
Abstract
Background
Clinicians need supports beyond training to deliver evidence-based treatments with fidelity. Workplace-based clinical supervision often is a commonly provided support in community mental health, yet too few studies have empirically examined supervision and its impact on clinician fidelity and treatment delivery.
Method
Building on a Washington State-funded evidence-based treatment initiative (CBT+), we conducted a randomized controlled trial (RCT), testing two supervision conditions delivered by workplace-based supervisors (supervisors employed by community mental health organizations). The RCT followed a supervision-as-usual (SAU) phase for comparison. The treatment of focus was trauma-focused cognitive behavioral therapy (TF-CBT). Clinicians (N = 238) from 25 organizations participated in the study across the SAU baseline and RCT phases. In the RCT phase, clinicians were randomized to either symptom and fidelity monitoring (SFM) or SFM and behavioral rehearsal (SFM + BR). For BR, clinicians engaged in a short role play of an upcoming treatment element. Supervisors delivered both conditions, with regular study monitoring for drift. Clinicians audiorecorded therapy sessions with enrolled clients, and masked coders coded a subset of recordings for adherence to TF-CBT. One hundred and thirty-three clinicians had recorded TF-CBT session data for 258 youth. We examined six adherence outcomes, including potential moderators.
Results
Results of generalized estimating equations indicated that there were no real differences on adherence outcomes for experimental conditions (SFM, SFM + BR) compared to SAU. Adherence scores in the baseline SAU phase and the RCT conditions were high. Only one interaction was significant.
Conclusions
Contrary to our hypotheses, we did not see improvements in adherence with the RCT conditions. However, nonsignificant findings seem best explained by clinicians’ acceptable/high adherence in SAU. This study was conducted within the context of a long-standing, state-funded EBT initiative, in which clinicians and their supervisors receive training and support, and in which participating community mental health organizations have adopted and supported TF-CBT.
ClinicalTrials.gov ID
NCT01800266
Plain Language Summary
Clinicians often receive training in evidence-based treatments (EBTs), but training alone is not enough for clinicians to deliver EBTs well. They need other supports. One of the necessary supports is clinical supervision. In public community mental health organizations, which are often resource-constrained, routine clinical supervision is a commonly available support. However, its potential for supporting high-quality EBT delivery is not well understood. This study looked at supervision and clinicians’ delivery of trauma-focused cognitive behavioral therapy (TF-CBT), an EBT for youth who have mental health problems subsequent to trauma. We found that clinicians who received workplace-based supervision on TF-CBT from TF-CBT-trained supervisors, within the context of a state-funded EBT initiative, delivered TF-CBT well. This initiative supported delivery by providing training and supervisor-specific supports. In a second phase of the study, we rigorously tested supervisors’ use of two specific technique packages. These packages included having supervisors review: (a) graphed client mental health symptoms across treatment and clinicians’ report of TF-CBT elements delivered each session or (b) these plus having clinicians do a brief demonstration of how they would deliver an upcoming TF-CBT element to their client, so supervisors could “see” clinicians’ skill and provide feedback. Contrary to expectations, we did not see important differences in clinicians’ TF-CBT delivery. This may be because the clinicians enrolled in our study were already delivering TF-CBT well and, therefore, there was less opportunity for changes. Future studies should explore if these techniques are more helpful for specific situations or clinicians.
Keywords
Introduction
Mental health-related concerns are prevalent among youth in the U.S. (Bitsko et al., 2022). Because most youth with mental health needs do not receive treatment (Bitsko et al., 2022; Whitney & Peterson, 2019) and because evidence-based treatments (EBT) are not always available in community-settings (Bruns et al., 2016), many states and local jurisdictions are interested in increasing the availability of EBTs for youth and families (e.g., Ashwood et al., 2018; Beidas et al., 2019). However, literature documents a range of challenges. One challenge involves delivering EBTs with fidelity, a multidimensional construct defined broadly as the extent to which treatment is delivered as intended (Tabak et al., 2012). To deliver EBTs with fidelity and be responsive to client needs, providers need support in appropriately tailoring treatment to their clients (Kendall & Frank, 2018) and the local context (Beidas et al., 2019). Identification of support strategies that are readily available within community mental health centers (CMHCs) is essential for high-quality mental health availability (Glasgow, 2013).
