
Abstract
Background:
Family planning helps to reduce the number of high-risk births and prevent unplanned pregnancies and mother-to-child transmission of HIV. The main purpose of this study was to determine the usage of family planning and its associated factors among women living with HIV who attended care and treatment clinics.
Methods:
This was a health facility–based cross-sectional study conducted among 332 sexually active reproductive-age women living with HIV who visited care and treatment clinics from 15 April and 15 June 2017. We used a systematic sampling technique for sample selection. The data were collected using pretested and structured questionnaires through face-to-face interviews. Seriously ill women living with HIV who were unable to respond to the questionnaire and refused to participate were excluded from this study. Logistic regression was fitted, and an odds ratio with a 95% confidence interval with a p value less than 0.05 was used to identify factors associated with modern family planning use.
Result:
The study revealed that the overall use of the modern family planning method was 56.3%, and the most common method used was injectable (37.4%) followed by implants (28.9%). About 19% of the users reported dual contraceptive use. About 58% got family planning from antiretroviral therapy clinics. Almost all the women (97.6%) had heard of seven modern family planning methods. Desire to have another child was the most common (79.7%) reason for not using family planning. Women who attended primary/secondary education (adjusted odds ratio: 2.61; 95% confidence interval: 1.29–5.28], who had no future fertility desire (adjusted odds ratio: 2.94; 95% confidence interval: 1.51–5.73), who had discussed family planning with their husband (adjusted odds ratio: 2.06; 95% confidence interval: 1.04–4.10), and who were counseled by the antiretroviral therapy provider about family planning (adjusted odds ratio: 4.53; 95% confidence interval: 1.70–12.06) were more likely to use family planning methods than their counterparts.
Conclusion:
The results of this study revealed that the use of modern family planning was low. There is a high frequency of implant usage, fear of mother-to-child transmission as a motivator for family planning usage, and low dual method usage. Hence, improving women’s education, involving husbands, and consistent family planning counseling by antiretroviral therapy providers are promising strategies to improve the uptake of modern family planning by women living with HIV.
Keywords
Introduction
Family planning (FP), one of the most cost-effective investments, 1 ensures maintenance of optimal health for women living with HIV (WLHIV), prevents mother-to-child transmission (MTCT) of HIV, and reduces the number of AIDS orphans. WLHIV have diverse FP needs, 2 and the need for FP is being satisfied with modern methods.3–6 According to the World Health Organization (WHO), the health sector strategy on HIV 2016–2021, global targets for 2020 are to reduce new HIV infections to less than 500,000 and zero new infections among infants. 7 Adding FP services to HIV care and treatment might facilitate the uptake of contraceptives by WLHIV, helping to maintain their health, plan safer pregnancies, and reduce the rate of MTCT of HIV.8–14
Low FP use among WLHIV was reported by studies from Africa and elsewhere; a study finding from Ghana reported 42.6% of modern contraceptive use among WLHIV. 15 Besides, from a study conducted to assess the situation of FP and HIV integrated services in five sub-Saharan African (SSA) countries including Kenya, Rwanda, South Africa, Uganda, and Ethiopia, only 12–37% of WLHIV used modern FP. 13 The contraceptive use rate was moderate at 50.6% in Lagos, Nigeria. 16 On contrary, studies conducted in Tanzania, Togo, and Uganda showed that 68.5%, 73.1%, and 85% of WLHIV had used modern FP, respectively,17–19 while it is 95% in South Africa. 20
In Ethiopia, an estimated HIV prevalence among women of reproductive age (WRA) is reported to be 1.9% since 2011, 21 while the rate of MTCT remains more than 20% in 2014. 4 Likewise, the persistent increase in rates of unintended pregnancy among WLHIV and the presence of the unmet need for modern FP (as high as 25%) are important public health challenges. 22 Further, several studies conducted in various regions of Ethiopia revealed discrepancies in the usage of modern FP among this key population group varying from very low to high rate of the contraceptive prevalence rate (CPR) 21,23–31.
