
Abstract
Background:
The precise effect of ejaculatory abstinence on semen parameters is highly debatable, especially among subfertile men. Previous studies on effect of abstinence time on different semen parameters have reported controversial results. The aim of this study was to retrospectively assess the variance of semen parameters with different periods of ejaculatory abstinence among both a population of normozoospermic (n = 1621) and oligozoospermic (n = 416) Tamil men, presenting to a fertility clinic for an infertility evaluation (N = 2037).
Materials and Methods:
A retrospective analysis of 2037 semen analysis reports involved grouping patients based on their ejaculatory abstinence, that is, <24 h, 1 to 2 days, 3 to 7 days, 8 to 15 days, 16 to 30 days, and >30 days. All semen parameters were assessed as per the World Health Organization (WHO, 2010) recommended guidelines. The unpaired two-tailed t-test and Welch’s analysis of variance (ANOVA) combined with Games–Howell post hoc test were used for statistical analysis. A p value <0.05 was considered to be statistically significant.
Result:
A retrospective analysis of data (N = 2037) identified no statistically significant differences in semen parameters of sperm concentration, percentage of progressively motile sperm, and normal sperm morphology in both normozoospermic and oligozoospermic individuals across different groups of abstinence. Semen volume was the only parameter that showed a statistically significant difference in both groups (p < 0.0001). In both normozoospermic and oligozoospermic men, the group with <24 h abstinence had the highest mean percentage of progressively motile sperm and normal sperm morphology.
Conclusion:
The findings of this study suggest that ejaculatory abstinence may be highly arbitrary, and the recommendation of a strict 2- to 7-day abstinence per the WHO may be liberalized. In both normozoospermic and oligozoospermic men, semen parameters associated with an abstinence of <24 h were found to be noninferior as compared to longer ejaculatory abstinence intervals. These findings support in eliminating conservative recommendations as far as abstinence is concerned and suggest that patients may be asked to collect a semen sample on the day they present for an infertility evaluation, regardless of abstinence.
Background
Male factor infertility affects over 50% of couples when presenting for infertility evaluation. 1 The semen analysis test remains the gold standard investigation of choice for the assessment of male infertility. 2 Semen analysis though has numerous clinical and/or technical limitations. Spermogram estimates of sperm concentration, motility, and morphology in isolation do not have adequate prognostic value in predicting conception. 3 Sperm parameters of concentration, motility, and morphology also rapidly change across time, space, and geography both inter-individually and intra-individually.4–6 The complexity is understandable, since semen contains a highly heterogeneous population of spermatozoa produced over a period of 75 to 80 days. 5 The ejaculate output, at any given point of time, in a man crucially depends on the following: (1) testicular sperm production and (2) accessory gland secretion. 5 Added to these, collection issues and laboratory factors can also confound a semen analysis report. 6
Of the several known factors that influence a semen analysis report, a significant confounder to the inherent variability seen in semen analysis is the duration of ejaculatory abstinence. 7 The recommended duration of ejaculatory abstinence as per the World Health Organization (WHO) manual ranges from 2 to 7 days. 8 This recommendation is based on the well-known fact that semen parameters even for a single individual are never uniform across time. 9 Abstinence is a rough measure since its relationship would vary with seminal parameters depending on the frequency of ejaculation and also on the units that are used to measure abstinence (hours or days). 9 The basis of this 2- to 7-day ejaculatory abstinence is unclear, with no supporting references. These recommendations date back to 1999, which is almost two decades old and it is unknown as to why the WHO is recommending these intervals when all other parameters have changed. 10 Most previous studies on ejaculatory abstinence also used different subgroups of participants in their analysis, further confounding the data and conclusions.11–15
The American Urology Association 2011 best practice statement recommends 2 to 3 days of ejaculatory abstinence, 16 while the American Society for Reproductive Medicine in a 2012 report recommended 2 to 5 days of ejaculatory abstinence. 17 Both these recommendations are much shorter than the WHO guideline values. The European Society of Human Reproduction and Embryology (ESHRE) and the Nordic Association of Andrology strongly recommend a 3- to 4-day abstinence time frame. 18 A recent study by Alipour and colleagues 19 reported significantly higher sperm kinematic parameters and percentage of progressively motile sperm with a 2-h abstinence period as compared to a 4- to 7-day abstinence time frame. Another study done on 100 normozoospermic men also reported similar significant improvements in sperm kinematic parameters with a 4-h abstinence time frame as compared to 4- to 7-day abstinence. 20 Another study by Bahadur and colleagues, 21 done on 73 oligozoospermic subfertile men, in which consecutive ejaculates were assessed reported improved sperm concentration, sperm progressive motility, and morphology with a 40-min abstinence period.
