
Abstract
Objectives:
While Nepal has made significant improvements in maternal and newborn health overall, the lack of maternal and newborn health–related knowledge in the more rural parts of the country has led to significant disparities in terms of both maternal and newborn health service utilization and maternal and newborn health outcomes. This study aimed to assess whether viewing culturally adapted maternal and newborn health educational films had a positive impact on (1) the maternal and newborn health knowledge levels among pregnant women and (2) the postpartum hemorrhage–related knowledge levels among Female Community Health Volunteers in rural Nepal.
Methods:
Four locations were selected for their remoteness and comparatively high number of pregnancies. A convenience sample of 101 pregnant women and 39 Female Community Health Volunteers were enrolled in the study. A pre- and post-test design was employed to assess this intervention. Paired t-tests were used to analyze the change in number of correct responses by knowledge domain for multi-film participants, producing a numeric “mean knowledge score,” and McNemar’s tests were used to calculate the change and significance among select questions grouped into distinct themes, domains, and points of “maternal and newborn health–related knowledge” based on the priorities outlined in Nepal’s maternal and newborn health 2030 goals.
Results:
There was a significant improvement in knowledge scores on maternal and newborn health issues after watching the educational films for both types of participants. The mean knowledge score for pregnant women improved from 10 to 15 (P < 0.001) for the Understanding Antenatal Care (ANC) film, 3 to 10 (P < 0.001) for the Warning Sign in Pregnancy film, and 6 to 14 (P < 0.001) for the Newborn Care film. For the Female Community Health Volunteers, knowledge also significantly improved (P < 0.05) in all except one category after watching the postpartum hemorrhage film. The percent that correctly answered when to administer misoprostol (80%−95%) was the only variable in which knowledge improvement was not significant (P < 0.057).
Conclusion:
Using culturally adapted educational films is an effective intervention to improve short-term maternal and newborn health–related knowledge among rural populations with low educational levels. The authors recommend additional larger-scale trials of this type of intervention in Nepal and other low- and middle-income countries to determine the impact on long-term maternal and newborn health knowledge and behaviors among rural populations.
Keywords
Introduction
Maternal mortality is a globally accepted proxy indicator for development, the overall strength of health systems, and their ability to reach vulnerable populations. As such, the World Health Organization included the ambitious goal of reducing the global maternal mortality ratio to less than 70 per 100,000 live births by 2030, as well as reducing the neonatal mortality rate to at least as low as 12 per 1000 live births, as part of its targets for “Sustainable Development Goal 3: Ensure healthy lives and promote well-being for all at all ages.” 1 Many countries, including Nepal, have followed suit and heavily invested in Maternal and Newborn Health (MNH) within their national health policies. In recent years, Nepal’s prioritization of MNH has contributed to a significant reduction in the official country-wide maternal mortality ratio, from 529 per 100,000 live births in 1996 to 239 per 100,000 live births in 2016, and a decrease in the neonatal mortality rate from 50 to 21 deaths per 1000 live births in the same period. 2 While impressive, this progress has not been evenly distributed across the country. Significant disparities persist between rural and urban areas of Nepal, particularly in terms of resource availability, availability of quality MNH services, and women’s ability to access care. 3
The disparities in MNH service utilization between urban and rural areas of Nepal are reflected in the local institutional delivery rates, a metric commonly used to assess the use of MNH services. The 2016 Demographic & Health Survey reported that although 69% of women in urban areas had institutional delivery, only 44% of women in rural areas had an institutional delivery. In rural Nepal, the low awareness and lack of MNH-related knowledge among the general population negatively impact the utilization of MNH services.4–6 As a result, many rural women still do not attend proper Antenatal Care (ANC) and subsequently deliver without a Skilled Birth Attendant, thereby placing themselves and their infants at heightened risk of conditions like Postpartum Hemorrhage (PPH), a manageable condition with appropriate MNH care, and currently the leading cause of maternal mortality in Nepal. 7
At the community level, there is a well-established network of over 50,000 Female Community Health Volunteers (FCHVs) under the oversight of the Government of Nepal. FCHVs are typically local women, often past their childbearing years, who advocate healthy behavior and promote safe motherhood, child health, family planning, and other community-based health promotion and service delivery. They receive basic training in various primary health center topics, including MNH services, but the government of Nepal still struggles to implement appropriate training for these dedicated volunteers, particularly within most of the remote areas of Nepal.