The literature identified multiple factors affecting the use of modern FP. Women’s age,16,21,25,27,32,33 level of educational attainment,18,21,24,26,28,29,33,34 marital status,25,31,35 level of earnings, and wealth status 21,25,33,36 are the factors associated with modern FP method use. Likewise, studies showed having information or knowledge of modern FP,21,30,36–38 knowledge of HIV-positive status, 39 attitude held by women toward modern FP 21,30 is the determinant of modern FP use by women. Furthermore, studies indicated that the number of living children and lack of future fertility desire are associated with FP use.20,24,28,30,31,37 Moreover, WLHIV who know their status is more likely to use condoms or dual method.20,32,39 Cultural bans over fertility control and religious beliefs are other reasons for not using FP methods. 40 The study also identified that FP counseling and advise given at health care facilities, 40 partner support and discussing with a partner,2,23–25,32,41 and access to a full range of FP service more notably integrating such services into the chronic HIV treatment and follow-up care 26,30,35,37,42 are associated with a higher rate of FP use.
The use of modern FP methods among WLHIV is different in different settings. The HIV prevalence among women in Ethiopia is low, though the rate of vertical transmission is 20%. This contrasts with other neighboring countries that have higher HIV prevalence and lower vertical transmission rates. Individuals with HIV/AIDS wished to limit their fertility but experienced a high unmet need for contraception. One reason could be the lower FP use among Ethiopian women, and identifying factors associated with modern FP use in this context could help inform policy-maker.
Also, most previously conducted studies are concentrated on the general population. To the best of our knowledge, there is no study conducted among WLHIV in Jigjiga town. Likewise, the ethnic makeup (e.g. language, religion, ethnic group) of Jigjiga differs from that of overall Ethiopia. Furthermore, existing national data or studies from other regions may not be representative of WLHIV in Jigjiga. Hence, the study aimed to assess the frequency of modern FP usage and its associated factors among women living with HIV/AIDS who attended chronic HIV care and treatment clinics (CTCs) at public health facilities in Jigjiga town, Eastern Ethiopia.
Methods
Study area, participants, and sampling
A health facility–based cross-sectional study was conducted from 15 April to 15 June 2017 at CTCs of three public health facilities of Jigjiga town. Jigjiga town is the capital of the Ethiopian Somali National Regional State, Eastern Ethiopia, which is located at 628 km away from Addis Ababa (the capital city of Ethiopia). There is 1 referral and general public hospital, 1 private hospital, 2 health centers, 1 maternal and child health (MCH) clinic, and around 30 higher and medium clinics in the town. Based on the 2007 population projection for the year 2013–2014, the population of Jigjiga town was estimated to be 125,876 of which 58,751 are women. Antiretroviral therapy (ART) service and prevention of mother-to-child transmission (PMTCT) programs are only provided by Meles Zenawi Memorial Referral Hospital, Karamara general hospital, and Ablale health center. Currently, the estimated overall number of WLHIV in the catchment area of Jigjiga was more than in 1750. About 1190, 386, and 192 WLHIV were getting services from CTCs of the three public health facilities, respectively. Before this study, the Ethiopian Somali Regional State HIV prevalence was estimated to be 0.75 for 2017. 43
The source population was all people living with HIV/AIDS (PLWHA) who attended the CTCs of the selected public health facilities of Jigjiga town. Selected sexually active reproductive-age (15–49 years old) WLHIV who attended CTCs of the three public health facilities and consented to participate in this study were the study population. Seriously ill WLHIV who were unable to respond to the questionnaire and refused to participate were excluded from this study.
The sample size was determined by using the single population proportion formula, with the following assumptions: proportion (p) of a population using modern FP to be 46.3% as estimated from the study conducted in northern Ethiopia, 23 among HIV-infected women, confidence interval (CI) of 95%, and 5% of marginal error (d). Then, the final sample size calculated considering the finite population correction formula and adding 10% for the nonresponse rate was 345. Public health facilities in Jigjiga town, which provide chronic HIV care and treatment follow-up service, were purposively included in the study. The sample size was proportionally allocated to the health facilities based on the total number of clients, and a systematic sampling technique was used to select participants from each facility by using client flow as the sampling frame.