The WHO 2010 guideline values for ejaculatory abstinence arise from observations made on semen parameters of normozoospermic fertile men. 22 Whether these guideline values can be applied to a population of subfertile men who present to a fertility clinic is to be conclusively proven. The exact relationship between ejaculatory abstinence and to how exactly it influences sperm concentration, motility, and morphology remains to be resolved.
With the advent of Intra-cytoplasmic injection of spermatozoa (ICSI), much greater importance is now given to sperm quality versus sperm quantity. 23 Depending on the type of fertility treatment employed, Intra-uterine insemination (IUI) or ICSI, sperm parameters have to be optimized for the best outcome. The clinical importance of ejaculatory abstinence with respect to the aforementioned treatment modalities thus remains indispensable.
Choosing the right ejaculatory abstinence time frame may help fertility clinics in optimizing the sperm quantity and quality for prospectively planned fertility treatments.
Thus, based on the existing literature and controversy surrounding ejaculatory abstinence, the aim of this study was to assess whether sperm parameters varied significantly with respect to different periods of ejaculatory abstinence in a population of normozoospermic and oligozoospermic Tamil subfertile men who were undergoing an infertility evaluation.
Materials and methods
For the study, a retrospective review of 2368 semen analysis reports (January 2013–January 2018) of men from infertile couples who presented to the clinic for an infertility evaluation was done. Of the 2368 patient records, semen reports that identified azoospermia and reports with missing entries were excluded from the data analysis. A total of 2037 semen analysis reports were included in the final analysis. The study was done in accordance with the Helsinki Declaration. The ethics committee of the institution approved the study (Ref. No.: VRRIBMS00000012). Written and informed consent was obtained from all participants. Data collected included the ejaculatory abstinence, semen volume, sperm concentration, percentage of progressively motile sperm, nonprogressive and immotile sperm, and finally percentage of sperm with normal morphology. Data on round cells, pH, debris, sperm vitality, sperm aggregation, and agglutination were all excluded, as this part of the data was not computerized for all patients. Semen parameter assessment strictly followed the 2010 WHO laboratory manual for examination and processing of human semen. 22 Semen analysis cutoffs were determined based on the 2010 WHO laboratory manual for examination and processing of human semen. A sperm concentration of ⩾15 million/ml was considered as normozoospermic. Values <15 million/ml were categorized as oligozoospermic. All patients included in the study had provided their semen samples in the clinic in a room adjacent to the andrology laboratory. Semen samples were assessed immediately after liquefaction (within 1 h of ejaculation). Semen volume was estimated by using a graduated pipette. Sperm concentration was estimated using a Neubauer counting chamber. Sperm motility analyses were performed on a 10-µl drop on a glass slide with a 22 × 22 mm cover slip and on a heated stage at 37°C, at 400× magnification with lens that had an eye piece reticle. Sperm morphology assessment was performed on Diff-Quik stained slides (Medion Diagnostics AG, Bonnestrasse 9, CH-3186 Dudingen, Switzerland). A total of 400 spermatozoa in replicate were assessed per sample by one experienced embryologist. Acceptability of differences were calculated for measured sperm parameters as per the 2010 WHO laboratory manual for examination and processing of human semen. 22
A total of 1621 reports of computerized patient records categorized as normozoospermic were then grouped on the basis of the abstinence period. The groups were as follows: ejaculatory abstinence <24 h, abstinence between 1 and 2 days, abstinence between 3 and 7 days, abstinence between 8 and 15 days, abstinence between 16 and 30 days, and last abstinence more than 30 days. Next, a total of 416 computerized patient records categorized as oligozoospermic were then grouped into a total of five abstinence groups, These were as follows: ejaculatory abstinence <24 h, abstinence between 1 and 2 days, abstinence between 3 and 7 days, abstinence between 8 and 15 days, and finally abstinence >16 days.