By making relevant information on pregnancy, labor, and delivery more readily available to rural communities and providing supplemental training for FCHVs, MNH programs can motivate local communities to adopt more effective MNH practices, support local health volunteers in improving the quality of their services, and promote the benefits of institutional delivery and other available health services. 8
The Information Education Communication approach generates awareness within communities to promote health-seeking behaviors appropriate to their specific settings. According to the Center for Disease Control, the Information Education Communication approach aims “to change or reinforce a set of behaviors in a target audience regarding a specific problem in a predefined period of time.” In conjunction with Behavioral Change Communication, Information Education Communication enables changes by empowering communities to initiate and sustain positive behavior.
Recognizing the potential impact that the combined use of Information Education Communication and Behavioral Change Communication could have on improving MNH service utilization in rural Nepal, One Heart Worldwide (OHW) and Medical Aid Films worked in partnership with the National Health Education Information and Communication Center (NHEICC), a government body required to authorize the production and distribution of any Information Education Communication/Behavioral Change Communication materials within the country, to develop a series of short educational films specifically adapted to the socio-cultural and MNH care delivery context of rural Nepal. Films were selected as the medium for this project because an emerging body of literature suggests that film-based educational delivery is effective in improving short-term health knowledge. Furthermore, additional studies have confirmed that locally developed films strongly amplified the ability to raise awareness among local community members.9,10
The following study aims to measure the efficacy of socio-culturally adapted audio-visual presentations on improving the MNH knowledge of pregnant women and FCHVs in rural Nepal through the use of four short educational films. The ultimate goal of the study is to determine if this easily scalable approach effectively communicates critical information on MNH topics, with the hope that this could be utilized in rural areas in other low- and middle-income countries.
Methods
Film production
Four themes were selected for film production as follows: (1) Understanding Focused ANC, (2) Warning Signs in Pregnancy, (3) Newborn Care, and (4) PPH Management. These four topics were selected based on the Government of Nepal’s focus areas within MNH, as found in the Nepal Safe Motherhood and Newborn Health Road Map 2030. 11 Films 1–3 were intended to help pregnant women, husbands, and family members better understand life-saving information related to MNH. Given that PPH is the leading cause of maternal mortality in Nepal, the fourth film was intended to enhance the capacity of rural FCHVs to appropriately identify and prevent PPH by administering misoprostol as its distribution is a part of their mandate. All the technical contents and scripts were reviewed and approved by the NHEICC technical working group, a government body authorized to review and approve any health-related Information Education Communication/Behavioral Change Communication materials, including the videos.
Study site
Once completed, the four educational films were presented to pregnant women and FCHVs in the health facilities of four communities (Dhitung, Durchim, Aarkhauley, and Chyasmitar) of the Haleshi municipality in the district of Khotang. These four locations were selected based on their remoteness and comparatively high number of annual pregnancies.
Study design
Researchers chose to implement a pre- and post-study design to measure changes in MNH knowledge levels. This study was conducted as a single-arm experiment, measuring participants before and after the intervention. Responses were grouped by domain and the mean value of improvement/familiarity with MNH concepts, “mean knowledge score,” as measured by the average percentage of correct answers, was the primary outcome in this study. In addition, while the authors surveyed the participants about all facts explained in the videos, this study focused on specific points of “MNH-related knowledge,” based on the priorities outlined in Nepal’s Safe Motherhood and Newborn Health Road Map 2030, which were either selected from among the questionnaire or were measured by combining multiple responses from the questionnaire.
