
Abstract
Plain Language Summary
Children living in disadvantaged communities are disproportionately impacted by lack of access to opportunities for physical activity and nutritious food, and so are at highest risk of childhood obesity and chronic diseases later in life. Effective interventions to reduce the risk for chronic disease in vulnerable children exist but they need to be expanded to reach more children. A school-based program called A Project Promoting healthy Living for Everyone in Schools (APPLE Schools) delivers a very successful intervention to encourage healthy living and mental health to vulnerable kids from disadvantaged communities. It currently operates in more than 100 schools in western Canada (Alberta, British Columbia, Manitoba, and Northwest Territories). The program plans to expand nationally to reach more vulnerable children. To do this, we need to understand which program elements make it successful.
From annual action plans developed by 70 APPLE Schools between 2011 and 2021, we extracted health promotion activities and strategies that support these activities. Overall, we identified a comprehensive list of 17 essential components of the APPLE Schools program. In addition, we identified 55 specific activities that—if put in place—will ensure a successful expansion of this program into new schools across Canada. The most common core functions were helping students make healthy choices (enablement), showing positive examples (modeling), and teaching (education). The most common forms included building supportive school environments, forming partnerships, engaging students in delivering health promoting activities, and providing staff training. This work can also benefit other schools that can use this resource to guide their health promotion efforts to improve healthy living among their students.
Keywords
Introduction
School-based interventions that foster healthy lifestyle behaviors and mental wellness from a young age are a critical public health strategy to reduce the chronic disease burden (Fung et al., 2012). Schools are also the ideal setting for delivering health promotion interventions that tackle health inequalities (Vander Ploeg, Maximova, et al., 2014). Therefore, school-based health promotion interventions with local evidence of effectiveness need to be scaled up to maximize their benefits. The World Health Organization advocates for health promoting schools (HPS) interventions to be implemented in each school, given their demonstrated effectiveness in improving children's health and well-being and academic outcomes, as well as cost-effectiveness and high return on investment (World Health Organization and the United Nations Educational, Scientific and Cultural Organization, 2021).
However, HPS interventions might be difficult to implement, sustain, and adapt to new contexts (Craig et al., 2008). Unlike discrete school-based interventions (e.g., installing water fountains or hydration stations or extending a physical activity break by 10 min), HPS interventions are complex: they include a wide range of intersectoral, multistakeholder, and multicomponent actions (or intervention activities) that aim to improve lifestyle behaviors and health of students and school staff, with most of these actions requiring at least several approaches (or implementation strategies) to adopt, integrate, and sustain them (Domitrovich et al., 2008; McIsaac et al., 2017; Moore et al., 2017; Ozer, 2006). Moreover, HPS intervention activities and implementation strategies must be tailored to each school's unique context, existing assets, and other contextual determinants of HPS implementation outcomes. A well-documented example of a successful HPS intervention currently operating in more than 100 elementary schools in several provinces and territories across Canada is A Project Promoting healthy Living for Everyone in Schools (APPLE Schools), an innovative, not-for-profit HPS intervention targeting elementary schools in socioeconomically disadvantaged settings.
APPLE Schools is internationally recognized as an evidence-based best practice for school health by the National Institute of Health/National Cancer Institute (National Cancer Institute, 2020), and as one of the world's 100 most innovative and inspiring education projects by a global nongovernmental organization HundrED (HundrED, 2019). In a series of quasi-experimental, pre–post trials with a parallel nonequivalent control group, the APPLE Schools intervention has been shown to be effective, with APPLE Schools students developing better nutrition habits, becoming 35% more physically active in/outside of school and 40% more likely to have a healthy weight (Bastian et al., 2015; Maximova et al., 2015; Roberts et al., 2016; Tran et al., 2014; Vander Ploeg et al., 2012; Vander Ploeg, McGavock, et al., 2014). The evidence also documents reductions in health inequalities: while all students benefit from the intervention, those most in need (i.e., most disadvantaged) benefit the most (Bastian et al., 2015; Vander Ploeg, Maximova, et al., 2014). Over 2 years, school averages of student lifestyle behaviors improved to approximate provincial levels (Bastian et al., 2015; Vander Ploeg, Maximova, et al., 2014). Moreover, this intervention was shown to be cost-effective (Ekwaru et al., 2017), with an astounding return on investment of 860% (i.e., every $1 invested avoids $8.6 in future direct and indirect costs associated with chronic diseases; Ekwaru et al., 2021).