Statistical analysis
For statistical analysis, a p value <0.05 was considered to be statistically significant. The unpaired two-tailed t-test, combined with one-way Welch’s analysis of variance (ANOVA) and the Games–Howell multiple comparison posttest, was used. Data are presented as mean along with the standard deviation (SD) and 95% confidence interval (CI). Percentages are expressed where appropriate.
Results
In this study, a retrospective evaluation of over 2037 normozoospermic and oligozoospermic semen analysis reports was done to assess as to how ejaculatory abstinence varied between individuals with respect to semen volume, sperm concentration, percentage of progressively motile sperm, and percentage of normal sperm morphology. The mean age of men in the normozoospermic group was 32.2 (SD = 4.91), while the mean age of men in the oligozoospermic group was 33.4 (SD = 5.37).
Ejaculatory abstinence and semen volume
The mean semen volume variance among different groups of ejaculatory abstinence in the normozoospermic group was statistically significant (F = 23.1, p < 0.001). The mean semen volume per ejaculate in the normozoospermic sample group was 2.40 ml (SD = 1.33 and 95% CI = 2.34–2.46). In particular, a statistically significant increase (1.2 ml, p < 0.0001, and 95% CI = 0.502–1.898) in the mean semen volume was noticed between values of 1.36 ml (SD = 0.62) and 2.56 ml (SD = 1.25), between categories of ejaculatory abstinence <24 h and on days 3 to 7 of ejaculatory abstinence, respectively. A similar trend of a statistically significant difference was also seen between the categories of <24 h ejaculatory abstinence and both days 8 to 15 and 16 to 30. The highest mean difference in terms of semen volume (1.67, p < 0.0001, 95% CI = 0.81–2.53) was evident between <24 h abstinence and 16 to 30 days abstinence categories (Table 1). The mean semen volume difference was not statistically significant when comparing 30 days of abstinence versus abstinence <24 h (1.23, p > 0.05, 95% CI = 0.09–2.55). In terms of absolute mean differences, a progressive increase in the mean semen volume is definitely seen starting from 1 to 2 days reaching a peak at 16 to 30 days, after which mean semen volume decreases (Figure 1).
Summary of post hoc tests in normozoospermic men.

For pairwise group comparison, the Games–Howell post hoc tests were carried out . The level of statistical significance was p < 0.05. The mean semen volume was significantly different across different groups of ejaculatory abstinence. Mean semen volume progressively increased with increasing duration of abstinence. However, sperm concentration, percentage of progressively motile sperm, and percentage of normal sperm morphology showed no significant change across different ejaculatory abstinence groups. ns, not significant.
p ⩽ 0.05; ***p < 0.0001.

Semen volume variance with ejaculatory abstinence.
In the oligozoospermic group, the mean semen volume variance with different ejaculatory abstinence groups was statistically significant (W = 14.07, df = 4, 30.87, p < 0.0001). Ejaculate volume significantly increased with increasing duration of abstinence. This difference was most pronounced when comparing <24 h to 8 to 15 days (1.63 ml, p < 0.0001, 95% CI = 0.84–2.43). Higher abstinence days had higher mean values of ejaculate volume (Table 2).
Semen parameters of semen volume, sperm concentration, percentage of sperm with progressive motility, and percentage of sperm with normal morphology for oligozoospermic men across different groups of ejaculatory abstinence.
