
Abstract
Background:
Cervical cancer is one of the most common causes of cancer-related morbidity and mortality globally. In developed countries, effective screening programs reduced its burden. However, in Ethiopia, cervical cancer remains a major public health problem despite the screening service being available free of charge.
Objective:
The aim of this study was to assess women’s willingness for cervical cancer screening services and associated factors among women attending health services in Addis Ababa, Ethiopia.
Design:
An institutional-based, analytic, cross-sectional study was conducted among sexually active women attending health facilities from August to September 2022.
Methods:
A pretested interviewer-administered questionnaire was used for data collection. Data were analyzed using SPSS version 25. Logistic regression was used to determine different variables’ frequencies and associated factors. A p value of <0.05 was considered statistically significant.
Result:
Four hundred twenty-two women were approached, and 394 (93.4%) met the study inclusion criteria. Study participants had a minimum of 1 and a maximum of 6 sexual partners in their lives. A total of 256 (64.9%) study participants had heard about cervical cancer. Among those who heard about cervical cancer, only 22 (8.6%) had been tested for cervical cancer. Of those who did not receive cervical cancer screening, only 175 (47.0%) are willing to receive cervical cancer screening. Age, religion, marital status, place of residence, educational level, occupation, and hearing about cervical cancer were found to be statistically significant. Women who heard about cervical cancer were 15.2 times more likely to take the test compared to those who never heard about cervical cancer before the study.
Conclusion:
Women’s willingness to be screened for cervical cancer is low despite many of the study participants having more than one partner in their lives and being at risk for cervical cancer. Only a few participants had been screened for cervical cancer. Women who had heard about cervical cancer were more likely to take the screening service compared to those who had never heard it before. This highlights the need to prioritize raising awareness about the benefits of cervical cancer screening services.
Introduction
Cervical cancer (CC) is the fourth most common type of cancer among women globally, with 604,127 cases reported in 2020. Around 90% of the estimated 341,831 deaths occurred in low and middle-income countries. 1 In Ethiopia, CC is also the second leading cause of cancer-related morbidity and mortality. 2 In 2020, there were 7445 diagnosed cases and 5338 deaths due to cervical cancer. The risk of cervical cancer among women aged 15 years and older in Ethiopia is estimated to be 33.7 million. 2 The Addis Ababa cancer registry indicates that cervical cancer is the second most common cancer among women, following breast cancer. 3
The prevalence of cervical cancer among women undergoing screening at the Addis Ababa CC screening center was found to be 23.5%. 4 Factors associated with cervical cancer were multiple sexual partners, Human Immune Deficiency Virus positivity, a history of sexually transmitted infection, and the early beginning of sexual intercourse. 4 In another study conducted at Tikur Anbessa Specialized Referral Hospital in Ethiopia revealed that almost one-third of the study participants had CC, and the clinical stages of the disease at the beginning of therapy were stage IIa. 5
Despite its prevalence until recently, CC has yet to be addressed as a significant public health problem at any level of the health care system in Ethiopia. There was no comprehensive program in place to prevent, educate, screen, or provide curative care. Furthermore, cancer detection for treatment was too late, and the health care system was lacking in terms of hospice care and other palliative care alternatives. 6 Scaling up cancer screening and treatment for pre-invasive and invasive CC is one of the global strategies of the World Health Organization to reduce CC mortality. 7
Visual inspection of the cervix with acetic acid wash (VIA) is a safe, acceptable, feasible, effective, and readily available method of CC screening for low and middle-income countries.8–10 Evidence showed that countries with effective CC screening programs and human papillomavirus vaccination decreased the incidence of CC mortality rate. 11
Currently, the Ethiopian Federal Ministry of Health (EFMoH) has developed the CC prevention and control guideline and has expanded the CC prevention and control program at the national level 12 as early screening and detection can prevent the disease. VIA is available in most government health institutions. However, women’s utilization of CC screening in different regions of Ethiopia remains still very low at 4%, 5.4%,7.3%, 8.7%, and 14.1% in Dire Dawa, Debremarkos, Ilu Abba Bor, Ambo, and Gojam respectively.13–17
Studies in various countries indicate that the factors associated with willingness to screen for CC among sexually active women were education level, knowledge of the disease of CC and awareness of the CC screening service, fear of screening, cultural beliefs, and availability of the screening service.18–20
Despite early cervical cancer screening plays a crucial role in reducing the burden of the disease as it allows for timely intervention and treatment and also helps to prevent the progression of cervical cancer, many women in Ethiopia managed for maternal and reproductive health services have missed opportunities for CC screening services. 21
This research aimed to evaluate the willingness of women to participate in cervical cancer screening services among women attending health services in Addis Ababa, Ethiopia. Therefore, based on the empirical findings, a recommendation will be provided to the concerned body to improve the use of the cervical cancer screening service for women in Ethiopia.