APPLE Schools was inspired by and modeled after the grassroots initiative called Annapolis Valley Health Promoting Schools (AVHPS), implemented in Nova Scotia in 1997 (Veugelers & Fitzgerald, 2005). The efforts to transfer the AVHPS intervention to schools in Alberta were informed by multiple training sessions, with the AVHPS team sharing experience implementing the intervention in Nova Scotia and thoughts on tailoring it to the Albertan context (Fung et al., 2012). Since its launch in 2008 in 10 schools in Alberta, this research evidence enabled APPLE Schools to scale up its operations to over 100 schools in Canada, now serving more than 33,000 children annually. Efforts are underway to scale it up to 200 schools in disadvantaged settings in the coming years and reach over 60,000 students annually.
To support these efforts and ensure implementation fidelity, which is crucial to maximizing the intervention's effectiveness and sustainability in new contexts, it is imperative to discern core functions (i.e., basic purposes, mechanisms and theoretical principles that fundamentally define the intervention and drive its effectiveness) and forms (i.e., specific content and delivery strategies implemented to achieve core functions; Jolles et al., 2019) of APPLE Schools intervention activities and implementation strategies. Indeed, clearly outlining which elements should be retained (i.e., core functions) and which ones can be tailored to the local context and needs (i.e., forms) is recognized as one of the essential determinants of a successful scale-up (Gesell et al., 2021; Hawe et al., 2004). This approach is particularly suited for the APPLE Schools intervention, shown to produce differential effect across schools and students (with disadvantaged schools and students benefiting the most) and requiring tailoring of its intervention activities and implementation strategies to each school's unique context. To our knowledge, only a few studies attempted to specify core functions and forms of complex interventions (Byng et al., 2008; Fianu et al., 2017; Hill et al., 2020; Jolles et al., 2019; Kirk et al., 2021; McNeal et al., 2022; Villeval et al., 2016, 2019; Wahlen et al., 2022), but they focused predominantly on healthcare interventions in clinical settings. Only one (Villeval et al., 2019) aimed to unpack the core functions and forms of a school-based health promotion intervention targeting nutrition and physical activity education. Further, none of the studies identified core functions and forms of both interventional aspects—intervention activities and implementation strategies. In this study, we aimed to build matrices of core functions and forms of APPLE Schools’ intervention activities and implementation strategies to inform the transfer of this intervention to schools across other Canadian provinces and territories.
Methods
The APPLE Schools Intervention
Grounded in the HPS approach, APPLE Schools aims to promote healthy lifestyle behaviors and mental health and well-being by transforming the culture of school communities to one where “the healthy choice is the easy choice” (Fung et al., 2012). APPLE Schools implements the HPS approach by delivering harmonized actions on four distinct but interrelated pillars (i.e., social and physical environment; teaching and learning; policy; and partnerships and services) to help school communities build capacity and students to take greater ownership of their own health (Pan-Canadian Joint Consortium for School Health, 2016). Recognizing the unique context in which each school functions, the APPLE Schools intervention is tailored to each school's needs and priorities. As such, there is no predetermined set of intervention activities and implementation strategies to be found in every APPLE School (which would be the case if the intervention followed a one-size-fits-all approach, previously shown to be largely ineffective in producing the desired effect, Powell et al., 2017).
To tailor the intervention to each school's needs and facilitate implementation, APPLE Schools places a school health facilitator (SHF) in each school who works closely with students, families, school staff, local business and community partners to collaboratively identify health promotion goals and implement health promotion activities. SHFs provide hands-on, full-time support over the first 2–3 years, after which a volunteer teacher mentored through APPLE Schools’ central office and called a school health champion (SHC) becomes the key person to maintain the HPS culture in the school.
Analytical Approach
To develop matrices of core functions and forms of APPLE Schools intervention activities and implementation strategies, the analytical approach included the following steps: (a) extracting all activities documented in APPLE Schools annual action plans; (b) classifying extracted activities into intervention activities and implementation strategies using manual and machine learning (ML) approaches; (c) mapping intervention activities and implementation strategies onto two sets of theory-informed core functions; and (d) grouping intervention activities and implementation strategies within each core function into forms using thematic analysis.
Extracting Activities From APPLE Schools Annual Action Plans
Between 2011 and 2021, APPLE Schools was operating in 70 schools. The SHFs and SHCs in these schools, under the guidance of APPLE Schools mentors, prepared a total of 555 annual action plans, which documented goals, objectives, and what and how health promotion-related activities were implemented. Action plans, particularly in the early years, did not follow a structured format; therefore, their organization and richness of captured information vary between schools. To prioritize action plans most likely to yield rich information, we rated them according to the level of detail provided, readability and comprehension, and whether they had been updated throughout the school year. The total score ranged from 0 to 3, with higher scores indicating better quality and richness of action plans (see Supplemental Material 1). Those rated lower than 3 (n = 364) were excluded (see Figure 1).