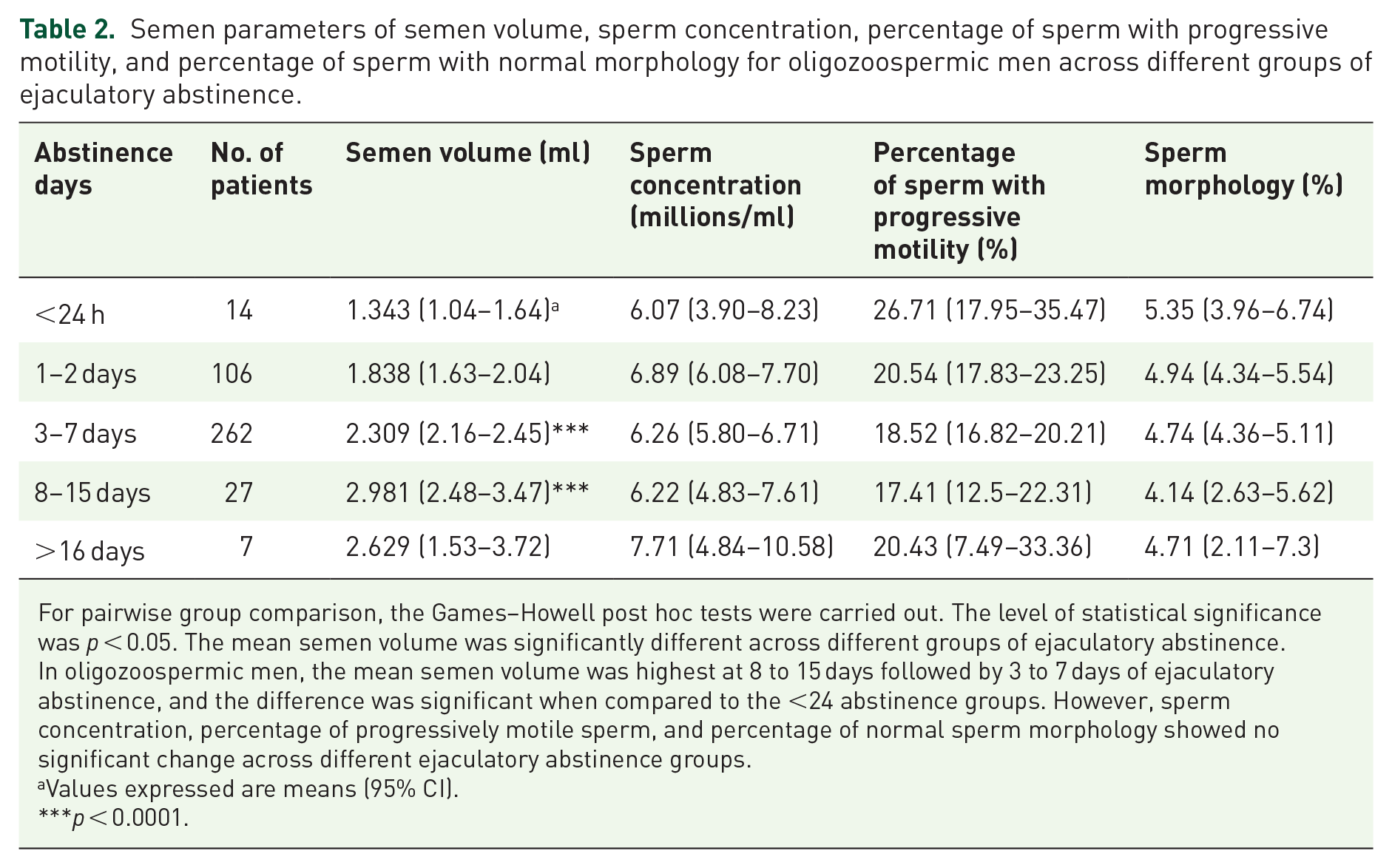
For pairwise group comparison, the Games–Howell post hoc tests were carried out. The level of statistical significance was p < 0.05. The mean semen volume was significantly different across different groups of ejaculatory abstinence. In oligozoospermic men, the mean semen volume was highest at 8 to 15 days followed by 3 to 7 days of ejaculatory abstinence, and the difference was significant when compared to the <24 abstinence groups. However, sperm concentration, percentage of progressively motile sperm, and percentage of normal sperm morphology showed no significant change across different ejaculatory abstinence groups.
Values expressed are means (95% CI).
p < 0.0001.