Study variables
The dependent variable was the use of modern FP. The independent variables in this study were divided into six categories. They were the following: (a) Sociodemographic, this category included variables such as age, residence, education level, marital status, religion, ethnicity, occupation, and monthly income; (b) Reproductive history and fertility desire, this category included variables such as the number of live birth and alive children, pregnancy status after being infected with HIV, and fertility desire, and the number of desired children; (c) Community-related factors, this category involved variables such as religious and cultural influence, perceived partner or important others support, and women’s approval of FP; (d) Client-related factors, this category constituted knowledge on FP methods (yes or no questions regarding knowledge on the seven commonly used FP methods), sources of information, and attitude toward the use of FP; (e) Service-related factors including counseling, availability, and accessibility of FP services; and (f) Perceived reasons for using or not using FP methods.
Operational definitions
Sexually active: A woman who reported having sexual intercourse at least once in the last 3 months.
Modern FP method: This refers to FP methods such as oral contraceptive pills (OCPs), injectable (Depo-Provera), implants, intrauterine contraceptive devices (IUCDs), condoms, vasectomy (male sterilization), and bilateral tubal ligation (female sterilization).
Modern FP use: This refers to the use of at least one type of modern FP method.
Dual method: This refers to using two methods of contraception, which is using a condom with another contraceptive method.
Current FP user: Respondents who responded positively after being asked whether they are currently using (at the time of the survey) any modern FP methods to delay or avoid pregnancy.
Knowledge of modern FP: Women who knew of at least one modern method of FP.
Attitude toward modern FP use: The mean score was used as the cutoff point.
Positive attitude: The women whose total attitude score was greater than or equal to the mean value were categorized as having a positive attitude toward FP use.
Negative attitude: The women whose total attitude score was less than the mean value were categorized as having a negative attitude toward FP use.
Fertility desire: It is defined as HIV-positive women on chronic HIV care and treatment follow-up who would like to have child or children in the future.
CPR: Percentage of women who use any of the above listed modern FP methods.
Unmet need for FP: WLHIV who say they are not using contraception and who say either that they do not want any more children or that they want to wait 2 or more years before having another child are considered to have an unmet need for FP.
Data collection and analysis
Data were collected using a pretested structured questionnaire. A questionnaire was developed by adopting relevant questions from various sources 30,26,37,44. The questionnaire was translated into local languages, Amharic and Somali, by experts in both languages, and was translated back to English by another person to ensure consistency and accuracy. The Amharic and Somali versions of the tool were implemented for the study. Data were collected using interviewer-administered face-to-face interviews by three trained diploma midwives. The data collectors were recruited based on previous experience in data collection and fluency in the local languages. The principal investigator closely supervised the data collection process. Also, training was given for 2 consecutive days on how to interview, handling ethical issues, and maintaining confidentiality and privacy.
A pretest was conducted to familiarize enumerators with the administration of the interview process and for ensuring consistency. Debriefing sessions were held with the pretest field staff, and the questionnaires were modified based on lessons drawn from the pretest. The pretest was conducted among 35 reproductive-age group WLHIV (which is 10% of the sample) who were taking ART in the Awbare town health facility, 2 weeks before the commencement of the main data collection. Every completed questionnaire was cross-checked daily for inconsistencies and completeness.
Data were first checked manually for completeness and coded. Then, the data were cleaned and analyzed using SPSS version 20. Cleaning was done by calculating frequencies and sorting. Categorical variables were presented as either numbers or percentages. Means and standard deviations were presented for continuous variables. Bivariate analysis between dependent (the use of modern FP) and independent variables was performed using binary logistic regression. A p value of <0.25 was used as a criterion to select candidate variables for multivariate analysis. Multivariable logistic regression analysis was done to adjust for possible confounding variables. A p value of <0.05 with 95% CI for odds ratio (OR) was used in judging the significance of the associations. Results were presented in text, tables, and charts.
STROBE statement
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines are followed in this study.
Patient and public involvement statement
There are no patients or public participation in this study.