Flowchart of Data Collection.
From the 191 action plans with a total score of three, 5,301 activities were extracted using a data extraction form, pilot-tested by two researchers (JK and BM). For each activity, the form captured the following information: goals and objectives, name (e.g., Smoothie Day, Taste Testing, Hoop Dance), how and by whom it was delivered (e.g., “Teacher brought her own fruit [crab apples] from her own garden”), whether students were involved in planning and delivery (e.g., “Student leaders planted and tend to flowers and vegetables [in the school garden]”), frequency of delivery (e.g., throughout the year, once a year, every month, every day), when it was delivered (e.g., throughout school year, fall, winter, spring), target audience (e.g., all grades, specific grades, school staff), as well as details about any adaptations made and justification for these changes (e.g., “Changes for the few months of cold weather: The student leaders will go to assigned classes and have the students participate in ‘Just Dance’ [indoors, as opposed to going to an outdoor playground]”). To obtain a sample of unique activities for analysis, repeat activities in the same school and activities that were planned but not delivered were excluded (n = 2618).
Classifying Activities into Intervention Activities and Implementation Strategies
The large number of unique activities retained for analyses (n = 2683) required employment of supervised ML methods, commonly used in sentiment analysis research (Geethangili & Suresh, 2022; Nasteski, 2017; Osisanwo et al., 2017), to maximize the efficiency and utility of all data available (as opposed to manually coding and analyzing only a subset of activities). First, JK and BM labeled (or manually classified) a subset of 1200 (45%) randomly selected activities as either intervention activities (i.e., what was implemented) or implementation strategies (i.e., how—or using which strategies or techniques—intervention activities were implemented). Of these 1,200 manually classified activities, a subset of 600 activities, along with the labels assigned by JK and BM, was used to train two ML algorithms to recognize text patterns associated with intervention activities and implementation strategies. Since ML algorithms require text to be processed and simplified, text of each activity was tokenized: phrases were split into individual words, which were reduced to their root stem (e.g., “running” was reduced to its root stem “run”) to enable cross-comparison across activities. Word vectors for each activity were created using the Term Frequency-Inverse Document Frequency approach, which considers the frequency of each word within each activity against its frequency in the entire sample of activities (for a detailed explanation of this approach, see Geethangili & Suresh, 2022; Li & Ou, 2021). Once the text was processed, ML algorithms used the k-Nearest Neighbors algorithm with k = 5 and Euclidean distance measures to classify activities according to the most common category among each activity's five nearest neighbors in the labeled training set (Dey et al., 2016).
Two ML algorithms (one trained to predict the likelihood of each activity being classified as an intervention activity and another one trained to predict the likelihood of each activity being classified as an implementation strategy) were applied to the remaining 600 activities within the training set, but no labels assigned by researchers were provided. ML classification of each activity as an intervention activity vs. implementation strategy was validated against labels assigned by researchers (JK, BM) in order to verify each algorithm's predictive performance (Stevens et al., 2020). ML models attained class precision and recall >80% for true positives, which was deemed sufficient to proceed, given that the subsequent two steps (i.e., mapping intervention activities and implementation strategies to their core functions and grouping activities into forms) involved analyses done by the researchers. The remaining unlabeled 1,483 activities were classified by ML algorithms only. ML models were ran using RapidMiner version 10.1 (rapidminer.com).
Of 2,683 extracted activities, 300 contained information pertaining to intervention activities and implementation strategies. For example, one of the extracted activities was “Spring Walk Day: [date]. Grade 3 students planned and implemented the event. We wore the T-shirts from [local community organization - blinded] and ended the walk with the Zumba party.”). This activity contains information on both the “what” (i.e., Spring Walk Day, Zumba party) and the “how” (i.e., the intervention activity was planned and implemented by Grade 3 students); therefore, the first part was classified as an intervention activity, and the second part—as an implementation strategy. The majority of extracted activities were labeled as intervention activities (n = 2,066), and fewer than half were labeled as implementation strategies (n = 1,217).
Mapping Intervention Activities and Implementation Strategies onto Their Core Functions
Nearly one-third of activities classified in the previous step as intervention activities (n = 685) and implementation strategies (n = 405) were randomly selected for mapping onto core functions. Core functions of intervention activities were drawn from the Behavior Change Wheel (BCW; Michie et al., 2011), considering a comprehensive range of interventions it captures and its appreciation of the broader social and physical contexts within which individual behavioral change occurs. Core functions of implementation strategies were drawn from the implementation components of HPS outlined by Rowling and Samdal (2011; see Table 1). JD and CH mapped intervention activities and implementation strategies to their core functions: in 60% and 82% of cases, intervention activities and implementation strategies were assigned by JD and CH to the same core function, respectively. Disagreements were discussed and resolved by the two reviewers.