Methods and materials
Study area and period: The study was carried out in Addis Ababa, Ethiopia. Addis Ababa is the capital city of Ethiopia, which is administratively divided into 11 sub-city, and each sub-city is in turn divided into 99 lower-level administrative units known as ‘woreda’. According to the Central Statistics Agency of the Federal Democratic Republic of Ethiopia for the 2007 Census, the projected population of Addis Ababa in 2021 was 5,006,000. 22 Most of the Addis Ababa sub-city currently has free CC screening services using VIA.
St Paul’s Hospital is one of the largest public hospitals and referral centers in Ethiopia, providing health care services to patients across the country, particularly those from low-income communities who lack access to private health care facilities. It is a pioneer in implementing the cervical cancer prevention program using VIA and serves as a national training center for the program. The hospital has established a strong referral network with 12 public health centers that offer cervical cancer screening. This network allows it to study the willingness of women receiving health care services to undergo cervical cancer screening. Additionally, St Paul hospital actively engaged in academic and research activities alongside its medical services.
The study was conducted mainly at St Paul’s Hospital and three randomly selected referral networked health centers (Selam, Kolfe, and Felege Meles Health centers) in Addis Ababa, Ethiopia. The data collection period for the study was from August 1 to September 30, 2022
Study design: Institutional-based cross-sectional study design was used.
Source population: The source population was all women who attended the women’s health services clinic at St Paul’s Hospital and its referral health networks in Addis Ababa, Ethiopia.
Study population: All sexually active women 18 years and older who attended the women’s health services clinic in St Paul’s Hospital and its selected referral health network (Health Centers) from 1 August to 30 September 2022, were included. Women who had been diagnosed with CC were excluded because their willingness to undergo CC screening is considered not applicable to them. The reporting of this study conforms to the strengthening of the reporting of observational studies in Epidemiology (STROBE) statement. 23
Sample size and sampling technique: The sample size was calculated using the single population proportion formula based on the following assumptions.
The level of significance was taken at 95% (Zα/2 = 1.96), and the margin of error was 5%. To the knowledge of the researchers, except for women living with HIV/AIDS and women who receive family planning, the proportion of women who are willing to test for CC in Addis Ababa, Ethiopia, is unknown. To obtain the target sample size, an estimate of 50% was taken, and a 10% non-response rate was considered.

Where:
P = Willingness to screen for CC 50%
d = the margin of error between the sample and the population, 0.05
Zα/2 = critical value at a 95% confidence level of certainty (1.96)
The calculated sample size = 384, 10% non-response rate = 38
The required sample size was 384 + 38 = 422.
Sampling procedure: St Paul Hospital and three health centers were randomly selected from 12 health centers that provided women’s health services and cervical cancer screening services regularly during the data collection period.
The total sample size was allocated to each selected health facility proportionally to the average monthly client flow by reviewing the registration books. Currently, the estimated number of women attending the outpatient women’s health clinic in each hospital and health center is an average of 1000–2000 per month and 300–600, respectively. So, the sample size was divided into hospitals and health centers according to their size (patient flow). A consecutive series of women who received women’s health services at the hospital and its referral network health centers and who met the inclusion criteria were included in the study until the calculated sample size was obtained.
Variables of the study
Dependent variable: Willingness of women to be screened for CC.
