
Abstract
Background:
Reproductive health emergencies, such as postpartum hemorrhage, contribute significantly to maternal and neonatal morbidity and mortality in Uganda due to knowledge and skills gaps. Medical interns, intern midwives, and nurses are crucial as frontline healthcare workers in responding to these emergencies. Our proposed hands-on strategy involves comprehensive simulation-based training (SBT) to equip these healthcare workers with the essential knowledge to manage common reproductive health emergencies and procedures in the country.
Objectives:
The study aimed to assess the effectiveness of comprehensive SBT in improving the knowledge of interns and fifth-year medical students on reproductive health emergencies and procedures at Gulu University and its Teaching Hospitals in Uganda.
Design:
A before-and-after study.
Methods:
A 4-day SBT was conducted for fifth-year medical students and interns (nurses, midwives, and doctors) at Gulu University Teaching Hospitals, focusing on reproductive health emergencies. Pre- and post-tests with 40 multiple-choice questions were used to evaluate knowledge enhancement, the scores were summarized as medians and interquartile ranges. Paired sample t-tests was used to test the difference in pre- and post-test scores. Independent sample t-tests compared median post-test results between interns and students, with a p-value <0.05 considered significant.
Results:
A total of 153 participants were enrolled, the majority being males (78.4%, n = 120) and medical students (73.9%, n = 113). Among the 40 interns, 55% (n = 22) were doctors, 30% (n = 12) were midwives, and 15% (n = 6) were nurses. The study participants showed an increase in knowledge, with median post-test scores higher than pre-test scores for all participants [63% (interquartile ranges, IQR: 57–71%) versus 49% (42–54%), with a median difference of 14% (8–23%), p < 0.001].
Conclusion:
The SBT effectively imparts key knowledge competencies to the interns and fifth-year medical students. We recommend that SBT be included as part of the course units that students should take and for continuous medical education for qualified healthcare workers in resource-limited settings.
Keywords
Introduction
Reproductive health (RH), as an essential part of overall health and well-being, deals with maternal and newborn health and includes high-quality family-planning services, prevention of unsafe abortion, and reproductive tract infections and cancers. 1 Many partners, including the World Health Organization, have put in significant effort to improve the RH since the 1996 Cairo Declaration. 2 Greater effort is required to address RH disorders and emergencies. If not effectively managed, they can pose a threat to the achievement of Sustainable Development Goals 3, 4, and 5.
RH emergencies are related conditions that frequently occur during pregnancy and in the immediate postpartum period 3 and threaten the lives of both the mother and the fetus/newborn baby. 4 These emergencies are normally unpredictable and create an ethical dilemma 5 leading to mismanagement which is common in low-income settings such as Uganda. 6 The probability of an adverse outcome occurring during any RH emergency depends partly on the competencies (knowledge, skills, decision-making, and attitudes) of healthcare providers and the environment (infrastructure, equipment, supplies, leadership, medications, technologies) that are available during the provision of emergency care. 7 A medical worker knowledgeable about RH emergencies is more likely to work faster to save the patients. 8 However, this is not the case in most low-income healthcare settings due to inadequacy of knowledge skills or lack of teamwork. 6
Most errors that result in patients’ adverse outcomes are preventable and the responsibility lies with the medical practitioners. 9 These errors can be minimized if healthcare workers are trained in emergency preparedness through drills, have the requisite knowledge, and are prepared to rapidly identify and take necessary lifesaving actions during suspected or real emergencies. 10 Simulation training has often led to a reduction in the number of avoidable deaths due to medical errors. 11 To bridge the existing gap in the healthcare systems within low-income settings, skilling the frontline healthcare providers through simulation-based training (SBT) might present an opportunity to instill the requisite knowledge, skills, decision-making, and attitudes to manage RH emergencies. 10
Available evidence suggests that SBT improves provider skills, patient safety, and the quality of RH emergency services. In addition, SBT can augment bedside teachings and thus enhance the clinical competence of frontline healthcare providers and undergraduate and postgraduate trainees. 12 Further evidence suggests that SBT can improve communication, decision-making, and team performances. 13
In Uganda, internship training is a mandatory 1-year placement for those in medical, nursing, and midwifery cadres before registering with the Uganda Medical and Dental Practitioners Council and the Uganda Nurses and Midwives Council respectively. To qualify for an internship, one must complete a 5-year and a 4-year training for medical doctors’ nurses and midwives, respectively. For medical interns, medical schools, accredited by Uganda’s National Council of Higher Education, are expected to produce medical doctors capable of handling typical RH emergencies, including procedures such as evacuations, cesarean sections, family-planning methods, as well as managing obstetric hemorrhage, neonatal resuscitations, and infection prevention in RH, among other tasks. The 5-month rotational internship course is an apprenticeship that is expected to build skills, attitudes, and professionalism in each major surgical or medical discipline. Similarly, the critical competencies expected of graduate midwives and nurses in Ugandan include management of RH emergencies such as obstetric hemorrhage, preoperative and postoperative management of cesarean sections, surgical management of incomplete abortions, gynecological surgeries, and neonatal resuscitation. 14
Universities prepare undergraduate midwives, nurses, and doctors through minimally integrated training. In real practice, these professionals work as a team to manage conditions, including emergencies. Minor surgical procedures such as manual vacuum aspirations, family-planning implant insertions and removals, and perineal laceration repairs are task-shifted to graduate nurses or midwives. The course contents of our SBT cater to intern doctors, midwives, and nurses, integrating theories into skills and teaching team management of emergency conditions, procedures, and communication in RH.