Framework for Mapping Forms onto Core Functions of APPLE Schools Intervention Activities and Implementation Strategies.

Note. APPLE Schools = A Project Promoting healthy Living for Everyone Schools.
Grouping Intervention Activities and Implementation Strategies into Forms Within Their Core Functions
To our knowledge, there are no established frameworks that would capture forms of intervention activities. Regarding the forms of implementation strategies, the School Implementation Strategies, Translating ERIC Resources (SISTER) framework (Cook et al., 2019) outlines implementation strategies in school-based interventions. However, most SISTER implementation strategies occur outside of the inner setting and/or pertain to the exploration and preparation phases of intervention implementation (see Aarons et al., 2011), which are unlikely to be captured in APPLE Schools action plans. Therefore, we relied on a reflexive thematic analysis (Braun & Clarke, 2019), positioned within a constructive perspective, to help identify forms for intervention activities and implementation strategies documented in APPLE Schools action plans. First, JK read all activities included in action plans during data extraction and generated initial descriptive codes for activities within each function. JK and JD discussed and modified these codes, and generated overarching themes, which were continuously revised. To quantify the frequency of core functions in 70 APPLE Schools, we calculated the proportion of schools that documented each function in their action plans.
Results
In thematic analysis, we identified 55 forms across 17 core functions of intervention activities and implementation strategies (see Tables 2 and 3, respectively). Both matrices include core functions, the proportion of schools that addressed each function, their forms, and activity examples with direct quotes from action plans. For intervention activities, we also captured the target of each form: physical activity, healthy eating, mental health, school connectedness, staff health and wellbeing, physical environment, family and community involvement, and cultural connection.
Forms and Functions Matrix of APPLE Schools Intervention Activities.

Note. APPLE Schools =A Project Promoting healthy Living for Everyone Schools; HPS: health promoting schools; DPA: daily physical activity; PALs: playground activity leaders; SHF: school health facilitator.
Forms and Functions Matrix of APPLE Schools Implementation Strategies.
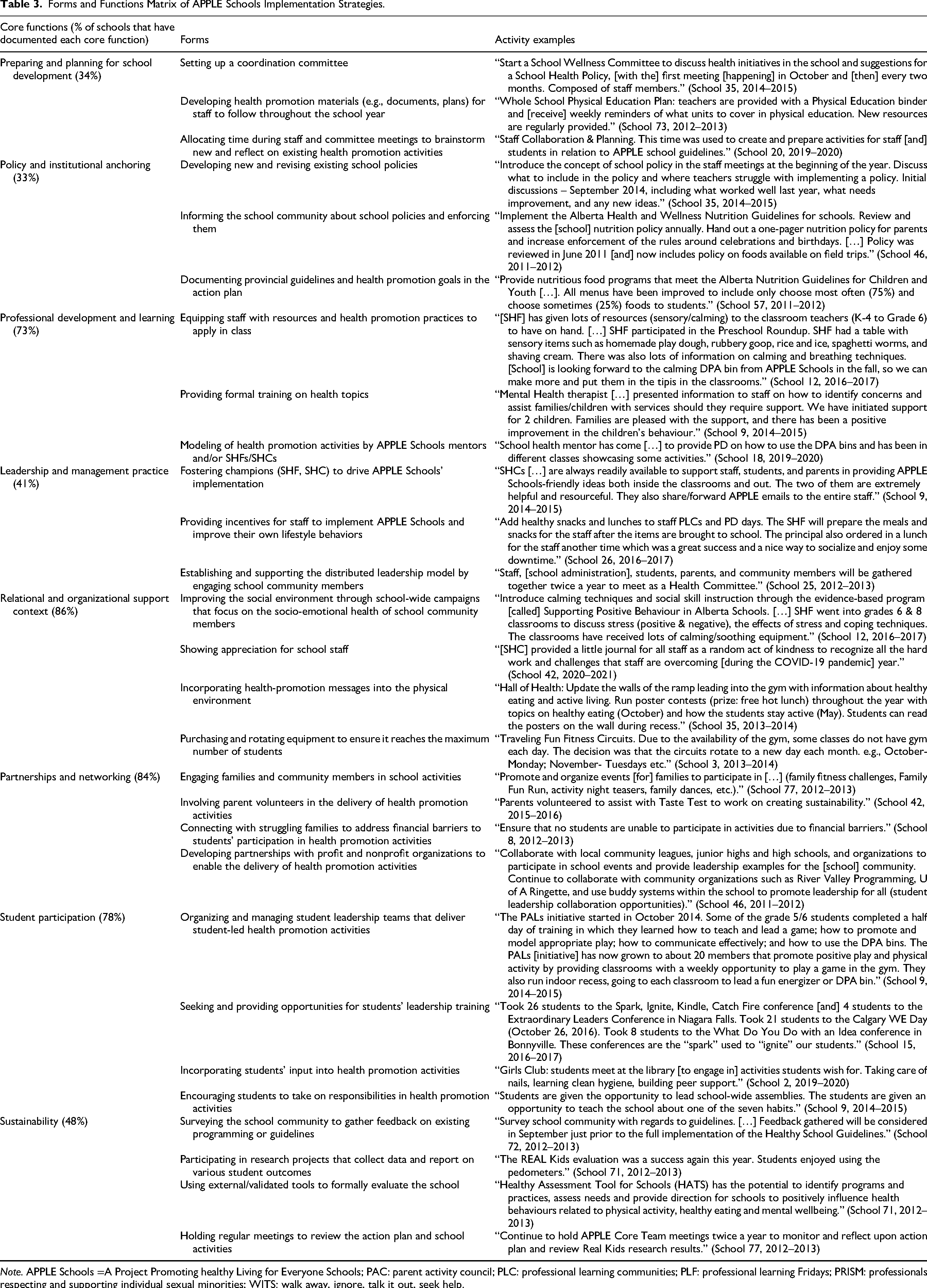
Note. APPLE Schools =A Project Promoting healthy Living for Everyone Schools; PAC: parent activity council; PLC: professional learning communities; PLF: professional learning Fridays; PRISM: professionals respecting and supporting individual sexual minorities; WITS: walk away, ignore, talk it out, seek help.
Core Functions and Forms of Intervention Activities
The most commonly addressed core functions were enablement (96%), modeling (66%), and education (54%), while others were addressed in fewer than half of the schools: persuasion (42%), training (40%), environmental restructuring (31%), restriction (27%), and incentivization (12%). None of the implemented forms were mapped to the coercion function.
