSS, fertility-sparing surgery; FST, fertility-sparing treatment; STUMP, uterine smooth muscle tumors of uncertain malignant potential; TOP, termination of pregnancy.
In the series by Richtarova et al., 60 46 patients with STUMP underwent FST through laparotomic, laparoscopic, vaginal, or hysteroscopic approaches. Seven recurrences took place (15.2%), all of which were treated by total hysterectomy with bilateral salpingectomy. All the 46 patients showed an NED after follow-up (median 30, range 7–149). Twenty-two pregnancies were obtained (47.8%) among 17 patients, hesitated in 2 miscarriages (9.1%), 2 termination of pregnancy (TOP; 9.1%), and 18 live births (81.8%). Comparable outcomes were obtained by Ha et al., 43 Huo et al., 44 Ning et al., 56 Sahin et al, 61 and Shim et al. 64 Overall, 47 live births from 175 patients who underwent FST for STUMP were reported.
Quality of evidence: The evidence regarding the safety, effectiveness, and reliability of FST for the treatment of STUMP was classified as evidence level 2b.
Discussion
Through this systematic review, we synthesized the existing evidence with the aim to highlight the complexities surrounding fertility preservation and oncologic safety in this patient population. US represent a heterogeneous group of neoplasms united by the same mesenchymal origin but with substantial differences in terms of prognosis and treatment. 75
As previously mentioned, the preoperative diagnosis of US remains complex and challenging. Since symptoms lack specificity, the majority of cases are identified incidentally following hysterectomy or fibroid morcellation. 76 Common clinical presentations include abnormal vaginal bleeding and an enlarging or rapidly growing uterus. 11 Any instances of rapid uterine growth in post-menopausal women or abnormal vaginal bleeding should prompt a rapid assessment. Unfortunately, the utility of endometrial sampling is restricted; the sensitivity of endometrial biopsy in diagnosing LMS is low, as it can detect the preoperative neoplasm in only half of the cases, 77 even in competent hysteroscopists who have received appropriate training. 78 The cornerstone of US treatment is represented by THBSO, 1 although radical surgery significantly affects fertility; the only option available for women desiring fertility who have undergone radical hysterectomy is uterine transplantation, which, however, is still far from being considered a standardized procedure. 79
LMS constitutes the predominant subtype of US, accounting for approximately 80% of all the group of neoplasms. 80 An analysis of the SEER database, covering patients diagnosed with US from 2000 to 2012, revealed that in those with LMS, 50% were identified at stage I, while 14% presented at stage II or III, and 31% were diagnosed with stage IV disease. 81 Surgical excision through total abdominal hysterectomy remains the primary treatment approach for LMS restricted to the uterus or localized within the pelvis.14 –16 In premenopausal women with early-stage disease (stage I or II), numerous studies have indicated that preserving the ovaries does not adversely affect overall survival (OS) or recurrence rates, 82 despite theoretical considerations suggesting that certain LMS may express estrogen receptors, potentially leading to hormonal responsiveness. 83
In the most extensive study comprising 1396 LMS patients, the 5-year disease-free survival (DFS) rate stood at 65.7% for the entire group. 84 The 5-year disease-specific survival (DSS) rates for stage I, II, III, and IV patients were 75.8%, 60.1%, 44.9%, and 28.7%, respectively. Various factors such as age, race, stage, grade, and primary surgery were identified as independent predictors of DSS in uterine LMS patients. However, oophorectomy did not demonstrate an independent effect on survival outcomes. 84 Nevertheless, FST may be associated with worsened oncologic outcomes. In the present systematic review, two studies involving nine patients who underwent FST of LMS were included.58,69 At the last follow-up, only one patient showed NED (11.1%), three patients were reported to be alive, without specifying if NED or alive with disease (AWD; 33.3%), three patients were AWD (33.3%), and four patients DOD (44.4%). Three pregnancies occurred (33.3%), hesitated in three live births. According to the results of this review, and in view of the important bias due to the small number of patients compared with other US histotypes, LMS represents the neoplasm most susceptible to recurrence, so FST may not be safe in these settings.