Workplace-based clinical supervision is a commonly provided support in CMHCs and has been highlighted as a potentially cost-neutral and feasible implementation strategy for EBT implementation (Schoenwald et al., 2008; Tugendrajch et al., 2023) that can improve EBT fidelity (Beidas & Kendall, 2010; Henggeler et al., 2002) and client outcomes (Bambling et al., 2006; Schoenwald et al., 2009). In some studies, supervision may matter as much, or more, than the modality of training for adherence and competency in EBTs (Beidas et al., 2012; Rakovshik et al., 2016; Sholomskas et al., 2005).
Theoretical work on supervision (Milne & Reiser, 2012) and clinician training (McLeod et al., 2018b) highlight several “gold standard” EBT supervision techniques (Milne, 2007; Roth et al., 2010). These include opportunities for practice, skill-building, and feedback which can activate learning processes that theoretically facilitate learning and reflection (Beidas et al., 2014; Kolb, 1984). Specifically, these supervision techniques include behavioral rehearsal, live or recorded session review, fidelity monitoring, and client symptom monitoring.
While workplace-based supervision research in CMHCs is limited, the available studies provide some empirical support for these techniques. An observational study of multisystemic therapy (MST) found that workplace supervisors’ use of active practice of skills, case conceptualization, and monitoring fidelity to MST, predicted greater clinician MST adherence and better client outcomes (Schoenwald et al., 2009). A more recent experimental study found that a supervision approach emphasizing corrective feedback based on actual practice review, and skills coaching using behavioral rehearsal, led to greater competency in an EBT than supervision as usual (Martino et al., 2016), with behavioral rehearsal defined as a simulated interaction, or role play, involving a trainee and another individual (Cross et al., 2007). Similar results were obtained in a study focused on graduate student trainees (Bearman et al., 2017). These findings, combined with related research focused on EBT expert consultation (Choy-Brown & Stanhope, 2018; Miller et al., 2004), provide empirical support for supervision techniques involving practice, observation, feedback, and progress and fidelity monitoring.
While the literature provides evidence for techniques that may impact treatment delivery, studies empirically testing specific supervision techniques in CMHCs are needed. Further, we lack an understanding of which techniques are most beneficial. This understanding is essential, given that although many organizations provide regular supervision for clinical providers, the typical 1–2 hours weekly is limited considering high caseloads (Choy-Brown & Stanhope, 2018; Dorsey, Pullmann et al., 2017). Additionally, workplace-based supervisors use supervision to accomplish many competing functions (Dorsey, Pullmann et al., 2017), including emotional support to clinicians (Fukui et al., 2019) and covering administrative needs. As such, guidance on how to maximize potential impact of supervision is needed.
Another level of precision largely absent from supervision research is what works for whom. The effectiveness of supervision techniques in improving clinician adherence may differ (i.e., be moderated) by clinician or supervisor characteristics. Social cognitive theory posits that self-efficacy is important for behavior (Bandura, 1998) and has been linked to successful implementation of physical activity interventions (Huijg et al., 2013). Both self-efficacy and knowledge play important theoretical roles in a mechanistic model of clinician training and consultation (McLeod et al., 2018a). For supervisors, their self-efficacy in supervising an EBT, or EBT knowledge, may affect supervision technique delivery, impacting clinicians’ adherence. For clinicians, self-efficacy or knowledge in the EBT may impact benefit of specific supervision techniques. Supervisors may adjust their approach based on clinician characteristics (Milne, 2009; Milne & James, 2000), as found in a study of workplace-based supervisors where a more directive approach was used with clincians less experienced in the EBT (Meza et al., 2023). In a study using direct observation of EBT-focused supervision, supervisors with less EBT knowledge were more likely to cover non-EBT content (Pullmann et al., 2018).