Ethical considerations
Ethical clearance and approval (protocol number: 137/2017) was obtained from the research ethics committee (REC) of the College of Health and Medical Science, Addis Ababa University (AAU). Besides, the official letters of cooperation were granted by the Ethiopian Somali National Regional Health Bureau and respective administrative offices of the health facilities. The purpose of the study was explained to the study participants, and recorded verbal informed consent was secured before data collection was started and confidentiality of the information was ensured by coding. Participation was voluntary after informed verbal consent, and responses were kept confidential. The consent procedure was approved by the ethics committee for all. The interview was undertaken privately in a separate area.
Results
Sociodemographic characteristics
The sociodemographic characteristics of the enrolled participants are presented in Table 1. Three hundred thirty-two participants have participated in the study with a response rate of 96.2%. The participants’ mean age was 31.4 years (±6.9 SD), and 43.4% of them were in the age group of 25–34 years. Three hundred one (91%) were urban dwellers, 146 (44.0%) followed the Muslim religion, and 124 (37.5%) belonged to the Somali ethnic group. One hundred ninety (57.2%) were currently married (cohabited), 132 (39.8%) had no formal education, and 101 (30.4%) were unemployed. Of 219 respondents who reported the total family monthly income, 118 (35.5%) of the respondents’ family had earned an income between 501 and 1500 Ethiopian Birr (ETB), and the median earning was 1226.2 ETB (with the interquartile range of 1293.5).
Sociodemographic characteristics of women living with HIV who attended CTCs of public health facilities in Jigjiga town, Eastern Ethiopia, 2017 (n = 332).

CTCs, care and treatment clinics. N indicates frequency.
Included Gurage, Wolayita, and Kambata.
Included student, farmer, and waitress.
Reproductive characteristics and fertility desire
The results of this study revealed that 266 (80.1%) of the participants had ever given live birth in their lifetime among which 148 (44.6%) of them had one to two live births in their lifetime. Moreover, 78 (23.5%) and 40 (12.0%) of the women had three to four and more than five live births, respectively. One hundred fifty-three (46.1%) of the women had at least one to two alive children, while 109 (32.8%) had at least three alive children. Also, 177 (53.3%) had become pregnant after they are aware of their HIV status, of which 38 (21.8%) of those pregnancies were unwanted. Concerning the desire for future fertility or for having more children, 171 (51.5%) expressed they have no further fertility desire. Yet of the women who have future fertility desire, 161 (48.5%), 105 (57.3%), and 77 (42.3%) of them have the desire to have one to two and three or more children in the future. On the other hand, 143 (43.1%) of their husbands have the desire to have children in the future.