Sample size
A convenience sample of 116 pregnant women was shown films 1–3, but 15 were excluded from the analysis because they declined to participate in either the pre- or the post-test. In total, 101 pregnant women who watched films 1–3 and participated in both pre- and post-tests were included in the study analysis. Thirty-nine FCHVs watched film 4 on the PPH management, participated in both the pre- and post-test, and were included in the study.
Data collection
Informed written consent was obtained from all participants before the educational films were shown. Researchers first administered pre-test questionnaires to all participants. For the pregnant participants, films 1–3 were shown, after which researchers administered post-test questionnaires immediately to assess their knowledge in three themes: Understanding ANC, Danger signs during pregnancy, and Newborn Care. As shown in Appendix 1, under each theme, questions were categorized into domains based on the Government of Nepal’s 2030 MNH goals. Under the theme “Understanding ANC,” there were 14 questions across four domains: knowledge on ANC, knowledge on tetanus toxoid (TT) vaccine, knowledge on maternity incentives, and knowledge on birth preparedness. Under the theme “Danger signs during pregnancy,” there were 16 questions across four domains: danger signs during pregnancy, knowledge on anemia, knowledge on eclampsia, and knowledge on infection. Finally, under the theme “Newborn Care,” there were 15 questions across five domains: cord care, thermal protection, breastfeeding, post-natal examination of newborn, and danger signs in newborn.
Thirty-five total questions were administered in a free-response format to the pregnant women cohort, with between one and four correct answers possible per question. One point was awarded for each answer provided, with a total possible knowledge score for the ANC, Warning signs, and Newborn films of 19, 20, and 20, respectively. For FCHV participants, film 4 was presented, after which researchers administered the post-test questionnaire to test their knowledge of PPH management. The seven questions were likewise administered in a free-response format, and for each correct answer, one point was given. The questionnaires utilized were adapted versions of questionnaires provided by Medical Aid Films and have not yet been validated for internal reliability.
Data analysis
A total of 42 questions (see Supplemental File) were administered to the pregnant women and FCHVs, and the responses were categorized into 1 of 13 domains and grouped into 1 of 3 themes (see Appendix 1). T-tests were utilized to determine the change in total “mean knowledge scores” for multi-film participants. McNemar’s test was applied to determine whether there was a significant difference in the percent of participants answering questions correctly in each specific “MNH-related knowledge” based on Nepal’s 2030 MNH goals, before and after watching the films. Results were considered statistically significant if they had a P-value < 0.05.
Results
Demographics
The pregnant participants’ age ranged from 15 to 44 years, with a mean value ± standard deviation (SD) age of 24 ± 6 years, although less than a third of all pregnant women were above 25 years old. Out of the 101 participants, 53% were primigravidas. The median age of marriage for the participating women was 18 years old, and one-third had given birth to at least one child by age 20 years, mirroring the high prevalence of early marriages and pregnancies in these communities. In addition, 21% of pregnant women had never gone to school, 20% had below a primary level of education, 44% had below a secondary level of education, and only 14% had secondary or above secondary education.
Participating FCHVs ranged in age from 21 to 61 years, with a mean ± SD age of 41 ± 12 years. Over half had primary education or less, although just over a third had completed their secondary education. Their experience as FCHVs ranged from 5 months to 35 years, with a mean ± SD of 14 ± 10 years.
Films 1–3
The results show a marked improvement in pregnant women’s MNH-related knowledge after watching the three educational films, as shown in Figure 1. While improvement was seen for all three films shown to pregnant women, the Warning Signs on Pregnancy film demonstrated the most dramatic increase despite having the lowest post-test scores overall, due to the markedly lower participant pre-intervention knowledge.

The change in mean knowledge score by film between pre- and post-test.
A breakdown of participants’ mastery of the specific topics covered in films 1–3 can be found in Table 1. The MNH-related knowledge of all participating pregnant women improved significantly across all domains (P < 0.04)
Improvements in “MNH-related knowledge” levels among pregnant women after watching films 1–3.

ANC: Antenatal Care.
Percent of women who responded correctly to this question on the test.