The problem faced in some of the internship training centers is the lack of regular supervision leaving interns to manage patients including those with RH emergencies unsupervised. This working condition can easily lead to adverse health outcomes for pregnant women and their unborn babies. Therefore, skilling interns and medical students in their final years through short-term SBT is a promising and sustainable intervention. This study evaluates the short-term effectiveness of SBT on knowledge of RH emergencies among medical interns, intern midwives, nurses, and fifth-year medical students in Uganda.
Methods
Study design and setting
The RH simulation was intended to provide intern doctors, midwives, nurses, and fifth-year medical students with skills and knowledge on major RH emergencies and procedures. The training was implemented through the Gulu University Sexual and Reproductive Health Resource Center (GU-SRHRC) established in 2021 with funding from the Center for International Reproductive Health Training-Africa (CIRHT-Africa). GU-SRHRC established the very first audio-visual simulation laboratory at Gulu University. The simulation laboratory provides low- to medium-fidelity audio-visual simulation. A context-based mini-curriculum was designed to offer training for intern doctors, midwives, nurses, and fifth-year medical students rotating in the Department of Obstetrics and Gynecology. The Template for Intervention Description and Replication (TIDieR) checklist 15 (Supplemental Materials 3) and CONSORT diagram (Figure 1) were used in the design and report of this study respectively.
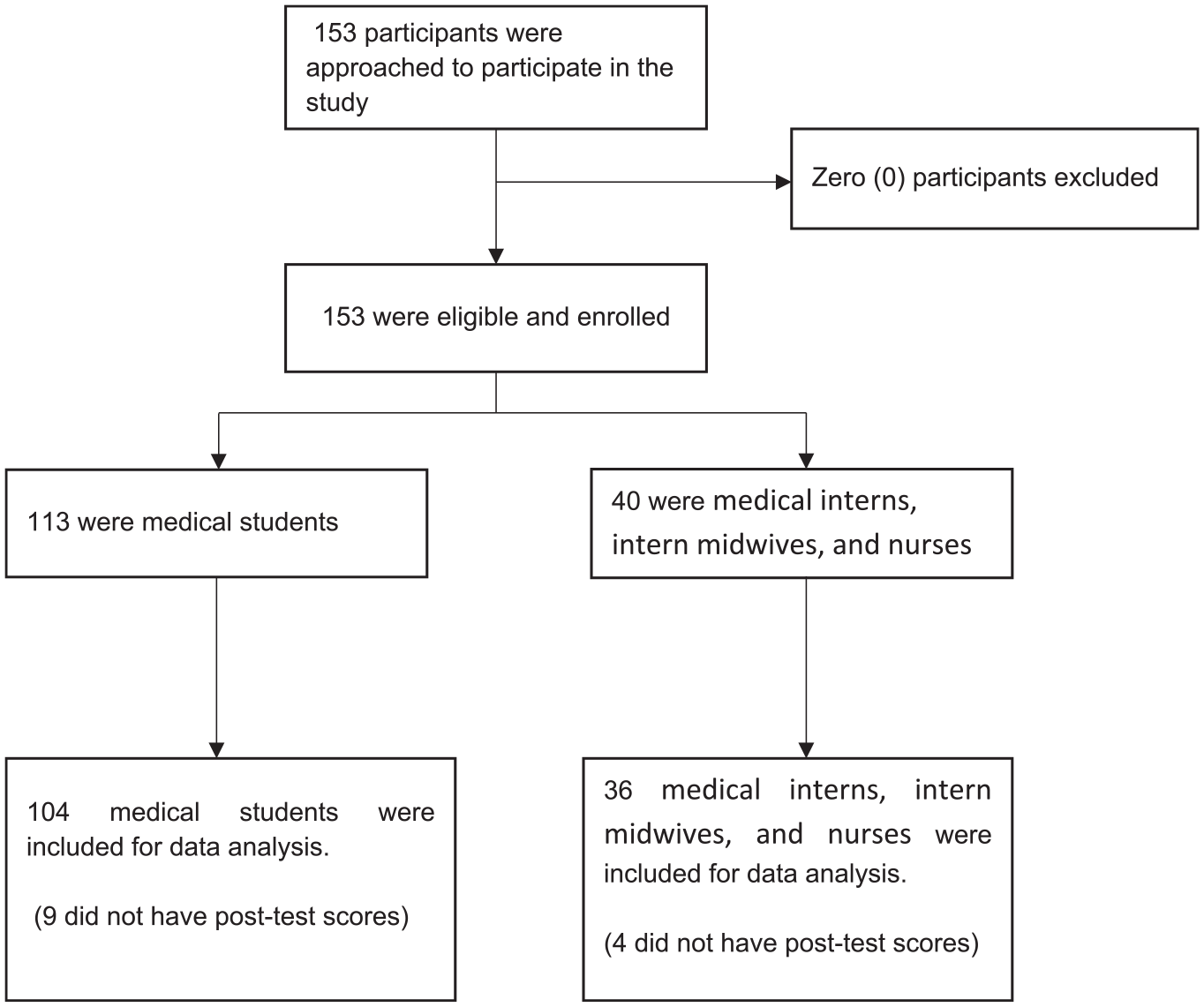
Flow diagram for participants included in the analysis.
Development of training tool
A team of six Obstetricians and Gynecologists in the Department of Obstetrics and Gynecology at Gulu University drafted a curriculum by adopting modules from Essential Surgical Skills used for training year five medical students at Gulu University, and Essential Training in Operative Obstetrics 16 used for training medical officers and postgraduate students by the Associations of Obstetricians and Gynecologists of Uganda (AOGU) and Ministry of Health. Experts in RH at AOGU first reviewed the draft curriculum before it was presented and approved