LG-ESS is the second most common malignant mesenchymal tumor after LMS, representing 6%–20% of all US but less than 1% of all uterine malignancies. 85 The recent classification by the WHO for tumors affecting the female reproductive system categorizes these growths into four separate groups: endometrial stromal nodule, LG-ESS, high-grade endometrial stromal sarcoma, and UUS. 8 Roughly 70% of individuals receive their diagnosis during the early stages (I–II), with stage being a crucial determinant of prognosis. 86 In contrast to other types of US, LG-ESS tends to affect individuals of a younger age and demonstrates a slow-progressing nature. For those in the early stages, the 5-year DFS rate exceeds 90%. 86 Overall, the 5-year and 10-year DSS rates range from 80% to 90% and 70%, respectively; however, there is an overall recurrence risk of up to 50%. 80 Twenty-two studies regarding FST of ESS were included in the present qualitative analysis. FS (fertility-sparing) surgical approach involves in most cases abdominal or hysteroscopic excision. Eighty-three patients underwent an FST; of them, 54 (64.3%) showed NED, 7 (8.4%) were AWD, and 3 patients (3.6%) were DOD. No data regarding alive patients were reported in the series by Bai et al. 31 Forty-six recurrences occurred in total (55.4%). Regarding the reproductive outcomes, 35 pregnancies were reported by the included studies, with 3 miscarriages and 32 live births.
RMS is a malignancy known for its aggressiveness and predominantly affects children and younger individuals. 87 However, it is exceptionally uncommon in adults, comprising approximately 3% of all cases of soft tissue sarcoma in this age group. 88 The classification system established by the WHO for RMS identifies four subtypes: ERMS, alveolar RMS (ARMS), pleomorphic RMS (PRMS), and spindle cell/sclerosing RMS (SRMS). 8 Sarcoma botryoides represent the predominant subtype among ERMS. 89 ERMS commonly manifests in the vagina during the initial 10 years of life, typically with an average age of onset at 3 years, while cervical RMS are notably more prevalent than those originating from the uterine corpus. 87 A systematic review complemented by pooled analysis did not reveal any adverse effects of FST on the 5-year OS among patients diagnosed with RMS compared to radical surgery. 90 The 5-year OS rates were 79% for radical surgery and 90% for conservative surgery, with no statistically significant difference noted (p = 0.229). Thirteen studies in this systematic review evaluated the outcome after FST of RMS in 36 patients, with 28 NED (77.8%), 3 AWD (8.3%), and 3 LTF (8.3%). No data were reported about follow-up in one study. 50 In most cases, the neoplasms were originating from the cervix. Among these patients, six pregnancies were reported, with one ongoing pregnancy (16.7%) and five live births (83.3%)
Uterine AS is a neoplasm characterized by a biphasic nature, comprising a benign or sometimes atypical glandular element alongside a malignant stromal component, accounting approximately for 5%–10% of US. 91 AS at stage I, lacking sarcomatous overgrowth, shows a relatively favorable prognosis with a 5-year OS rate reaching up to 80%. 91 Five studies within the encompassed studies assessed the oncologic and reproductive outcomes after FST for AS. Twenty-two patients were treated conservatively, with 17 showing NED (77.3%), 3 AWD (13.6%), and 3 patients showing PD after treatment (13.6%). Four pregnancies were reported among the treated patients in the various studies, all of which hesitated in live births.
Finally, according to the 2014 WHO definition, STUMP is defined as smooth muscle tumors exhibiting characteristics that prevent a definitive diagnosis of LMS, yet they do not meet the criteria for leiomyoma or its variations. 92 This raises suspicion regarding potential malignant behavior, and only clinical outcomes can ascertain its benign or malignant nature. STUMP represents a less common category of uterine smooth muscle tumors with intermediate morphological features, making classification challenging. In fact, diagnosing leiomyoma, STUMP, or LMS can be challenging due to similar symptoms like menstrual irregularities and pelvic masses. Moreover, postoperative histological diagnosis of STUMP is complicated by the absence of standardized diagnostic criteria. The diagnostic criteria currently most used are based on the studies by Bell et al.92,93 STUMP is an exceptionally rare condition, found in 0.01% of women undergoing surgery with a suspected diagnosis of uterine leiomyoma, 94 and generally occurs in women of reproductive age. 95 The 5-year OS rate reported in literature ranges between 92% and 100%. 96 In six of the included studies a FST approach was employed for the treatment of STUMP, involving 175 patients. Oncologic outcomes were proficient, with 157 patients showing NED at the last follow-up (89.7%). Twenty-six recurrences occurred (14.9%). Fifty-eight pregnancies occurred across all the studies, with 4 miscarriages, 2 TOP, 5 ongoing pregnancies, and 47 live births.