Ejaculatory abstinence and sperm concentration
The sperm concentration among 1621 normozoospermic sample reports ranged from 15 to 250 million/ml. The mean sperm concentration was 65.83 (SD = 36.69, and 95% CI = 62.77–66.89). Sperm concentration at an ejaculatory abstinence of <24 h showed no statistically significant difference when compared with all other ejaculatory abstinence groups. The mean sperm concentration at <24 h ejaculatory abstinence was 50.96 (SD = 38.02 and 95% CI = 35.92–66); this value of mean sperm concentration showed a reduction of 8.98 million/ml at 1 to 2 days of abstinence and 1.44 million/ml at 3 to 7 days. Both the observed differences did not reach statistical significance. At 8 to 15 days, mean sperm concentration was 65.32 million/ml (SD = 47.14 and 95% CI = 68.68–71.96) compared to 50.96 million/ml at <24 h ejaculatory abstinence; however, this difference was not statistically significant (Tables 1 and 3). Beyond 30 days, a decrease in mean sperm concentration was seen back to 56.15 million/ml, but this did not reach statistical significance (Figure 2). In the oligozoospermic group, no statistically significant changes were found in sperm concentration across different groups of ejaculatory abstinence (W = 0.765, df =4, 29.74, p = 0.5526).
Semen parameters of semen volume, sperm concentration, percentage of sperm with progressive motility, and percentage of sperm with normal morphology of normozoospermic men across different groups of ejaculatory abstinence.

CI: confidence interval.
Values expressed are means (95% CI).

Sperm concentration variance with ejaculatory abstinence.
Ejaculatory abstinence and sperm progressive motility
The percentage of sperm with progressive motility of normozoospermic samples ranged from 32% to 87%. The mean percentage of sperm with progressive motility was 47.72% (SD = 10.22 and 95% CI = 47.07–48.36). A peak mean sperm motility value of 42.37% (SD = 12.62 and 95% CI = 37.38–47.36) was observed in the ejaculatory abstinence group of <24 h. The percentage of sperm with progressive motility values showed a gradual decrease with increasing days of abstinence (Figure 3); sperm progressive motility was lowest at >30 days of ejaculatory abstinence. None of these changes observed in the sperm progressive motility reached statistical significance (Table 1).

Percentage of progressively motile sperm with ejaculatory abstinence.
An assessment of percentage of total sperm motility and its variance with ejaculatory abstinence was done. Percentage of total sperm motility showed a peak mean value of 60.33% (SD = 11.55 and 95% CI = 55.92–64.75); there was a much smaller reduction in sperm total motility at 1 to 2 days and 3 to 7 days of abstinence (Figure 4) as compared to sperm progressive motility. This change also did not reach statistical significance. A statistically significant reduction in percentage of total sperm motility values was observed at ejaculatory abstinence >30 days as compared to <24 h of ejaculatory abstinence (8.67%, p < 0.001, 95% CI = 0.77–27.31).

Sperm total motility and its variance with ejaculatory abstinence.
No statistically significant changes in the percentages of progressively motile sperm was seen in the oligozoospermic group with different intervals of ejaculatory abstinence (W = 1.322, df = 4, 29.38, p = 0.285). Of note, the <24-h abstinence group showed the highest mean percentage of progressively motile sperm 26.71% (SD = 15.17 and 95% CI = 17.95–35.7). Higher groups of ejaculatory abstinence showed lower peak mean values of motility. The differences though were not significant.
Ejaculatory abstinence and percentage of sperm with normal morphology
Percentage of sperm with normal morphology was assessed as per the WHO 2010 guidelines. Mean peak percentage of sperm with normal morphology values of 7.31% normal forms was observed at an ejaculatory abstinence of 8 to 15 days; however, when compared to <24 h ejaculatory abstinence, the difference between the values was not statistically significant (0.9%, 95% CI = 0.36–1.82). No specific trends toward an increase in the percentage of normal sperm or a decrease were observed across different groups of ejaculatory abstinence (Figure 5; also see Table 1).

Percentage of sperm with normal morphology and its variance with ejaculatory abstinence.
In the oligozoospermic group, no statistically significant difference in the percentage of normal sperm morphology was observed across different groups of ejaculatory abstinence (W = 0.4493, df = 4, 29.68.38, p = 0.774). Once again, peak mean sperm percentage of normal sperm was observed in <24-h abstinence group (M = 5.35%, SD = 2.40, 95% CI = 3.96–6.74).