Independent variables: Socio-demographic characteristics, sexual and reproductive history, awareness of CC and its detection, CC screening history, and reasons for not utilizing CC screening in the future.
Data collection procedures: To have the appropriate instrument, after an extensive review of the published literature, standard tools were adapted from Refs. 19, 24, 25, 26. The questionnaire was first translated from English into the local language (Amharic) and then retranslated into English by a linguistic graduate to ensure its consistency. The discussion was made by a group of health professionals (obstetrics gynecologists, oncologists, and nurses) on the survey instrument in detail to relate it to the local context and make it easily understandable to the respondents.
Furthermore, the questionnaire was pretested in 5% of the total sample size 27 in another health institution (Ras Desta Damtew Memorial Hospital). Cronbach’s alpha was also used for the reliability (internal consistency) of the tool.
Eight female BSc nurse data collectors and two supervisors were recruited for data collection considering different units of women’s health service in the hospital and health centers (Medical, Surgical, Gyn/OBS, Ophthalmic, ENT, Dental, and Pediatric units).
Training was provided on the purpose of the study and the methods of administering the questionnaire to data collectors and supervisors before the beginning of actual data collection. Data collection tools contain variables related to the socio-demographic characteristics of study participants, sexual and reproductive history, the awareness, utilization, and willingness of study participants to be screened for CC, and factors associated with willingness to be screened for CC. Data were collected using a structured questionnaire administered by a data collector based on the arrival order/consecutive series/ of women attending health institutions for women’s health services. An exit interview was conducted in a separate room after the client had obtained the service for which she came to the institution until the calculated sample size was achieved.
Operational definitions and terms
Willingness to screening for CC refers to a woman willing to be screened or tested for CC in the future by asking the question. Are you willing to be screened for CC? If a woman replied yes, she was considered willing. Otherwise, she was considered not willing.24,26
Women’s health service: Health facilities/units/providing health services for women. Examples: Medical, Surgical, GYN/OBS (family planning, antenatal, postnatal, vaccination), Dental, ENT, Ophthalmic, and Pediatric units.
Data quality assurance: The quality of the data was ensured through the complete evaluation of experts and the pretest of the questionnaire. Proper training of data collectors and supervisors, close supervision of the data collection process, and proper categorization and coding of the data were used. The completeness and accuracy of the collected data were verified daily. Data cleaning and verification were also performed before analysis.
Data analysis: Data were entered into SPSS (Statistical package for the Social Science) version 25 statistical software packages for data analysis. SPSS version 25 is a widely used tool for data analysis, visualization and statistical modeling in different fields including social sciences, education, health care and business. Descriptive statistics like mean, standard deviation, and frequency analysis of the different variables were performed to describe the characteristics of the participants and estimate their willingness to be screened for CC. Logistic regression was used to determine associated factors with willingness to undergo CC screening.
First, a simple logistic regression was fitted for each of the independent variables to select potential factors for the multiple binary logistic regression. Factors with a p value ⩽0.20 were considered for the multiple logistic regression. Finally, a multiple logistic regression that takes into account the binary nature of the outcome of interest and that can control confounding factors was used to identify factors associated with willingness to undergo CC screening. The adjusted odds ratio with a 95% confidence interval was used to assess the magnitude and precision of the association. A p value of <0.05 was considered statistically significant. The findings were presented using text, tables, and graphs.
Result
Demographic and socio-economic background of study participants
A total of 422 women were approached, and 394 (93.4%) of them met the study inclusion criteria, resulting in a response rate that was lower than the assumed non-response rate of 10%.
The study participants had a median age (interquartile range) of 33.0 (26.0–43.0) years, with a range of 20.0–66.0 years. A large proportion of the study participants were Orthodox Christians (52.8%) in religion, currently married (70.1%), residents of Addis Ababa (63.7%), attended primary or secondary school (52%), and housewives (40.4%) by occupation (Table 1).
Demographic and socio-economic background of study participants (n = 394).