This article presents the findings from a within and between subjects hybrid type 3 randomized controlled trial (RCT) of supervision strategies, conducted in publicly funded CMHCs. The RCT compares clinician adherence, an important aspect of fidelity (Dorsey et al., 2013) for two randomized supervision conditions that followed a baseline supervision-as-usual (SAU) phase. The randomized conditions are (a) symptom and fidelity monitoring (SFM) and (b) SFM plus behavioral rehearsal (SFM + BR). We hypothesized that adherence would be highest for SFM + BR, given that the BR involved an active, experiential activity for clinicians and provided supervisors the opportunity to observe an “analog” of clinicians’ treatment delivery (Beidas et al., 2014). We hypothesized that both SFM and SFM + BR would outperform SAU, as both experimental conditions include opportunities for reflection on treatment delivery and client response. Clinicians delivered trauma-focused cognitive behavioral therapy (TF-CBT) (Cohen et al., 2017), an EBT for youth mental health symptoms subsequent to trauma exposure. Given that some implementation strategies, like some clinical interventions, may work best for subsets of individuals, we also examined potential moderators with empirical support in the literature, including clinicians’ objective knowledge and self-efficacy in TF-CBT and supervisors’ TF-objective knowledge in TF-CBT and self-efficacy in supervising TF-CBT.
Methods
Data came from the NIMH-funded Supervision to Enhance Practice Study (STEPS) focused on workplace-based clinical supervision of TF-CBT (Dorsey et al., 2013), with primary aims of (a) describing “baseline” SAU strategies (Phase I; September 2012–August 2013) and (b) evaluating the effects of two different supervision conditions relative to each other and to baseline SAU on clinician adherence and client outcomes (Phase II; September 2013–December 2016). The Phase II supervision conditions incorporate gold standard elements from efficacy and effectiveness trials.
Procedures
Ethical Review
Washington State IRB, and subsequently the University of Washington IRB, approved all study procedures.
Study Sample Recruitment
The present study builds on a longstanding academic-community partnership, the Washington State EBT initiative (called CBT+), focused on public mental health (Dorsey et al., 2016). In a 2015 analysis, 83% of all public mental health organizations in Washington had participated. The CBT+initiative provided training in TF-CBT, as well as depression, anxiety, and behavior problems, for CMHCs. Organizations participating in CBT+ sent at least one supervisor for 3 days of in-person training and 6 months of twice-monthly consultation, focused on applying the training to cases. Supervisors had the option to join technical assistance calls every month and a yearly supervisor training. To address trained provider attrition, organizations could send clinicians each year.
Organizations that participated in CBT+ and still had at least one TF-CBT-trained supervisor were approached. Our planned sample size targets were determined via an a priori power analysis. Detailed study descriptions were provided to senior leaders and potentially eligible supervisors, followed by informed consent procedures with interested supervisors. Across Phases I and II, of the 33 organizations approached, 25 (76%) were interested in participating. Enrolled supervisors identified potentially eligible clinicians. The research team invited them to participate, screened for eligibility, and obtained informed consent. Enrolled clinicians introduced the study to guardians of youth who met study criteria. If families expressed interest, study staff conducted final eligibility screening, and informed consent/assent. Clinicians audiorecorded all TF-CBT sessions with enrolled study youth for 6 months or until treatment termination, whichever happened first. Clinicians labeled recordings with the primary treatment component for that session and recordings were automatically date-stamped. Any portion of supervision meetings in which enrolled TF-CBT cases were discussed were also recorded. At the end of the Phase II RCT, organizations received $3,000 for participation. Compensation for completing surveys was $30 for supervisors and clinicians, $20 for guardians, and $10 for youth.