Another significant aspect concerning US pertains to the potential for occult occurrences identified during surgery intended for presumed benign fibroids. In parallel, controversy arose from the introduction of minimally invasive surgical techniques. With the increasing preference for minimally invasive procedures like laparoscopic and robotic surgery for hysterectomy or myomectomy since the mid-2000s, there has been a concurrent escalation in the use of morcellation for tissue extraction.97,98 Furthermore, the implementation of operative endoscopy has enabled better feasibility of hysteroscopic myomectomies, even for fibroids previously considered less operable with this technique, such as G3 fibroids, 99 often linked to infertility.100,101 Nevertheless, in 2014 The Food and Drug Administration released a statement advising against the utilization of these devices due to safety apprehensions, primarily concerning the unintentional spread of hidden uterine cancer in individuals undergoing hysterectomy and myomectomy for presumed benign leiomyomas. 102 Nonetheless, a meta-analysis conducted by Pritts et al., 103 which encompassed 133 studies, revealed that the estimated incidence rate of LMS stood at 0.51 per 1000 procedures (with a 95% credible interval (CrI) of 0.16–0.98), translating to approximately 1 case in 2000 surgeries. By restricting the meta-analysis to the 64 prospective studies, the meta-analysis yielded a notably lower estimation of 0.12 LMSs per 1000 procedures (with a 95% CrI ranging from <0.01 to 0.75) or approximately one case of LMS per 8300 surgeries. 103
Limitations
This systematic review is subject to several limitations. Firstly, the absence of randomized controlled trials on the topic limits the ability to draw definitive conclusions regarding the reproductive and oncologic outcomes in young women undergoing FST for uterine STUMP and sarcomas. Additionally, the lack of prospective studies contributes to the challenge of establishing robust evidence in this area.
Furthermore, the heterogeneous nature of US, encompassing various histological subtypes with very different prognoses and treatment strategies, presents a significant limitation. The lack of standardized approaches for classifying and treating these tumors adds complexity to the interpretation of the available data. In addition, the unrepresentative number of patients of some histotypes, such as LMS and LGMS, does not allow solid conclusions to be drawn; in fact, although high pregnancy rates have been reported, it is also true that recurrence rates are the highest among the groups. Although the data for this type of US are not significant, this would still dictate that even more attention should be paid. Despite these limitations, this systematic review is, to the best of our knowledge, the largest to date in the literature and provides valuable insights into the current understanding of reproductive and oncologic outcomes in young women with US undergoing FST.
Conclusion
FST is a possible and already widely used option for gynecologic cancers. Despite the large number of articles included in this qualitative analysis, the high heterogeneity of histologic types of US and FST implemented does not allow us to make a definitive judgment. However, our results may suggest that FST might be a possible treatment option for young women with US who have not yet realized their reproductive desire after carefully considering the risk-benefit ratio involved in each histotype of US. These patients should be referred to high-volume centers for gynecologic malignancies and taken care of by a multidisciplinary team. They should also receive appropriate counseling to make them aware of the concrete high risk of recurrence and the need for radical surgery once their desire for parenthood is fulfilled. The eventual achievement of pregnancy may be more difficult for some histotypes than others. In case of delay in achieving pregnancy, ART should be the way forward. Future research efforts should focus on conducting well-designed prospective studies and clinical trials to address these knowledge gaps and enhance clinical decision-making in this population.
Supplemental Material
sj-docx-1-reh-10.1177_26334941241271563 – Supplemental material for Reproductive and oncologic outcomes in young women with uterine sarcoma undergoing fertility-sparing treatment: a systematic review
Supplemental material, sj-docx-1-reh-10.1177_26334941241271563 for Reproductive and oncologic outcomes in young women with uterine sarcoma undergoing fertility-sparing treatment: a systematic review by Andrea Etrusco, Vittorio Agrifoglio, Antonio Simone Laganà, Elko Gliozheni, Annamaria Caringella, Antonio Stanziano, Ettore Cicinelli, Vito Chiantera, Andrea Giannini, Baydaa Alsannan, Fabio Barra and Antonio D’Amato in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941241271563 – Supplemental material for Reproductive and oncologic outcomes in young women with uterine sarcoma undergoing fertility-sparing treatment: a systematic review
Supplemental material, sj-docx-2-reh-10.1177_26334941241271563 for Reproductive and oncologic outcomes in young women with uterine sarcoma undergoing fertility-sparing treatment: a systematic review by Andrea Etrusco, Vittorio Agrifoglio, Antonio Simone Laganà, Elko Gliozheni, Annamaria Caringella, Antonio Stanziano, Ettore Cicinelli, Vito Chiantera, Andrea Giannini, Baydaa Alsannan, Fabio Barra and Antonio D’Amato in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.