by the Gulu University Faculty of Medicine Board (Supplemental Materials 2) as a training tool for medical interns, intern midwives, nurses, and 5th-year medical students. A team from AOGU conducted a 4-day training of trainers to deliver the approved curriculum. The trained trainers included obstetricians and gynecologists, graduate midwives, pediatricians, general surgeons, and general practitioners who teach and supervise the medical students in clinical rotations and medical interns, intern midwives, and nurses at Gulu University Teaching Hospitals which comprised Gulu Regional Referral Hospital and St. Mary’s Hospital Lacor.
Training
To ensure consistency in content delivery, all trainers, comprising obstetricians and gynecologists, family-planning providers, general surgeons, pediatricians, and general practitioners, underwent a 4-day training on the new curriculum by experts in RH from AOGU. In addition, they were also skilled in adult learning theories. Then, the study participants were offered a 4-day intensive SBT on RH emergencies at the Simulation Laboratory. The training included lectures, small group discussions, demonstrations, role plays, and skills practice. The 4-day training was based on the key principles of adult learning and used interactive learning sessions comprising of short interactive lectures (3 h 45 min of total time), simulation training using low fidelity obstetric, family planning, newborn and resuscitation mannequins, watermelons uterine simulator for manual vacuum aspiration, practices and evaluation (22 h 30 min of the total time) setting ground rules, pre-tests, and post-tests and evaluation, setting ground rules (3 h 45 min of the total time).
The training covered the following areas in RH: (1) introduction to adult learning; (2) communication in RH emergency; (3) infection prevention and control in RH (including proper scrubbing, gowning, gloving, and draping); (4) knotting and suturing techniques; (5) labor and delivery; (6) management of cord prolapses; (7) cesarean section; (8) antepartum and postpartum hemorrhage; (9) early pregnancy bleeding; (10) neonatal resuscitation; (11) perineal tears and fistula; (12) preeclampsia and eclampsia; (13) management of abortion; and (14) provision of family-planning methods.