Sexual and reproductive history of study participants
The mean age (standard deviation) at the first sexual intercourse of the study participants was 20.0 (3.5) years, with a minimum of 14.0 and a maximum of 28.0 years. These women had a minimum of 1 and a maximum of 6 sexual partners in their lives, with a median (interquartile range) of 2.0 (1.0–3.0). Furthermore, 260 (67.2%) had children (Figure 1).

Sexual and reproductive history of study participants.
Those women who had children had their first pregnancy at a mean (standard deviation) age of 21.8 (3.8) years, with a minimum of 14.0 and a maximum of 37.0 years. These women had a minimum of 1 and a maximum of 7 children, with a median (interquartile range) of 3.0 (2.0–3.0), and had a minimum of 1 and a maximum of 7 children alive, with a median (interquartile range) of 2.0 (1.0–3.0).
Study participant’s awareness of CC and its screening
A total of 256 (64.9%) study participants had heard about CC, with the media being the primary source of information for 163 (63.7%). Among those who heard about CC, 91 (35.5%) mentioned that CC is a disease that affects only women and 80 (31.3%) did not know about CC besides that it is a disease. Thirty-seven (14.5%) had ever seen a patient with CC, and 14 (37.8%) had a family member with CC. One hundred twenty-two (47.7%) knew the risk factors for CC, with 46 (37.7%) mentioning multiple sexual partners, followed by 34 (27.9%) family history, and 32 (26.2%) began sexual intercourse before the age of 17. Ninety-three (36.3%) did not know any symptoms of CC, while 79 (30.9%) mentioned vaginal discharge as a symptom of CC.
Two hundred forty-seven (96.5%) believe that CC is preventable, with 181 (73.3%) mentioning early screening, followed by 59 (23.9%) mentioning early screening and HPV vaccine as prevention for cervical cancer. HPV stands for Human Papillomavirus. HPV is a group of viruses that can infect the human body and cause a variety of health issue, including cervical cancer which is the leading cause of mortality in women. VILI stands for visual inspection with Lugol’s iodine (VILI). VILI is simple, affordable and effective screening method especially in low- resource countries where access to more advanced screening techniques such as pap smears or HPV testing may be limited. It allows early detection of precancerous or early stage of cervical cancer in women, which enable timely treatment and management to prevent the development of cervical cancer. Two hundred and ten (82.0%) believe that CC is treatable, with 103 (49.0%) mentioning chemotherapy, followed by 71 (33.8%) mentioning chemotherapy, surgery, and radiotherapy as treatment. Two hundred and thirty-one (90.2%) believe that CC is curable. Fifty-three (20.7%) knew of CC tests, with 20 (37.7%) mentioning Pap smear, followed by 18 (34.0) mentioning VIA and VILI as test procedures. Ninety-eight (38.3%) knew where to screen for CC, 58 (59.2%) knew about screening centers near their home, and 16 (16.3%) did not (Table 2).