Information source, knowledge, and attitude
Respondents were asked whether they knew any of the modern FP methods. Almost all the participants (97.6%) reported that they knew at least one method of FP. The most often mentioned source of information was health professionals (95.3%) followed by mass media (31.7%; Figure 1). The most well-known method of FP was injectable (88.6%), followed by condom (86.1%), pills (83.7%), implants (68.7%), and intrauterine devices (IUDs; 56.6%). Besides, 213 (64.2%) of the participants know at least four FP methods.
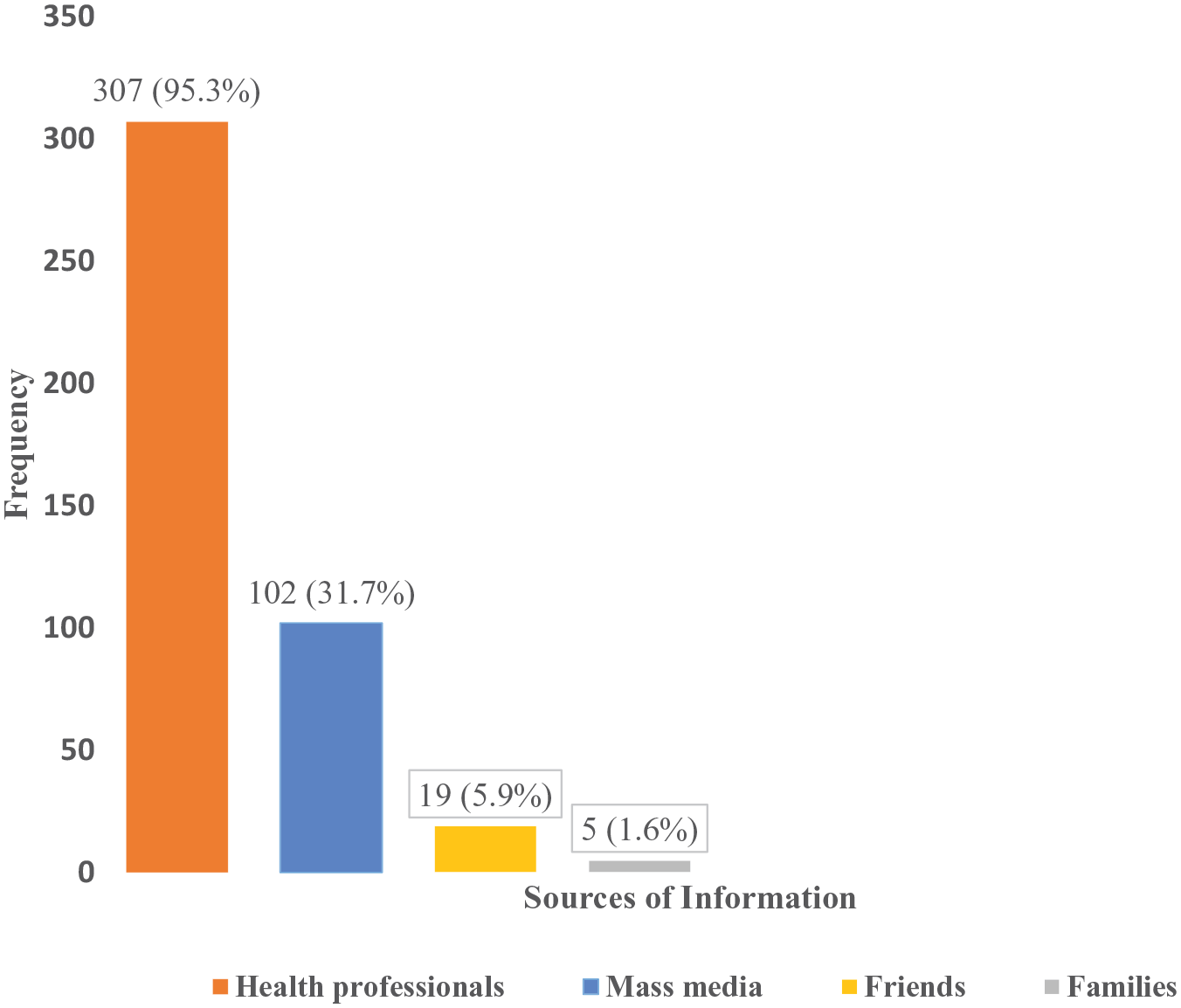
Source of information for family planning (FP) methods (multiple responses) for women living with HIV who attended care and treatment clinics (CTCs) of public health facilities in Jigjiga town, Eastern Ethiopia, 2017.
The mean score of attitudes toward modern FP and its use was found to be 48.57 (±6.82 SD) with a minimum score of 14 and a maximum score of 70. Using this mean score measure, 186 (56.0%) of the women had a positive attitude toward modern FP and its use. Majorities (68.1%) of participants were in favor of modern FP use.
Community-related characteristics
Two hundred fifty-three (76.2%) of the study participants indicated that their utilization of FP was not influenced by their HIV-positive status. One hundred ninety-seven (59.3%) had peer support and 204 (61.4%) had no support from their husband to use FP. Two hundred twenty (66.3%) of the study participants reported their religion does not affect their FP utilization. However, 210 (63.3%) of them were influenced by cultural dogmas held by their community. Regarding the decision-making role of a woman on contraceptive use, 291 (87.7%) had been involved in decision-making toward the use of FP. On the other hand, 113 (34.0%) of the participants had reported having an open discussion about FP with their husbands.
Service delivery–related factors
The study revealed that a large proportion (87.7%) of the respondents got counseling about FP from the ART provider. More than two thirds (64.5%) of the participants reported ART and prevention of MTCT service did not influence their desire to be pregnant. Moreover, 74.7% and 77.4% of the participants mentioned that they accessed modern FP whenever they needed and health facilities met their need for FP, respectively.