Discussion
The primary aim of the study was to assess how different semen parameters vary with different intervals of ejaculatory abstinence among a group of normozoospermic and oligozoospermic Indian subfertile male population of Tamil origin . The reason this study population was chosen is because India is the world’s second largest population. 24 Moreover, about one-fifth of the total Indian population resides in the South Indian subcontinent and Tamil Nadu alone holds close to 80 million individuals (maternal, child mortality, and total fertility rates). 25 Infertility affects over 17 million couples in India as per data from the NFHS (National Family Health Survey). 26 Research in infertility from this large population has also been neglected. Infertility treatments are not subsidized and remain largely a private-sector dominated field with the government neglecting infertility both as a health problem and as a subject of research.27,28
The WHO 2010 manual did not include data from India and China in estimating the semen parameter reference value. 29 Studies have clearly established that the values of sperm concentration, motility, and morphology change from place to place and individual to individual. 29 Due to the complexity of the reproductive system and physiology that is influenced by genetics, local environment, and lifestyle factors, it would be ideal whether semen analysis reference values could be individualized depending on the country and/or a specific geography.
Thus, the findings of this study could be the first small step in trying to establish a recommendation for abstinence tailored specifically for the Indian subfertile male population of Tamil origin. Previous studies on ejaculatory abstinence and its impact on semen parameters had similar findings to this study.30,31
Levitas and colleagues 30 reported that in their retrospective analysis of over 5983 normozoospermic samples, a significant decrease in the percentage of sperm motility and normal morphology was seen on days 11 to 14 of ejaculatory abstinence. The findings of this study reported that among patients with male factor infertility, mean sperm motility, morphology, and the total number of motile sperm in the ejaculate were better with shorter durations of ejaculatory abstinence and all the changes reached statistical significance. Keihani and colleagues 31 in their retrospective analysis of 9840 semen samples had identified that semen volume, sperm concentration, and sperm motility increased with increasing duration of abstinence, while sperm progressive motility and morphology also showed a decrease with increasing duration of ejaculatory abstinence.
Both the aforementioned studies had strongly recommended a shorter duration of ejaculatory abstinence versus the current WHO recommendations of 2 to 7 days.30,31 The findings of this study are similar but with some notable differences. This study’s findings indicate that abstinence only affects semen volume from a statistically significant viewpoint in both normozoospermic and oligozoospermic individuals. With increasing duration of ejaculatory abstinence, semen volume also increased. All other parameters of sperm concentration, percentage of progressively motile sperm and percentage of sperm with normal morphology, showed no major statistically significant change across different groups of ejaculatory abstinence intervals. This finding was observed in both normozoospermic and oligozoospermic groups. Interestingly, the best combination of semen parameters (excluding volume), that is, in terms of sperm concentration and percentage of progressive motile sperm, was seen with patients who had an abstinence time frame of <24 h. In the oligozoospermic group of our study, the <24-h abstinence group showed the highest mean values of sperm concentration, motility, and normal morphology. Absolutely no statistically significant difference was seen in all the semen parameters assessed excluding semen volume in both normozoospermic and oligozoospermic groups. On an interesting note, in both 1 to 2 days and 3 to 7 days of ejaculatory abstinence, sperm progressive motility, total motility, and sperm concentration were lower as compared to the <24 h of ejaculatory abstinence. This is in stark contrast to all previous published studies and professional society recommendations.
The finding of this current study was similar to the findings of Mayorga-Torres and colleagues, 32 whose study data reported that with shorter abstinence, most of the semen parameter values are still within the WHO 2010 semen analysis normal reference ranges. This study’s findings also identified that for patients who had an ejaculatory abstinence of <24 h, all semen parameter values were well within the WHO 2010 semen analysis guideline values for the normozoospermic group. The current study’s large size enables detecting subtle differences in concentration, motility, and/or morphology that could have reached statistical significance.
Our study’s findings suggest that abstinence time might not have adequate clinical impact on semen parameters of both normozoospermic and oligozoospermic men.
Based on these study findings, the following recommendations are suggested:
Ejaculatory abstinence prior to a semen analysis is highly arbitrary, and thus patients could be asked to give a semen sample at the time of visiting a fertility clinic, regardless of their last sexual contact as opposed to a stipulated interval of 2 to 7 days as per WHO guidelines.