Study participants’ awareness toward cervical cancer screening.
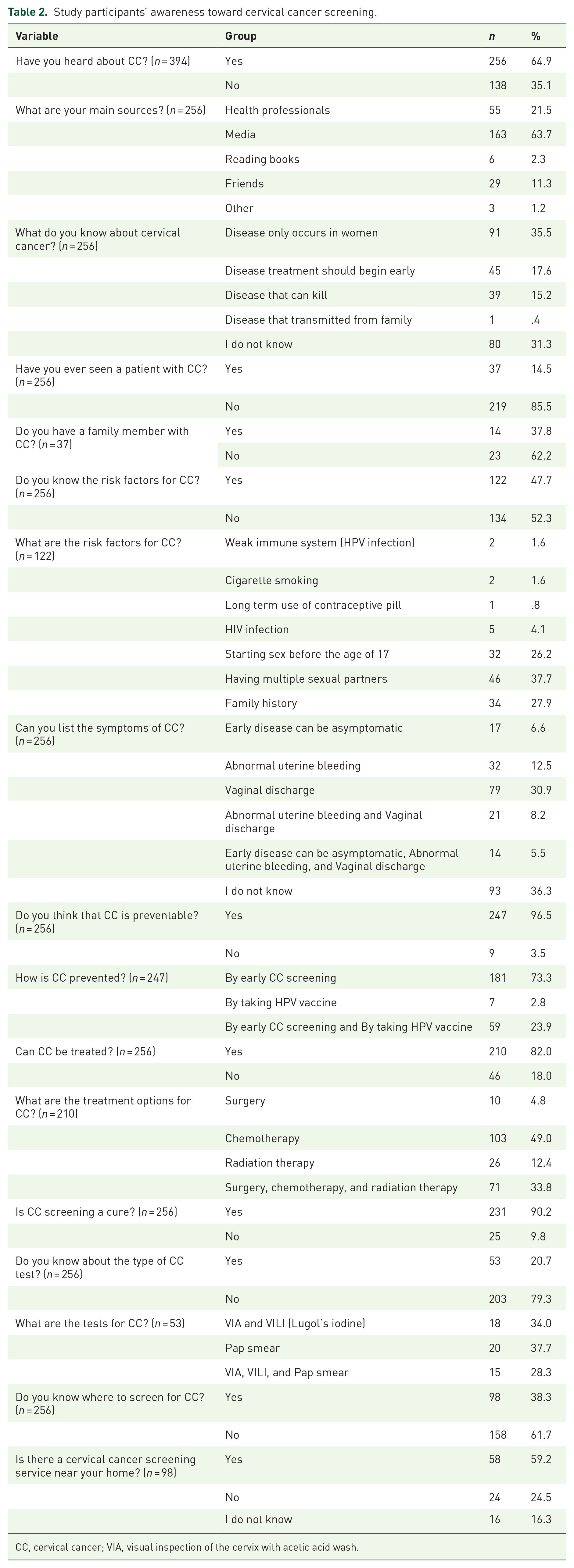
CC, cervical cancer; VIA, visual inspection of the cervix with acetic acid wash.
Cervical cancer screening history
Among those who heard about CC, only 22 (8.6%) had screened for CC, with 19 (86.4%) of them screened in the last 6 months prior to the study, and 21 (95.5%) were screened by either VIA or VLI (Figure 2).

Study participants’ history of cervical cancer screening.
A total of 372 out of the 394 women contacted were not screened for CC. Among those who were not screened for CC, 175 (47.0%) are willing to be screened for CC in the future, with 124 (70.9%) saying they will be screened sometime soon, while 9 (5.1%) are willing to take the test immediately. Of those who were not willing to take the test, 113 (57.4%) reasoned that they either did not have easy access to the test or did not have any reason (Figure 3).

Study participants’ willingness to undergo CC screening in future.
Distribution of willingness for CC screening
A similar proportion of Muslim and Orthodox Christian women were willing to screen for CC, while a large proportion of Protestant and Catholic Christians were not willing. Except for married women, many women, regardless of their marital status, were not willing to undergo a screening. The distribution of willingness is similar to that of the place of residence. A large proportion of women who attended college certificates and diplomas or primary school were willing to be screened. In contrast, many women who attended other levels of education or with no formal education were not willing to screen. Most government employees, students, and merchants were not willing to take the test, while most housewives, private employees, and other employees were willing to take the test (Table 3).
Distribution of the willingness to test for CC screening among study participants demographic and socio-economic characteristics (n = 372).

CC, cervical cancer.
A large proportion of women who had heard about CC were willing to take the test, while many women who had never heard about CC before the study were not willing to take the test (Figure 4).

Distribution of the willingness to test for CC among the sexual and reproductive health characteristics of the study participants.
Factors associated with willingness to undergo CC screening
A binary logistic regression was fitted to assess the factors associated with women’s willingness to take the CC test at some time. All variables considered: age, religion, marital status, place of residence, educational level, occupation, and hearing about CC were found to be statistically significant factors associated with the willingness of women to take the test (p value <0.05).