Enablement was fulfilled not only by almost all APPLE Schools but also through a greater variety of forms, compared to other functions. The forms were implemented to benefit different members of school communities (e.g., students, families, school staff) and aimed at all but one target (forms related to the physical environment were mapped to environmental restructuring). The education function was fulfilled by staff-led activities aimed at educating students about healthy lifestyle behaviors and mental health and well-being. Efforts were also made to educate families about health promotion to ensure consistency of health promotion messages between the school and home settings. Two related functions of modeling and training were addressed by exposing students to new foods through taste testing and alternative ways of staying physically active, and through teaching students cooking and food preparation skills and providing hands-on gardening experiences, respectively. Importantly, targeted activities to reinforce the principles of equity, diversity, inclusion, and accessibility (EDIA; e.g., asking students to bring traditional dishes) have also been documented, particularly in recent years when the EDIA principles became an integral part of school curricula. The rest of the functions (i.e., restriction, incentivization, environmental restructuring, and persuasion) were addressed by a limited number of forms.
Core Functions and Forms of Implementation Strategies
The following four core functions of implementation strategies were addressed in most schools: relational and organizational support context (86%), partnerships and networking (84%), student participation (78%), and professional development and learning (73%), while others were addressed in fewer than half of the schools (range: 33–48%).
Fostering champions in schools—SHFs or SHCs, depending on the school's stage in APPLE Schools—was central to ensuring the leadership function. SHFs and SHCs were the driving force behind implementing most of the forms mapped to this and other core functions. Another crucial implementation strategy was setting up coordination committees that varied in composition (e.g., staff, students, parents) and met on a regular basis to review schools’ action plans, discuss funding and activities, and map existing assets (preparing and planning). School relational and organizational support context was addressed through forms aimed at improving the social and physical environments. Anchoring the HPS principles in school (policy and institutional anchoring) was done through developing new and revising existing school policies (i.e., formal policies), often with the input of various stakeholders, and informing school community members about these policies to facilitate adherence to them. In the absence of formal school policies, some schools used provincial/territorial guidelines to inform their health promotion activities. Forms addressing the partnerships and networking function centered around engaging parents as participants and/or partners in delivering health promotion activities and developing new or strengthening existing partnerships with community organizations. Some schools formed student leadership teams (e.g., Student Wellness Action Team, Physical Activity Leaders), comprised of students with formal leadership training, to oversee forms mapped to student participation and encourage students to play an active role in the planning and delivery of health promotion activities. To increase school staff's competency in delivering health promotion activities and fulfill the professional development and learning function, staff were provided with resources on health-related topics and given opportunities to participate in formal training or witness APPLE Schools mentors and/or SHFs/SHCs delivering health promotion activities. Finally, gathering feedback on existing programming and/or guidelines, collecting data on various student outcomes, and formally evaluating the school's HPS-related outcomes were often used to address the sustainability function. Data emerging from these activities were often shared with the broader school community.