Modern FP use
Two hundred forty (72.3%) women had ever used at least one method of FP. Similarly, 234 (70.5%) of the women had ever used at least one method of FP after they become HIV positive. One hundred eighty-seven (56.3%) of the women were currently using at least one FP method of which 108 (57.8%) of the women have indicated that they do not have future fertility desire. Figure 2 indicates the most commonly used contraceptive method is injectable (37.4%), followed by implants (28.9%) and dual contraceptives (18.7%). While oral contraceptives and IUDs are the least used, the use of permanent contraceptive was not reported at all by the participants of this study. Moreover, 212 (63.9%) of the participants had the desire to use modern FP in the future.

Type of family planning (FP) method used by women living with HIV who attended care and treatment clinics (CTCs) of public health facilities in Jigjiga town, Eastern Ethiopia, 2017.
All the current users (100%) had their preferred FP method free of charge. One hundred eight (58%), 46 (24.6%), and 33 (17.6%) of the women were reported that they obtained their current method of FP from ART clinics, FP clinics, and nongovernmental (or family guidance association) clinics, respectively. Furthermore, of those who had a desire to use modern FP in the future, 199 (93.9%) of the women were reported they prefer ART clinic to provide FP service in the future.
Perceived reasons for using and not using FP methods
Figure 3 presents both reasons for using and not using modern FP. Fear of MTCT of HIV was the most common (42.8%) reason for not using FP followed by other health concerns (29.4%). Only 15% wanted to space births and 11.2% wanted to limit births. One hundred forty-five (43.7%) of the participants were not using any method of FP (currently nonuser). Among them, the most common reason (76.6%) for not using any FP method was due to the desire to have children. Other reasons were religious prohibition (35.9%), spouse’s denial (17.9%), no knowledge of whether FP is indicated for PLWHA (13.8%), and fear of side effects of using FP methods (9.7%).

Perceived reasons for using or not using contraception among women living with HIV who attended care and treatment clinics (CTCs) of public health facilities in Jigjiga town, Eastern Ethiopia, 2017.
Factors associated with the use of modern FP
Results of binary logistic regression showed that women whose age was between 25 and 35 years, who attended primary and secondary education, those who were housewife or government and private workers, who were married, who had three to four live births (parity), and those who had three or more than three live children, who had a positive attitude toward FP, who had a discussion with their husbands about FP, who were counseled about FP by the ART provider, and whose husbands had no future fertility desire and approved the use of FP were identified as associated factors of modern FP use at a p value less than 0.25.
In multivariable logistic regression analysis, four variables, that is, women’s educational status, women’s future fertility desire, discussion with husband about FP, and counseling of FP by the ART provider, were associated with the use of modern FP methods. When compared with those who had no formal education, women who attended primary/secondary education were 2.61 times more likely to use modern FP [adjusted odds ratio (AOR): 2.61; 95% CI: 1.29–5.28]. Also, women without future fertility desire were 2.94 times more likely to use modern FP than women who desire to have children in the future (AOR: 2.94; 95% CI: 1.51–5.73). Likewise, women who had a discussion about FP with their husbands and who received counseling about modern FP from their ART provider were 2.06 and 4.53 times more likely to use modern FP than their counterparts (AOR: 2.06; 95% CI: 1.04–4.10) and (AOR: 4.53; 95% CI: 1.70–12.06), respectively (Table 2).
Factors associated with modern FP use among women living with HIV who attended CTCs of public health facilities in Jigjiga, Eastern Ethiopia, 2017 (n = 332).

AOR, adjusted odds ratio; ART antiretroviral therapy; CI, confidence interval; COR, crude odds ratio; CTCs, care and treatment clinics; FP, family planning.
N indicates frequency.
Significance for bold values, *p < 0.05 and **p < 0.01.
Discussion
This study assessed the frequency of modern FP use and its associated factors among reproductive-age WLHIV on chronic care and treatment follow-up attending public health facilities in Jigjiga town, Eastern Ethiopia. The study revealed that 97.6% of the study participants know at least one modern FP method and 68.1% of the study participants were in favor of FP utilization. Similarly, knowledge of contraceptive methods is almost universal in Ethiopia. However, the finding of this study is higher than the result of the Ethiopia Demographic and Health Survey (EDHS) 2016 report for the Somali Regional State, in which only 79% of currently married women know at least one method of contraception. 45 In another way, even though there is a high proportion of knowledge and women’s approval of modern FP use, the CPR is paradoxically lower. This implies the fact that knowledge and approval of FP by women does not necessarily lead them to utilize FP.