They were able to name at least two components of the Birth Preparedness Package: (1) identification of health worker and health facility for delivery, (2) saving money, (3) arranging transport, and (4) identifying two persons for blood donation.
Film 4: PPH management film targeted to FCHVs
Knowledge significantly improved regarding the measurement of blood loss after delivery (44%−85%, P < 0.001), the timing of giving misoprostol (67%−97%, P = 0.001), the dose of misoprostol (62%−100%, P < 0.001), and when should FCHVs provide misoprostol to pregnant women (74%−92%, P = 0.033). Knowing when to administer misoprostol (80%−95%) was the only variable in which knowledge improvement was less noteworthy. The percentage change on this parameter was lower and statistically insignificant (P = 0.057). The full results appear in Table 2.
Improvements in “MNH-related knowledge” levels among FCHVs after watching film 4.
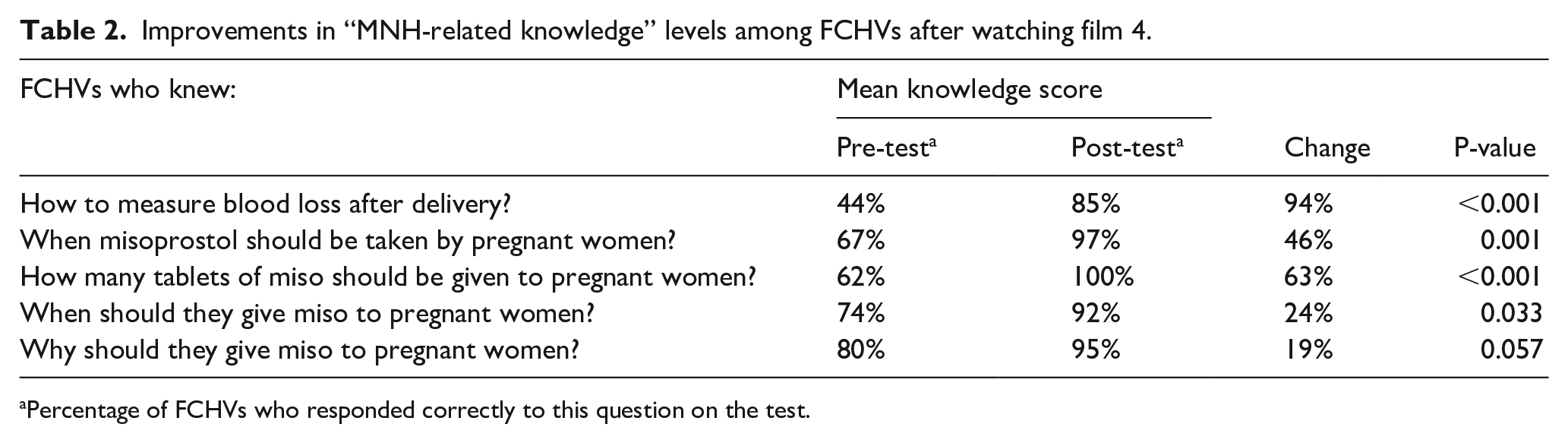
Percentage of FCHVs who responded correctly to this question on the test.
Power analysis
As our study participants were part of a convenience sample, a power analysis was performed retrospectively for the pregnant women and FCHV groups to confirm a sufficiently powered study using G power 3.1.9.4. For the pregnant women group, setting alpha = 0.05 and finding the effect size to be 1.5 with a correlation of 0.55, the power was determined to be 100%. For the FCHV group, setting alpha = 0.05 and finding delta = −0.44, p12 = 0.46, and p21 = 0.02, the power was determined to be 99.5%.
Discussion
The purpose of this investigation was to determine whether a culturally adapted audio-visual approach would be effective at improving MNH knowledge in rural Nepal. Our pilot project adapted four Medical Aid Films’ educational videos to the local socio-cultural and healthcare delivery context to test the efficacy of this approach in the specific context of rural Nepal. We found that the improvements in MNH knowledge between the pre-film and post-film questionnaires for all four films demonstrated a statistically significant improvement in the immediate knowledge of pregnant women and FCHVs. These results suggest that our educational films effectively communicate critical information on MNH topics, especially in remote rural communities such as those featured in the study.