Discussion
While specifying matrices of core functions and forms of various interventions is becoming more common in implementation science and practice (Byng et al., 2008; Fianu et al., 2017; Hill et al., 2020; Jolles et al., 2019; Kirk et al., 2021; McNeal et al., 2022; Villeval et al., 2016, 2019; Wahlen et al., 2022), there is a lack of studies that would also attempt to disentangle the “what” and “how to” aspects of interventions. This study aimed to close this gap by leveraging over 10 years of health promotion activities, delivered and recorded in 555 annual action plans in 70 APPLE Schools, to derive a list of 17 core functions and 55 forms of specific actions that comprise the APPLE Schools intervention (“what” or intervention activities) and techniques used to bring about its implementation outcomes (“how to” or implementation strategies). Below, we discuss study's results and their practical implications, its strengths and limitations, and reflect on the methodological approach we employed and directions for future research.
While keeping in mind that the number of core functions was predetermined by the theoretical frameworks chosen to guide this study, only a few core functions of intervention activities (i.e., enablement, modeling, education) and implementation strategies (i.e., relational and organizational support context, partnerships and networking, student participation, and professional development and learning) were documented in more than half of the schools. A wide range of forms was implemented to fulfill core functions, with a greater number and variety of forms mapped to these most commonly documented core functions.
The core function of intervention activities that stands out in that it was addressed almost universally (in 64 out of 67 schools) was enablement, with most of its forms aiming to improve student physical activity and healthy eating. This finding aligns with the philosophy (i.e., “making the healthy choice the easy choice”) and historical emphasis of the HPS approach on promoting “healthy eating and active living” (Veugelers & Schwartz, 2010). Albeit to a lesser degree, modeling and education functions were also commonly addressed. Forms implemented to fulfill the modeling function reflected continuous efforts of APPLE Schools SHFs and SHCs to introduce new foods (e.g., Taste Testing) and activities (e.g., Zumba fitness classes) to complement traditional health education approaches and make these activities more accessible to those students who might not get exposed to them outside of school. These activities often required establishing new or tapping into existing partnerships with community organizations. The finding that the education function was commonly implemented is consistent with the results reported by Villeval et al. (2019) and is to be expected since its forms may be easier for school staff to integrate into the school curriculum which already has health education as an essential component.
The aforementioned core functions require concurrent systemic changes to the school's physical environment (Bartelink et al., 2022; Leger et al., 2007), which is why one of the HPS pillars in the original framework is “the school physical environment” (World Health Organization, 1996). Changes to the school building, grounds, spaces, and equipment serve as tangible expressions of the broader organizational support context (Guldager et al., 2018). However, modifying the physical environment requires considerable financial investments, which might not be readily available in APPLE Schools, most of which are located in socioeconomically deprived areas. This could explain why environmental restructuring was one of the rarely documented core functions. Others included restriction and incentivization, reported in 27% and 12% of schools, respectively, with no forms falling under the coercion function.
It is worth noting that most of the forms of intervention activities were aimed at the student body. The lack of documented forms targeting staff health and lifestyle behaviors could be due to students often being perceived as the main (and sometimes the sole) target audience in school-based health promotion interventions. Nevertheless, staff wellbeing is essential to the effectiveness of the HPS interventions. Therefore, designing and implementing forms that target lifestyle behaviors of school community members other than students would support creating a positive social environment that promotes the social, emotional, cognitive, and physical wellbeing of students (Braun et al., 2020; Granziera et al., 2023). Finally, involving families in school-based health promotion activities, whether as participants or active deliverers, is crucial to ensuring consistent health promotion messages in the school and home settings but is challenging due to parents grappling with competing priorities. This calls for schools and school-based health promotion initiatives to actively devise new strategies or adapt existing ones (Centers for Disease Control and Prevention, 2019a, 2019b) to engage family and community in HPS and sustain their involvement.