An increase in age of 1 year is associated with a 12% decrease in the chance of willingness to take the test. Christian women are 5.59 times more likely to be willing to take the test compared to their Muslim counterparts. Current unmarried women were 76% less likely to take the test compared to their married counterparts. Women who reside in Addis Ababa were 61% less likely to take the test than women who reside outside of Addis Ababa. Women without formal education were 88% less likely to take the test relative to women who had attended college or university level education. There is no statistically significant difference between primary and college or university education and between secondary and college or university education. Government employees were 77% less likely to take the test compared to women who had other jobs. There is no statistically significant difference between private employees and government employees, between merchants and government employees, and between housewives and government employees. Those women who have heard about CC are 15.2 times more likely to take the test compared to those who had never heard about CC prior to the study (Table 4).
Factors associated with CC screening willingness among study participants (n = 372).
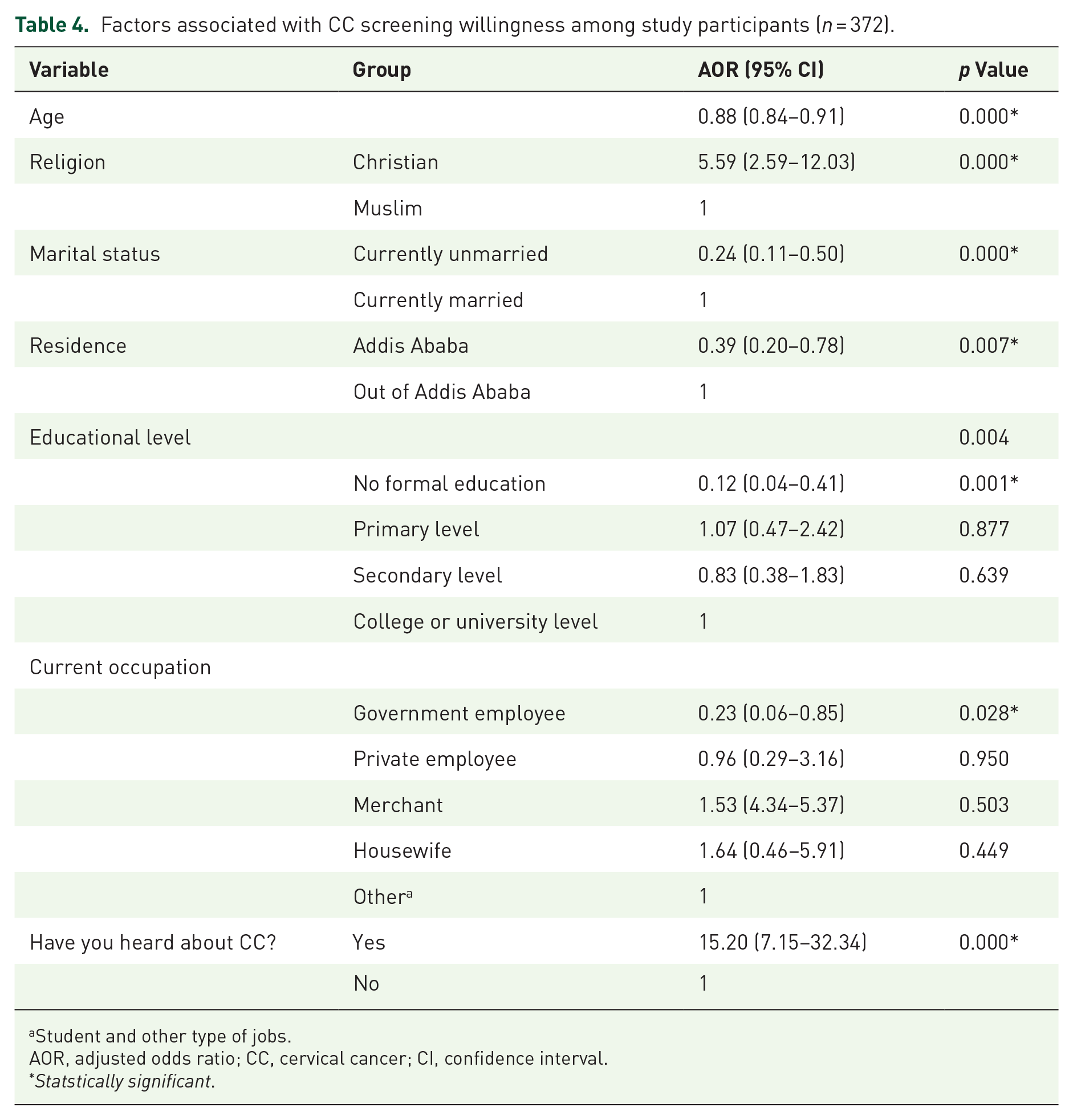
Student and other type of jobs.