In Phase II, clinicians continuing from Phase I and newly enrolled clinicians were randomized by the last author (M.D.P.) to one of two supervision conditions stratified by supervisor (random number generator) to ensure condition balance within supervisors (see Figure 1). Study staff notified clinicians of their condition. Supervisor adherence to condition was monitored. Research assistants masked to condition reviewed four randomly selected supervision meetings per supervisor (two per condition, distributed across clinicians) within 2-weeks of the supervision meeting occurring. Experimental drift was exceedingly rare (fewer than five instances a year); however, when identified, supervisors were contacted within 2 weeks for booster training on conditions. Supervisors received an email on condition adherence every 2 weeks.
STEPS Consort Diagram
Intervention
The delivery of TF-CBT was the focus of supervision. TF-CBT is an EBT designed to address symptoms of posttraumatic stress (PTS), depression and disruptive behaviors among youth exposed to traumatic events (Cohen et al., 2017; Dorsey, McLaughlin et al., 2017). The acronym “PRACTICE” summarizes components clustered in three phases: (a) stabilization consisting of psychoeducation, parenting (for guardians), relaxation, affective modulation, cognitive coping (i.e., PRAC), (b) trauma narration (TN) and processing consisting of the initiation of discussion and/or writing about the traumatic event/s and cognitive processing (i.e., T), and (c) integration and consolidation including in-vivo mastery, conjoint caregiver–child sessions, and enhancing safety and future development (i.e., ICE). For our examination of adherence, we focused on stabilization, gradual exposure in stabilization, and TN (within the TN and processing phase) as well as days until TN initiation.
Description of Supervision Conditions
SAU/Phase I (Baseline)
Clinicians who participated in Phase I of STEPS received SAU. Supervisors were asked to supervise clinicians’ TF-CBT cases as they naturally would. Having a baseline supervision phase allows for examination of clinicians’ TF-CBT delivery under usual supervision—without intervention—prior to introduction of the two RCT conditions in Phase II of STEPS. In the SAU phase, supervisors most often used techniques that included supportive listening, information gathering, didactic instruction, and providing clinical suggestions (Dorsey et al., 2018).
SFM
In the Phase II RCT, clinicians in both conditions monitored key symptoms in each session using brief measures standard in the CBT+-Initiative. These include the child-completed Screen for Child Anxiety-Related Emotional Disorders—Anxiety and PTS Subscales (Birmaher et al., 1997; Muris et al., 2000) and the caregiver-completed externalizing subscale of the Pediatric Symptom Checklist-17 (PSC-17) (Gardner et al., 2007). These measures were available through the deidentified, web-based measurement feedback system, EBP toolkit (www.ebptoolkit.com), used by all CBT+ training participants, where clinicians use monikers for their clients (e.g., skateboarder). We added a feature that automatically graphed measure scores over time, providing clinicians and supervisors with a pictorial representation of symptom improvement, maintenance, or deterioration. Fidelity monitoring was also conducted within EBP toolkit, via a short TF-CBT adherence checklist completed by clinicians after treatment sessions. Supervisors reviewed symptom and adherence data by accessing EBP toolkit during supervision. Supervisors had a slightly expanded TF-CBT checklist that included follow-up adherence queries, including key elements of the TF-CBT components and cross-cutting CBT techniques (e.g., homework, role-play), as well as a prompt on preparing for the upcoming session.
SFM + BR
In the Phase II RCT, clinicians in the SFM + BR condition received SFM and an additional, multipurpose strategy—behavioral rehearsal (BR). The inclusion of BR is potentially a high-yield addition to address concerns of relying on clinician self-report of fidelity (i.e., indirect methods) and promote skill building (Bearman et al., 2013). In the SFM + BR condition, in each supervision session, supervisors had the clinician do a short BR (5–10 min) demonstrating how they would deliver a TF-CBT element relevant to an upcoming session, followed by supervisor feedback. A set of brief BR guidelines (e.g., bulleted form; one-page; see our Supplemental File) were provided to supervisors for TF-CBT components, along with pointers for addressing common challenges (e.g., dealing with avoidance, homework assignment/review).