Similarly to core functions of intervention activities, core functions of implementation strategies addressed in most schools were those commonly emphasized as crucial to the successful HPS implementation (e.g., relational and organizational support context, partnerships and networking, student participation, professional development and learning). Ideally, all core functions of implementation strategies should be addressed as they serve as key enablers of intervention activities and major determinants of intervention's implementation outcomes. While some interventions may be successfully delivered by using only one implementation strategy (e.g., providing training on new guidelines), complex interventions such as APPLE Schools often require multifaceted implementation strategies, and each implementation strategy can be viewed as an intervention on its own (Proctor et al., 2013). Therefore, our finding that fewer extracted activities were classified as implementation strategies compared to intervention activities (n = 1217 vs. 2066)—which could in part explain why they were mapped onto fewer core functions—should not be interpreted as implementation strategies receiving less attention than intervention activities during the APPLE Schools implementation. APPLE Schools is an established intervention that encompasses activities across all intervention phases (i.e., exploration, adoption/preparation, implementation, sustainment, Aarons et al., 2011), but since school-specific action plans are written and used during the implementation and sustainment phases, they do not fully capture activities delivered by the APPLE Schools central office during the first two phases.
For example, implementation strategies related to planning were documented in 34% of schools. Notwithstanding, preparing and reviewing the action plan itself is an act of planning, and APPLE Schools mentors meet with SHFs and SHCs to review their action plan at least twice during the school year to encourage schools to plan, adapt, and improve their health promotion programming. This underscores the importance of relying on multiple sources of information (e.g., in-depth interviews with APPLE Schools mentors, SHFs/SHCs, school administrators) in order to capture the full breadth of implementation strategies. More work is needed to document a comprehensive set of implementation strategies, identify the ones that APPLE Schools SHFs and SHCs perceive to be the most feasible and effective, and, similar to Moore et al. (2021), map them onto the SISTER framework (Cook et al., 2019), which covers implementation strategies across all four intervention stages.
In addition, specifying each implementation strategy according to the prerequisites outlined by Proctor et al. (2013; i.e., in terms of the actor, action, action target, temporality, dose, and implementation outcome affected; and providing justification for a specific strategy and detailed guide on how to use each strategy and keep track of its utilization) would increase the practical value of this work. For example, the implementation strategy “Developing new and revising existing school policies” could be further refined by specifying that it is APPLE Schools central office, in collaboration with school divisions, (actors) that should develop new and revise school policies (action). This strategy should be directed at school staff to improve their knowledge of school policies (target). This is an ongoing implementation strategy, since policies should be revised on an ongoing basis (temporality and dose), which aims at ensuring the intervention's sustainability (implementation outcome). Systems thinking and complex adaptive systems provide the theoretical justification for this implementation strategy, as altering school policies was shown to foster a culture that promotes healthy behaviors, supports mental well-being, and encourages physical activity (Rosas, 2017).
However, specifying implementation strategies according to prerequisites outlined in Proctor et al. (2013) was not feasible in this study since the list of implementation strategies was derived from activities documented in action plans. Indeed, the process of specifying each strategy might benefit from a consensus-building process (e.g., Delphi), which merits a separate study. Future research could also link all implementation strategies to barriers and facilitators to the implementation and sustainment of HPS interventions (e.g., using the CFIR 2.0 framework, Damschroder et al., 2022) to understand which implementation determinants are particularly vital to implementation success (Larson & Cook, 2023).
Strengths and Limitations
There are several considerable strengths of this study. First, we used an inventory of 191 action plans, completed for a large number of APPLE Schools in socioeconomically deprived areas in both urban and rural settings. This comprehensive inventory of action plans yielded rich data of more than 2,000 unique activities, which we used to derive a list of 55 forms of intervention activities and implementation strategies and mapped them onto their theory-informed core functions. Another strength is that this study further advances the approach taken by Villeval et al. (2019) by teasing apart APPLE Schools’ intervention activities and implementation strategies. Moreover, this study demonstrates how manual text classification can be successfully supplemented by ML methods. In our experience, supervised ML algorithms achieved high class precision and recall (>80%) in identifying the “what” and “how to” aspects of the APPLE Schools intervention. The application of ML methods in public health and health promotion research remains limited despite becoming increasingly common in healthcare research (Tricco et al., 2023). This study demonstrates that supervised ML algorithms can help tease apart complex aspects of interventions and therefore have a place in the toolbox of implementation scientists. Moreover, since the commencement of this study, artificial intelligence (AI) technology has been introduced and can serve as a powerful tool that could be leveraged by implementation scientists (Trinkley et al., 2024).