AOR, adjusted odds ratio; CC, cervical cancer; CI, confidence interval.
Statstically significant.
Discussion
The willingness to screen for cervical cancer is one of the contributing factors in increasing women’s utilization of the service and thus reducing the burden of morbidity and mortality related to cervical cancer. Currently, the EFMoH and non-government organizations in Ethiopia have been working to expand the CC prevention and control program, as CC has become a public health concern. 28 This study aimed to evaluate the willingness of women to test for cervical cancer and its associated factors among sexually active women attending women’s health services in Addis Ababa, Ethiopia. The finding of this study indicates that the willingness of women to test for CC is low, while the willingness is the primary driver to participate in cervical cancer screening. The willingness of women to test for cervical cancer in the study was associated with education, religion, marital status, place of residence, and hearing about cervical cancer screening. The will to have cervical cancer screening was primarily influenced by hearing about cervical cancer.
Although the study participants had a minimum of 1 and a maximum of 6 sexual partners in their lives, many of the study participants had never heard of the CC screening and were not willing to take the test. Only 256 (64.9%) study participants had heard about CC in the study area, which is almost in line with a study conducted in the South Gondar zone, Ethiopia 66%. 29 On the contrary, the finding of this study was higher than other findings from the study conducted in Nigeria, 12.8%. 30 The difference might be due to the different study settings.
Early detection is one of the mechanisms to overcome the impacts of cervical cancer. However, women’s awareness of early screening could have been higher. Only 87 (38.3%) of the study participants knew where to screen for CC, which is greater than a study conducted in India 34%. 20 The difference might be due to the active participation of cervical cancer prevention programmers in community awareness compared to others.
In the current study among study participants who heard about CC, only 22 (8.6%) were screened for CC, which is less than a study conducted in Tanzania 50.2%, 31 in Saudi Arabia 24.6%, 32 Nigeria 9.4% 33 and North Shoa 21.2%, 26 and is greater than a study conducted in Ambo 6.3%. 34 This difference could be due to the level of community awareness about the service and the strength of the CC screening service units in the study areas.
In addition to the above, the result of the current study is also higher than the studies conducted elsewhere in Ethiopia, including the Arsi zone 7.2% 35 ; Ilu Abba Bor zone, South Western Ethiopia, 7.3% 15 ; and Dire Dawa, Eastern Ethiopia, 4%. 13 This difference could be due to the different educational backgrounds of the study participants and the study setting, as the study is carried out in the capital city of the country, where participants could easily access information about CC screening services than in the countryside.
The prevalence of willingness to test for CC was also low (47.0%), which is consistent with a study conducted in Girar Jarso district, Ethiopia, 46.7%. 26 Less than a study conducted at Jinka General Hospital, Ethiopia, 56.9%. 36 Nigeria at 88.9% 30 and China at 84% 37 , which is also higher than a study conducted in India at 32% 20 and Saudi Arabia at 45%. 32 The variation in the study findings could be due to the different study areas and the difference in the evaluation period.
In the current study, the willingness to test was higher among women who heard about CC. Those women who heard about CC were 15 times more likely to take the test compared to those who had never heard about CC prior to the study, which is similar to a study conducted in Indonesia and India.19,20 A possible reason might be that they will use the screening service when they hear about the screening services provided in health facilities, including the advantages of screening and how the screening service will be performed.