The proportion of modern FP use by WLHIV (56.3%) in this study is almost consistent with the findings of previous similar studies in different parts of Ethiopia, Kenya, and Nigeria in which 50%, 56.7%, 55.5%, and 50.6% of participants used contraceptives, respectively.37,16,29,35 On the other hand, the finding of this study is higher than that of similar studies conducted among WLHIV in Ethiopia and Ghana, which had reported a CPR of 47.9%, 31.7%, 44.3%, 46%, and 42.6%, respectively.24,15,23,27,28 Likewise, the prevalence of modern FP use in this study is higher compared with national EDHS finding, which was 35% (51), and far higher than the national report of 2016 for the Somali Regional State (which was only 1%). The inconsistency might be occurred due to differences in the study populations and can be associated with the integration of FP services into the chronic HIV care and treatment services where HIV-positive women attending ART clinics get access to frequent counseling about FP as part of their HIV care and follow-up. The EDHS used currently married women of the reproductive-age group, while HIV-positive women of the reproductive-age group were considered study populations in this study. The observed inconsistency might be due to differences in sampling and/or sociodemographic characteristics of study populations.
However, inconsistently, similar studies undertaken in different areas including studies in Addis Ababa (two studies) and southwest Ethiopia, South Africa, Togo, Uganda, and Nepal reported a significantly higher rate (64.1–95%) of modern FP use by HIV-positive women.18–20,31,44,25 The higher rate of contraceptive use among WLHIV in these study areas might be due to HIV/AIDS care and FP service integration and high-quality service delivery with access to different modern FP methods.
In this study, the most commonly used contraceptive method by WLHIV was injectable by 37.4%. This finding is in line with studies done elsewhere.19,30,31,28,46 Yet, the use of condoms and the dual method was found to be very low in this study. The possible reasons can be due to misconception and related negative attitudes toward condom use influenced by culture and religion. This finding is consistent with the result of a study in Ethiopia and Malawi, 28,39 however significantly low for the condom and dual method use compared with the finding reported by some other studies elsewhere.19,30,31,16,15 Higher rates of condom and dual method use in these studies might be due to service-related factors like the presence of active promotion and distribution of condoms.
However, the use of barrier contraceptives by HIV-positive women is a strongly recommended strategy to realize the goal of prevention of unintended pregnancy and avert subsequent vertical transmission of HIV. So, much has to be done to increase the utilization of this method of FP. Similarly, the use of short- and long-acting FP (IUDs) including permanent methods in this survey was low. The finding is similar to the report of other similar studies.30,37,16,28 The implication could be the use of a variety of modern methods by HIV-positive women can be affected by several factors, including access to FP counseling, availability of different methods, access to numerous methods to meet individual preferences, and provider’s attitude and capability in providing different contraceptive methods.
More than half (57.8%) of the WLHIV of current FP users obtained their methods from ART clinics. This finding is significantly higher compared with the result of a study conducted in Bahir-Dar town (Ethiopia) which is 44.7%. 30 The possible reason for inconsistency might be the difference in the service delivery approach. Besides, in this study, 63.9% of WLHIV with a desire to use modern FP in some future time mentioned ART clinics as their preferred source. This finding is almost similar to results from similar other studies.30,37,26,35 This has programmatic implications for strengthening the integration of FP services with HIV care and treatment programs as it can be an opportunity to influence the current low uptake of modern contraceptives by this population group.
In the present study, WLHIV having formal education (primary and secondary education) are 2.61 times more likely to use modern FP than women who had no formal education. This finding is in line with the findings of the EDHS 2016 report and other similar studies conducted by hitherto.30,35,28 The high rate of modern FP utilization among women with better education might have been associated with increased women’s income and social independence where they are less likely to be influenced by social norms in making fertility and contraception decisions. Another plausible explanation might be that educated women have improved access to health care information and services. Therefore, educating women and empowerment helps in overcoming barriers to use modern FP methods.