Participants
Supervisors
Fifty-six supervisors were enrolled across Phases I and II; 48 of these supervised clinicians with recorded sessions (analysis sample). Table 1 provides demographic information for all participants. Supervisor participants were located in 29 CMHCs in 39 offices across WA. Of 70 supervisors approached, 78% were eligible and agreed to participate. Criteria for study inclusion were receiving TF-CBT-specific training as part of the EBT initiative and supervising two or more clinicians eligible to participate. There were no exclusionary criteria. Thirty-three supervisors were enrolled in Phase I. For Phase II, 25 of these continued and 23 additional supervisors were enrolled.
Participant Characteristics a
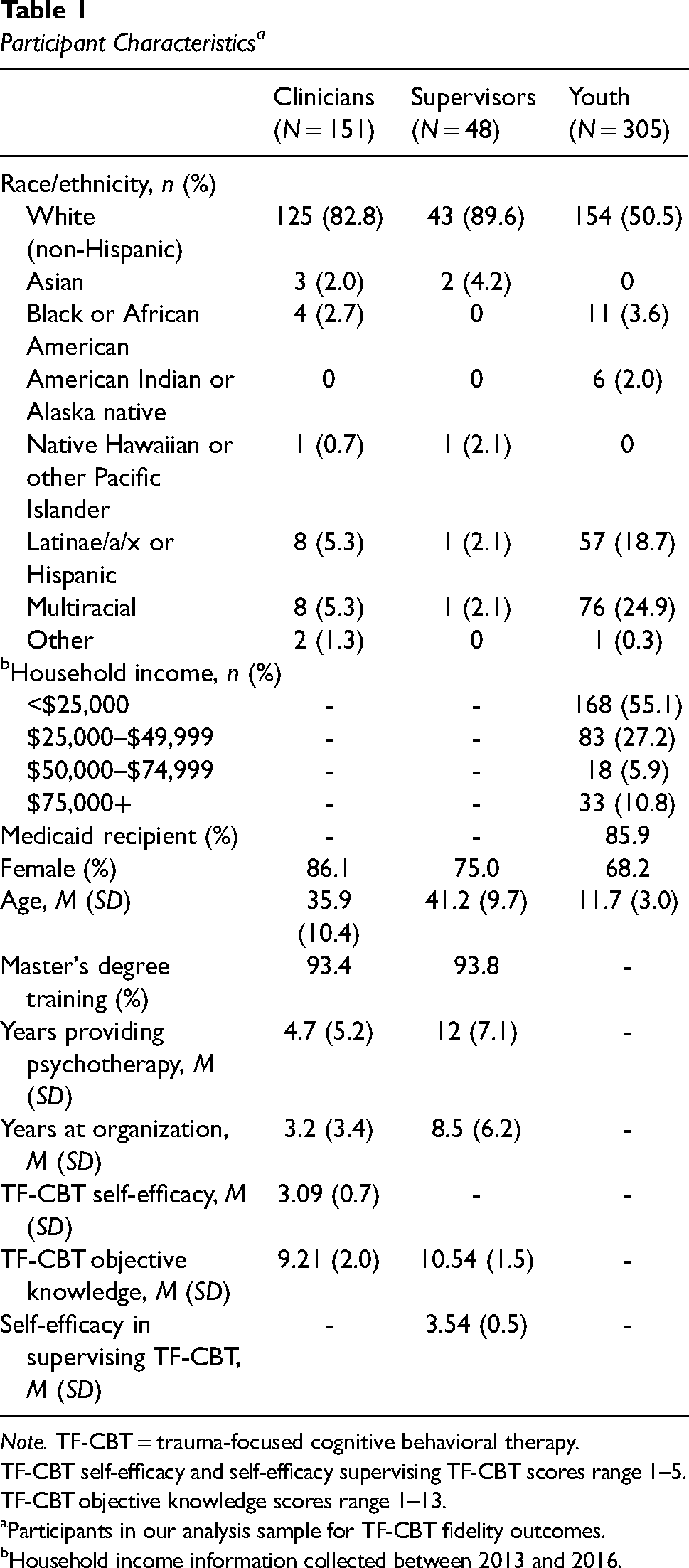
Note. TF-CBT = trauma-focused cognitive behavioral therapy.