Training assessment
The knowledge-based assessment tool (The Multiple-Choice Questions) was developed based on the blue-print created from the contents: (1) introduction to adult learning had no question; (2) communication in RH emergency had four questions; (3) infection prevention and control in RH (including proper scrubbing, gowning, gloving, and draping) had no questions since it was practical skills; (4) knotting and suturing techniques had no questions since it was practical skills; (5) labor and delivery had nine questions; (6) management of cord prolapses had no questions since it was practical skills; (7) caesarean section had three questions; (8) antepartum and postpartum hemorrhage had seven questions; (9) early pregnancy bleeding had two questions; (10) neonatal resuscitation had no questions since it was practical skills; (11) perineal tears and fistula had three questions; (12) preeclampsia and eclampsia had four questions; (13) management of abortion one question; and (14) provision of family-planning methods had six questions (Supplemental Materials 1). The pre- and post-tests were administered immediately before and after the training, respectively. The 40 multiple-choice questions used in the pre-and post-tests were the same, giving a like-for-like comparison for each participant tested.
Participants
The participants included fifth-year medical students and medical interns, intern midwives, and nurses at Gulu University Teaching Hospitals. The fifth-year medical interns, intern midwives, and nurses were undergoing clinical rotations in obstetrics and gynecology. The fifth-year were in their final year in medical school. These interns were recent graduates with Bachelor of Medicine and Bachelor of Surgery (medical interns), bachelor’s degrees in nursing (nurses), or bachelor’s degree in midwifery (midwives) respectively. The SBT was provided to them as an approved refresher course at the beginning of their rotation in the Obstetrics and Gynecology departments in the two teaching hospitals.
Data analysis
Raw marks for the pre- and post-tests were computed and converted to percentages. Since the marks were not normally distributed, they were summarized as median with corresponding interquartile ranges (IQR). The pre-tests were done on day one before the onset of the training and post-tests on day 4 at the end of the training. The difference between the pre- and post-training tests was assessed using the paired samples t-test. Independent sample t-tests compared median post-test results between interns and students, with a p-value <0.05 considered significant.
Results
Demographic characteristics
There were 153 participants in the study, the majority were males (78.4%, n = 120), and about one-quarter were interns (26.1%, n = 40), of whom 55% (n = 22) medical doctors, 30% (n = 12) midwives, and 15% (n = 6) nurses. During analysis, we excluded data from 13 (8.5%) participants due to missing outcome data (Figure 1).
Training evaluation
For all participants, there was a notable improvement in percentage knowledge scores from the pre- to post-tests. The median post-test score of 63% (IQR: 57–71%), higher than the pre-test score of 49% (42–54%), with a median difference in score of 14% (8–23%), Table 1, and this was statistically significantly (p < 0.001), Figure 2. For fifth-year participants, the percentage knowledge scores improved from 48% (IQR: 42–53%) pre-training to 63% (57–70.8%) post-training [median difference: 15% (8–23%), p < 0.001], Figure 3. Similarly, the scores of interns improved from 53% (45–58%) on pre-test to 65% (58–73%) at the post-test [median difference: 14% (8–20%), p < 0.001], Figure 4.
Pre- and post-test median knowledge scores of the participants.

IQR, interquartile ranges.

Participants’ scores were stratified by pre- and post-tests.

Before and after plot showing pre- and post-test scores of the fifth year.

Before and after plots showing pre- and post-test scores of the interns.
Discussion
This study aimed to evaluate the impact of SBT on the knowledge of fifth-year medical students and interns (nurses, midwives, and doctors) in Uganda in handling major RH emergencies and procedures shedding light on its importance and potential benefits in low-income settings. Overall, these results suggest that the comprehensive SBT program statistically increases knowledge among medical students and interns in RH emergencies. These findings are comparable with other studies.17,18
It was not surprising that the interns had higher pre-test scores compared to the fifth-year medical students due to their earlier exposure. Similarly, the post-test score was higher among interns although the median range is the same. This could be explained by the diversity in the intern population composed of nurses and midwives who might have different backgrounds in training. Alternatively, the fifth-year medical students could have performed to a level closer to the interns because they expected that this could still be used in the future for examination. This is the basis of an assessment-driven learning model, in which individuals who might face examinations may be more interested in learning a particular content compared to those not hoping to be examined.19 –21 Above all, it explains that this SBT curriculum can be used to train a diverse team of healthcare providers.