The findings of this study indicate that the WHO proposed 2- to 7-day period of ejaculatory abstinence cannot or need not be generalized and/or applied to all populations, as these findings based on Indian subfertile male population of Tamil origin report that <24 h of ejaculatory abstinence was not inferior in terms of semen parameters versus all other periods of abstinence . In both oligozoospermic and normozoospermic men, strict recommendations of abstinence can be liberalized. This will be of great benefit to the patient.
By not prescribing a specified duration of abstinence, a significant saving is done for the patient in terms of costs, travel, and loss of wages, and this recommendation is more apt for developing countries like India.
This study, however, is not without its limitations. One previous study again reported no difference with increasing the duration of ejaculatory abstinence in this subpopulation of participants who are oligozoospermic. 31 The oligozoospermic group in this study, which had 416 participants, reports similar findings. Whether the same finding can be applied to the heterogeneous Indian male factor infertility patients has to be independently evaluated.
In one study, Gosálvez and colleagues 33 reported a 48% reduction in sperm DNA fragmentation when an ejaculatory abstinence of less than 3 h was advocated. The other major limitation was that the exact duration of pre-ejaculatory sexual arousal was not taken into account for this study since, to a certain extent, this “duration” can influence sperm concentration. Most studies on ejaculatory abstinence looked at semen values from just one ejaculate, due to the practical limitations in recommending patients to give multiple samples. Just as with all previous studies in abstinence, this study could also be measuring a chance fluctuation in subjective parameters. The next limitation of this study lies in its retrospective nature. The number of patients who gave a semen sample for analysis with less than 24 h of ejaculatory abstinence was just 27 in the normozoospermic group and 14 in the oligozoospermic group. This number is significantly much lesser than all the other abstinence study groups, which had a much higher number of study participants.
Sperm concentration for a single patient measured over 120 days can range from 0 to 120 million as prominently highlighted in the WHO 2010 manual. Thus, with such a huge variation, and abstinence being an added confounder, no medical study published with the aim of improving male fertility with medications can be accurate or even reproducible as most medications given for idiopathic male infertility and claiming to improve semen parameters are probably measuring a chance fluctuation in semen parameters due to its inherent high biological variability.
As far as abstinence is concerned, a true clinically important difference in semen volume, sperm concentration, percentage of progressively motile sperm, and percentage of sperm with normal morphology was not observed with higher days of ejaculatory abstinence in both normozoospermic and oligozoospermic men. Moreover, across different groups of abstinence in normozoospermic individuals, all semen parameter values were still within the WHO-defined normal ranges.
In oligozoospermic men, in the context of Assisted Reproductive Technology (ART) advocating a shorter duration of abstinence may be highly beneficial, since sperm quality becomes more clinically important than total volume or count. 34 With longer duration of abstinence, spermatozoa of subfertile men may be more prone to oxidative stress and reactive oxygen species (ROS)–induced damage. This ROS-based damage could possibly happen in the epididymis and vasa.35,36 Furthermore, in oligozoospermic men, lower duration of ejaculatory abstinence was not associated with any detriment in semen parameters.
Conclusion
This study suggests the importance and need for several well-funded prospective studies on the various geographical and/or racial populations of both subfertile and fertile men. 36 To conclude, the findings of the current study suggest that strict sexual abstinence may not be routinely recommended for Indian subfertile male population of Tamil origin during a baseline infertility evaluation and that patients may be recommended to give a semen sample on the day of their clinical visit regardless of their abstinence period.
Footnotes
Author contributions
S.D. collected data and drafted the manuscript. N.P. and R.P. conceived the study idea and design, and also helped in drafting the manuscript. S.D., R.P., J.K., and B.P. helped in data collection and statistical analysis, and also helped equally in drafting the manuscript. All authors read and approved the final manuscript.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent for publication
Written and informed consent was obtained from all participants.
Ethics approval and consent to participate
The study was done in accordance with the Helsinki Declaration. The ethics committee of the VRR Institute approved the study (Ref. No.: VRRIBMS00000012).