In this study, age, educational level, occupation, religion, marital status, place of residence, and hearing about CC were found to be statistically significant factors associated with the willingness of women to be screened. Women without formal education, housewives, government employees, and women who had never heard about CC before the study were less likely to be screened for CC. This is in line with a study conducted in Tanzania, China, and the Gurage zone in southern Ethiopia.32,37,38 The finding revealed that it is crucial to educate women about CC prevention methods and where to look for early detection and treatment. Continuous education should be established at the community and health institution level using different teaching methods, as an integrated one-stop-shop approach to health services is a comprehensive and safe approach even for those who came for other women’s health services. 11
In this study, Muslim women were less likely to be willing to take the test compared to their Christian counterparts, which is in line with a study conducted in Canada. 39 This might be due to religious beliefs, as many Muslim women believe that ‘becoming ill and dying is the will of Allah and those health problems are a punishment from God’ which could contribute to their lower willingness to participate in cervical cancer screening.
In this study, the willingness of women to take the cervical cancer test is mainly influenced by the awareness of study participants. Different studies support our findings and reveal that the awareness of study participants about the disease and the benefits of the cervical cancer screening service significantly influence their willingness to participate in the cervical cancer screening service.18,19,20,37 This highlights the need to raise women’s awareness about the benefits of using cervical cancer screening services and the availability of a free screening service in the community.
Therefore, the researchers recommend implementing comprehensive educational and awareness programs by engaging religious and community leaders as well as utilizing mass media platforms to spread awareness about cervical cancer screening and the importance of early detection. Implementing these recommendations can enhance women’s willingness to test for cervical cancer, thereby reducing the incidence and mortality rates associated with this preventable disease.
Strengths and limitations of the study
Since the study is cross-sectional, it may not show causal relationships between dependent and independent variables. It can only identify associations. The study focuses on women attending health services in Addis Ababa, which may not be representative of women who do not utilize the health services.
Conclusion
Women’s willingness for cervical cancer screening in the study area is low. Only a few participants had been screened for cervical cancer, despite many of the study participants having more than one partner in their lives and being at risk for cervical cancer.
One-third of the study participants knew where to screen for CC. Among those who were not screened for CC, less than 50% of the study participants are willing to undergo CC screening in the future. Women who had heard about CC were 15.2 times more likely to take the test compared to those who had never heard about CC prior to the study.
As cervical cancer is one of the most common women’s health problems in Ethiopia, the finding in this study highlights the need to raise community awareness about the benefits of cervical cancer screening, the availability of a free screening service, and where to screen using different media.
Supplemental Material
sj-docx-1-reh-10.1177_26334941241253181 – Supplemental material for Women’s willingness for cervical cancer screening and associated factors among women attending health services in Addis Ababa, Ethiopia
Supplemental material, sj-docx-1-reh-10.1177_26334941241253181 for Women’s willingness for cervical cancer screening and associated factors among women attending health services in Addis Ababa, Ethiopia by Tangute Demas, Teshale Biku, Tewodros Getinet, Bereket Fantahun, Delayehu Bekele, Negat Woldehawariat, Rahel Muzemir and Martha Shoarega in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941241253181 – Supplemental material for Women’s willingness for cervical cancer screening and associated factors among women attending health services in Addis Ababa, Ethiopia
Supplemental material, sj-docx-2-reh-10.1177_26334941241253181 for Women’s willingness for cervical cancer screening and associated factors among women attending health services in Addis Ababa, Ethiopia by Tangute Demas, Teshale Biku, Tewodros Getinet, Bereket Fantahun, Delayehu Bekele, Negat Woldehawariat, Rahel Muzemir and Martha Shoarega in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-3-reh-10.1177_26334941241253181 – Supplemental material for Women’s willingness for cervical cancer screening and associated factors among women attending health services in Addis Ababa, Ethiopia
Supplemental material, sj-docx-3-reh-10.1177_26334941241253181 for Women’s willingness for cervical cancer screening and associated factors among women attending health services in Addis Ababa, Ethiopia by Tangute Demas, Teshale Biku, Tewodros Getinet, Bereket Fantahun, Delayehu Bekele, Negat Woldehawariat, Rahel Muzemir and Martha Shoarega in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
The authors thank St Paul Hospital Millennium Medical College and Addis Ababa Health Bureau for supporting this research activity. We also thank women’s health service unit staff, data collectors, supervisors, and study participants.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.