Several limitations are worth noting. Given that the APPLE Schools intervention has evolved since its inception in 2008, some of the recently introduced intervention activities might be underrepresented. For example, there were fewer than expected forms targeting mental health and wellbeing, school connectedness, and cultural connection. In response to worrisome trends in mental health and well-being of children and adolescents (Gohari et al., 2024) and a well-recognized need to foster connectedness within communities to battle social isolation and loneliness (Statistics Canada, 2021), APPLE Schools’ programming was enhanced in 2017 to include mental health and well-being as one of its priority areas (Annual Reports—APPLE Schools, n.d.). Therefore, we expect activities related to mental health and well-being to become more consistently documented in the coming years.
In addition, action plans written in the early years of the APPLE Schools intervention did not have a predetermined structure as to what information should be captured and at what level of detail. To circumvent this limitation, we classified action plans in terms of the comprehensiveness of data that could be extracted from them and limited data extraction to action plans deemed “high quality” (i.e., complete and well-written). Finally, while there is no existing framework that outlines the core functions of HPS interventions, we utilized the BCW framework given the comprehensive list of interventions it offers and its explicit acknowledgement that individual behavior changes occur within a complex context and arise from combinations of different components of the behavior system. Results of this study may inform the refinement of existing frameworks and development of new frameworks that are better aligned with the HPS approach.
Given the holistic and complex nature of HPS interventions, which require the coordinated implementation of multiple interrelated activities across several pillars, we did not attempt to isolate the individual contributions of specific forms or core functions to producing implementation and/or intervention outcomes. Liu et al. (2019), in their systematic review and meta-analysis of school-based obesity prevention interventions, found that individual components of multicomponent interventions may demonstrate limited effectiveness when assessed in isolation, despite the overall intervention being effective. This phenomenon may be explained by mechanisms such as accumulation, amplification, facilitation, cascade, or convergence (Weiner et al., 2012), through which individual components interact synergistically to produce implementation and/or intervention outcomes.
Nonetheless, several forms and core functions of intervention activities and implementation strategies identified in this study—when delivered as stand-alone, single-component interventions—have been previously shown to improve children's lifestyle behaviors. For example, Jacob et al. (2021) showed that health promotion education (aligned with the education function in this article) resulted in a shift toward healthier body mass index levels in adolescents aged 10–19 years. Bikomeye et al. (2021) found that schoolyard greening (an example of the environmental restructuring function) positively influenced children's physical activity and mood. Likewise, Wang et al. (2025) demonstrated that providing opportunities for physical activity through daily physical education, structured outdoor play, and access to sports facilities (an example of the enablement function) increased adolescent physical activity levels. We acknowledge that identifying high-impact forms and/or core functions might help refine the HPS approach. However, effects of individual forms and/or core functions need to be considered in the context of other components that comprise the HPS interventions and—through various mechanisms of actions—produce implementation and intervention outcomes.
Conclusion
In this study, we developed matrices of core functions and forms for documented intervention activities and implementation strategies of the successful HPS intervention called APPLE Schools. These matrices provide a roadmap for scaling up this intervention to new settings and can serve as a useful resource for school administrators and school health practitioners working on implementing HPS interventions in schools. Current work is underway to identify systematic and proactive cultural adaptations made to APPLE Schools intervention activities and implementation strategies over the years. These adaptations will further help improve the fit of the APPLE Schools intervention for racially and ethnically diverse disadvantaged communities during scale-up. Additionally, this work informs the development of AI-powered tools that can provide schools with tailored, real-time support for effective implementation and sustainment of HPS interventions.
Supplemental Material
sj-docx-1-irp-10.1177_26334895251385936 - Supplemental material for Intervention Activities and Implementation Strategies for School-Based Health Promotion: Identifying Core Functions and Forms to Facilitate Scale-up of an Effective Intervention
Supplemental material, sj-docx-1-irp-10.1177_26334895251385936 for Intervention Activities and Implementation Strategies for School-Based Health Promotion: Identifying Core Functions and Forms to Facilitate Scale-up of an Effective Intervention by Julia Dabravolskaj, Jodi Kalubi, Julia Moore, Boshra A. Mandour, Camila Honorato, Paul J. Veugelers and Katerina Maximova in Implementation Research and Practice
Footnotes
List of Abbreviations
Acknowledgements
The authors also like to thank APPLE Schools for sharing their action plans to facilitate this research.
ORCID iDs
Ethical Consideration
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Authors’ Contributions
JK, JD, JM, KM, and PJV designed the project and data analysis plan. JK led the analyses, and BAM, CH, and JD assisted with coding and thematic analyses. All authors discussed the results and contributed to interpretation. JD and JK lead the drafting and revising of the manuscript, with KM and PJV providing critical feedback. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets used and/or analyzed during the current study are not available as supplementary file due to their volume but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.