It has been previously reported that a significant proportion of pregnant women attending tertiary birthing centers do not have adequate knowledge of obstetric danger signs. 12 Among the tested pregnant women, “Warning Signs During Pregnancy” and “Newborn Care,” the percentage of correct responses increased by nearly the same amount. However, of the two, the knowledge for “Warning Signs” was markedly lower in the pre-test. Although all domains saw a significant increase in the number of pregnant women answering correctly post-video, two areas remained below a 50% correct response rate in the post-test. The first was recognizing at least one symptom of pre-eclampsia, and the other was about the correct timing for their post-natal check-up. There are multiple possibilities for why these questions received such low mean knowledge scores, including poor question design, previous unfamiliarity with the topic, the free-response design of the survey, or even how the material was presented. As both are of utmost concern, we hope future studies will make modifications to the presentations to ensure improved scores in these domains. We are unsure whether the quality, time spent, or explanation of the presentation material was insufficient in these areas or if a previously unaccounted for cultural component impeded effective adaptation of the material in this regard.
FCHVs that viewed film 4, focusing on aspects of maternal and neonatal health care that most often lead to adverse outcomes, improved significantly in all domains, except for “Why should you give misoprostol to pregnant women?” However, even in this domain, correct responses increased from 80% to 95%. This is likely due to the number of FCHVs that had prior knowledge of the indicators for misoprostol administration before watching the MNH films. However, “How many tablets of misoprostol should be given to pregnant women?” increased from 62% to 100%. These improvements in knowledge about the use of misoprostol are crucial as multiple studies have found the use of misoprostol to prevent adverse outcomes due to PPH, especially in low-resource settings.13–15 Of note, less than half of FCHVs knew how to measure blood loss after delivery before watching the video. However, 85% of FCHVs responded correctly after the presentation.
This study’s findings are consistent with previous investigations into the efficacy of audio-visual-based approaches to education. Educational films can be a powerful and effective tool to convey complex ideas in a minimal amount of time.16–18 Studies have shown that when educational videos have the appropriate cognitive load, viewers process visual information more quickly and efficiently than written text, retaining a greater quantity of quality information even with learning complex procedures.19–21 Moreover, both visual short- and long-term memory are separate from semantic short- and long-term memory, and when meaningfully integrated with a semantic encoding, memory recall is improved.22,23
This research had several limitations that should be considered while interpreting the results, including the timing of the post-test, the sample size, and the intrinsic issues of pre- and post-tests. As the participants were quizzed immediately after the film was shown, only short-term recall was tested. Additional research is needed to measure long-term knowledge retention and behavioral changes. Furthermore, due to the sample size surveyed, the results should be confirmed by a repeated trial with a larger group of participants. In addition, while pre- and post-studies have the statistical strength to suggest that the outcome “knowledge” was impacted by the intervention (viewing the films), they are limited by a variety of factors, including lack of randomization of the sample, the lack of a control group or second arm, and priming the subjects for what questions will be asked in the post-test. Further research is necessary to confirm the internal validity of the study for testing the effect as well as the videos’ long-term effects on MNH knowledge, which will require additional studies. Finally, we hope to include husbands in future studies as previous research has shown that educating pregnant Nepalese women together with their male partners has yielded a greater net impact on maternal health behaviors than educating women alone. 24
Conclusion
In conclusion, this study found that viewing the specially produced MNH educational films had a positive impact on (1) the knowledge level related to MNH among pregnant women and (2) the knowledge level related to PPH among FCHVs. After watching the educational films, there was a significant improvement in knowledge scores on MNH issues for both types of participants. This result implies that audio-visual programs at the community level may be an effective tool to increase the knowledge level of highly vulnerable populations and the FCHVs who care for them. Based on this study’s positive short-term results, our team is now providing the videos to all the birthing centers within OHW’s current program districts to be shown to pregnant women in the waiting rooms. In addition, our team recommends that the Government of Nepal, and the governments of other Low- and Middle-income countries, encourage larger-scale trials to determine long-term efficacy in improving MNH knowledge in rural areas.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221104297 – Supplemental material for Socio-culturally adapted educational videos increase maternal and newborn health knowledge in pregnant women and female community health volunteers in Nepal’s Khotang district
Supplemental material, sj-docx-1-whe-10.1177_17455057221104297 for Socio-culturally adapted educational videos increase maternal and newborn health knowledge in pregnant women and female community health volunteers in Nepal’s Khotang district by Sajana Maharjan, Liladhar Dhakal, Linda George, Bhagawati Shrestha, Helen Coombe, Surya Bhatta and Sibylle Kristensen in Women’s Health
Footnotes
Appendix 1
Questions, domains, themes, and possible knowledge scores.