The planning for the intern’s training was in such a way that the intern’s nurses, midwives, and doctors are trained together, to help promote team communication that is very pertinent in obstetric emergency management. This is similar to other studies using multidisciplinary teams to build knowledge and team communication. 22 The timing for training was in such a way that students or interns were exposed to simulation training before they rotated in the wards. This has several advantages that address the unique challenges faced by low-income countries in healthcare education. First, it provides a safe and controlled environment for interns as new healthcare professionals to acquire and refine essential clinical skills without compromising patient safety. 23 By simulating realistic skills and team spirit, professionals can practice critical decision-making, communication, and teamwork skills, leading to improved competencies and better patient outcomes. 24
The findings could have important implications for medical education and internship training particularly in resource-limited settings where there may be limited opportunities for hands-on training or supervision. Inconsistent quality and frequency of teaching and supervision are a major barrier in African medical education. 25
Strength and limitation of the study: However, it is important to note that the study has some limitations, including the use of a single institution, which may limit the generalizability of the findings. Although the effectiveness of simulation training for short-term knowledge acquisition among medical students has been widely studied as seen in a review by Mcinerney et al. 26 and thought to build confidence skills among medical students, 27 our study did not assess skills acquisition and long-term impact of the SBT program on the participants’ competencies. Future research could assess the skills and teamwork with the long-term impact of the SBT program on participants.
Despite these limitations, a slightly larger sample size, with diverse trainees including medical students, intern doctors’ nurses, and midwives makes this study a representative starting point to explore more SBT in RH emergencies and procedures.
Conclusion
The results suggest that a comprehensive SBT program could be effective in knowledge promotion for medical students and interns in managing RH emergencies and procedures. The findings describe a single evaluation that should give a foundation for more elaborate research, particularly in resource-limited settings. SBT is therefore recommended to be included as part of the course units that students must undertake.
Supplemental Material
sj-docx-1-reh-10.1177_26334941241251967 – Supplemental material for Efficacy of the Gulu University Reproductive Health Simulation Training for final year medical students and interns: a before-and-after study
Supplemental material, sj-docx-1-reh-10.1177_26334941241251967 for Efficacy of the Gulu University Reproductive Health Simulation Training for final year medical students and interns: a before-and-after study by Pebalo Francis Pebolo, Jerom Okot, Felix Bongomin, Silvia Awor, Baifa Arwinyo, Sande Ojara, Jimmyy Opee, Ayikoru Jackline, Eric Ssennuni and Simple Ouma in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941241251967 – Supplemental material for Efficacy of the Gulu University Reproductive Health Simulation Training for final year medical students and interns: a before-and-after study
Supplemental material, sj-docx-2-reh-10.1177_26334941241251967 for Efficacy of the Gulu University Reproductive Health Simulation Training for final year medical students and interns: a before-and-after study by Pebalo Francis Pebolo, Jerom Okot, Felix Bongomin, Silvia Awor, Baifa Arwinyo, Sande Ojara, Jimmyy Opee, Ayikoru Jackline, Eric Ssennuni and Simple Ouma in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-3-reh-10.1177_26334941241251967 – Supplemental material for Efficacy of the Gulu University Reproductive Health Simulation Training for final year medical students and interns: a before-and-after study
Supplemental material, sj-docx-3-reh-10.1177_26334941241251967 for Efficacy of the Gulu University Reproductive Health Simulation Training for final year medical students and interns: a before-and-after study by Pebalo Francis Pebolo, Jerom Okot, Felix Bongomin, Silvia Awor, Baifa Arwinyo, Sande Ojara, Jimmyy Opee, Ayikoru Jackline, Eric Ssennuni and Simple Ouma in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We acknowledge the Dean Faculty of Medicine, Dr Kaducu Felix, Deputy Dean Dr Ocaya Anthony, the Vice Chancellor of Gulu University Prof Openjuru George Ladaa, and Deputy Vice Chancellor of Gulu University, Associate Prof Owiny David for their tireless effort in guiding and supporting the formation and operationalization of Gulu University Simulation Laboratory. Special thanks go to the Medical Director of St Mary’s Hospital Lacor, Dr Odong Emintone Ayella for the guide in formulating the Gulu University Reproductive Health Simulation Training Curriculum. Special thanks to the Association of Obstetricians and Gynecologists of Uganda (AOGU) for their kind reviews and input in the curriculum and training of the trainers.
Declaration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.