In addition, WLHIV with no future fertility desire are about three times more likely to utilize modern FP methods than women who wish to have children in some future time. Similarly, previous studies from Ethiopia, Ghana, and Uganda showed HIV-positive women with no future fertility desire were found to have increased odds of FP utilization than their counterparts.19,30,28,15 The observed difference in FP utilization between these two categories could be HIV-positive women with no fertility desire are in a better position of utilizing modern FP methods, as they are more likely to want to prevent unintended pregnancy and the resultant vertical transmission of HIV.
Moreover, WLHIV who reported discussing FP with their husbands or partners have about two times higher chance of using modern FP than those who have not discussed FP with their husbands or partners. The positive association between spousal communication and contraceptive use has been well documented by previous similar studies undertaken in different areas.24,31,32,25,46 This implies discussion about modern FP between women and their partners and the related agreement can significantly affect contraception utilization as it enables them to make an informed decision on fertility and its control. This indicates the need for husband involvement in FP programs.
Furthermore, the chance of utilizing modern FP among WLHIV who received counseling about modern FP methods from their ART provider or counselor was 4.53 times higher than women who did not receive counseling from an ART provider or counselor. The result is consistent with findings from studies conducted in different countries in East Africa and south-east Asia 30,31,44,35,46 The explanation for this could be counseling on FP is a unique opportunity to provide information about FP and its widespread health benefits for WLHIV, which facilitates decision-making for use. Therefore, continuous, targeted, and tailored information provision along with strengthening the integration of FP services into HIV programs has paramount importance in scaling up FP (contraceptive) utilization among HIV-positive WRA.
Finally, this study has its strengths. First, it is targeted at the WLHIV, which are an important population group. Also, a random sampling technique was used to select the sample for the study through a direct face-to-face interview. However, this study does have some inherent limitations. First, the study design makes it difficult to determine the direction of causality, and there is a risk of social desirability bias whereby WLHIV may overreport their contraceptive use because of pressure from health workers and community members to practice protected sexual intercourse. Besides, clinical HIV and ART status that may contribute to the difference in FP use were not included in this study. Similarly, the use of other FP methods including emergency contraceptive methods was not considered in this study. This study sampled WLHIV from ART clinics; thus, the findings might not be generalized to all women with HIV because WLHIV attending the health care facilities may differ from women outside of the health care system.
Conclusion
In conclusion, this study showed that though there is a high desire to have children in the future, the use of FP was only half. The novel findings include the high frequency of implant usage, fear of MTCT as a motivator for FP usage, and low dual method usage. Women’s educational level, desire to have another child, having discussed FP with husbands, and receiving counseling about modern FP from ART providers were important predictors of modern FP use among WLHIV. Therefore, integrating FP services with HIV/AIDS care and support services and investing in women’s education, promoting gender equality, and empowering women, as these positively affect women’s level of decision-making and access to health care, could have a significant impact. Besides, through the prevention of unintended pregnancy, integrated services are likely to benefit MCH, prevent vertical transmission, and decrease the incidence of conception-related sexual transmission to discordant sexual partners. Furthermore, ART providers should provide FP counseling regularly. WLHIV who effectively used modern FP methods can be involved in peer-to-peer education.
Footnotes
Acknowledgements
We are very grateful to Addis Ababa University for the approval of the ethical clearance, and its financial support to the study. We express our heartfelt thanks to data collectors, and to participants for their willingness to participate in the study, without whom this research would be impossible.
Author contributions
HSA conceived and designed the study, supervised the acquisition of the data, and carried out the statistical analysis. EGS and GST participated in the design of the study and tool development and approved the proposal with some revisions. TGD participated in the statistical analysis, drafted, and revised the manuscript. EGS and NGD critically revised the manuscript. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Addis Ababa University postgraduate office funded the fieldwork of this research project.
Ethical approval and informed consent
Addis Ababa University (AAU), College of Health and Medical Science, research and ethics committee approved this study, and an informed verbal consent was obtained from all study participants.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.