| Theme, domain, and question | Possible score |
|---|---|
| Understanding ANC | 19 |
| Knowledge on ANC | 10 |
| Why is the ANC important? | 3 |
| How many times ANC check-up should be done? | 1 |
| When should the ANC check-up be done? | 1 |
| Care during pregnancy | 4 |
| Place of delivery | 1 |
| Knowledge on TT | 2 |
| Why is TT injection given? | 1 |
| How many doses of TT injection should be given? | 1 |
| Knowledge on maternity incentives | 3 |
| Heard about maternity incentives | 1 |
| How much is given to mothers? | 1 |
| Heard about increased incentive? | 1 |
| Knowledge on birth preparedness | 4 |
| Identification of HWs/HF for delivery | 1 |
| Saving money | 1 |
| Transportation arrangement | 1 |
| Identifying two persons for blood donation | 1 |
| Knowledge on danger signs | 19 |
| Danger signs during pregnancy | 7 |
| Bleeding | 1 |
| Headache | 1 |
| Swelling of hands/feet | 1 |
| Blurred vision | 1 |
| Abdominal pain | 1 |
| Vomiting | 1 |
| Fits/seizures | 1 |
| Knowledge on anemia | 7 |
| Understanding anemia | 1 |
| Signs/symptoms of anemia | 3 |
| Ways to prevent anemia | 2 |
| Knowledge on iron intake | 1 |
| Knowledge on eclampsia | 3 |
| Symptoms on eclampsia | 3 |
| Knowledge on infection | 2 |
| Symptoms of infection | 2 |
| Newborn care | 20 |
| Cord care | 2 |
| Cord cutting instrument | 1 |
| Application of CHX on cord | 1 |
| Thermal protection | 4 |
| When should a newborn be bathed? | 1 |
| What should be done to keep the newborn warm? | 3 |
| Breast feeding | 5 |
| When should a newborn be breastfed? | 1 |
| Benefits of breastfeeding | 4 |
| PNC examination of newborn | 1 |
| When should examination of newborn be done | 1 |
| Danger signs in newborn | 8 |
| Grunting/wheezing sound | 1 |
| Increasing breathing | 1 |
| Rashes/blisters on skin | 1 |
| Fits/convulsion | 1 |
| Infection in eyes or navi | 1 |
| Hot or cold | 1 |
| Difficulting in sucking mother’s milk | 1 |
| Baby is less active or not moving as usual | 1 |
ANC: Antenatal Care; TT: tetanus toxoid; CHX: chlorhexidine digluconate; PNC: postnatal care; HWs: health workers; HF: health facility.
Acknowledgements
The authors thank the National Health Education Information and Communication Center (NHEICC), Family Welfare Division, Medical Aid Films, and the Vitol Foundation for their support in the development of the videos.
Author contribution(s)
Availability of data and materials
The data sets and tools used for this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance from NHRC (Reg.no.541/2018) and informed written consent were obtained from all the respondents.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a subcontracted grant from the Vitol Foundation through Medical Aid Films.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.