TF-CBT self-efficacy and self-efficacy supervising TF-CBT scores range 1–5.
TF-CBT objective knowledge scores range 1–13.
Participants in our analysis sample for TF-CBT fidelity outcomes.
Household income information collected between 2013 and 2016.
Clinicians
Two hundred thirty-eight clinicians were enrolled across phases I and II; 151 clinicians had some child data (clinical outcome measures), 133 of these had recorded TF-CBT sessions and are part of the analysis sample (see Figure 1). Ninety-five clinicians were enrolled in Phase I. For Phase II (RCT), 69 of these continued and an additional 143 clinicians were enrolled. Across both phases, of the 303 approached, 78% were eligible and agreed to participate. Criteria for study inclusion were receiving supervision from a participating supervisor and being trained in TF-CBT. Training was defined as: (a) receiving training through the initiative or (b) through completion of the freely available, 10-hr, online TF-CBT program (https://tfcbt.musc.edu/) and previous provision of TF-CBT to one client under supervision of a TF-CBT-trained supervisor at their organization. In-person, initiative training was not required for clinicians because annual training spaces are typically limited to two to three clinicians per organization. Given high turnover rates, organizations regularly rely on online training before clinicians can do in-person training. Exclusionary criteria were having an adult-only caseload, employed less than 80% time, and immediate plans to leave the organization.
Children and Adolescents
Participants were 305 youth and a guardian; 258 youth had recorded TF-CBT sessions and are part of the analysis sample. The study team contacted 370 families across both phases; 82.4% were eligible and agreed to participate. Reasons for nonparticipation and rates are included in Figure 1. Inclusion criteria were: (a) client of a participating clinician and receiving TF-CBT; (b) 6–17 age range; (c) endorsed trauma history; (d) significant baseline PTS symptoms assessed by the study team; (e) living with a parent/legal guardian willing to participate; and (f) spoke English (guardians could speak Spanish or English). Exclusion criteria were: (a) youth having a pervasive developmental disorder or substantial cognitive impairment and (b) guardian serious mental illness.
Measures
All supervisor and clinician self-report measures were administered upon participant enrollment in the study, and before engaging in any other study activities (e.g., supervision/client session recording, participation in RCT conditions). For most participants, enrollment was at the beginning of Phase I or II. However, given high rates of supervisor and clinician turnover, we continued to enroll participants during both study phases.
Participant Characteristics
Participants provided information on demographics, work environment, clinical experience, training, and other background information (Table 1). Supervisory-specific information was also obtained (e.g., number of supervisees).
TF-CBT Knowledge
Supervisors and clinicians completed the 13-item TF-CBT knowledge test. Adapted from the Denver Post Health Survey (Fitzgerald, 2010), this measure reflects domains in the TF-CBT certification program. Participants responded to multiple choice and true–false items. In our sample, average item difficulty was 0.73 (range 0.32–0.93) and average item discrimination was 0.38 (range 0.20–0.53), showing a good relation between probability of answering individual items correctly and respondents’ total score. Our measure also demonstrated good convergent validity with clinician-reported TF-CBT training extensiveness (r = .42, p < .001) and the related, but distinct construct of TF-CBT self-efficacy (r = .27, p < .001).
Self-efficacy in Delivering TF-CBT
Clinicians were asked to complete an 11-item index to assess their self-efficacy in TF-CBT (Deblinger & CARES Institute, 2013; NCVRTC MUSC, 2010). Participants rated perceived competency in implementing TF-CBT on a 5-point Likert scale (ranging from 0 = not at all to 4 = exceptionally). Participants rated their self-efficacy in TF-CBT skills such as, “Completing trauma narratives with children.” Higher scores indicate greater self-efficacy in TF-CBT delivery. Cronbach's alpha for this sample was .92.
Self-efficacy in Supervising TF-CBT
Supervisors’ perceived competence in supervising TF-CBT was measured using a 13-item self-efficacy in supervision index adapted from a measure created by TF-CBT developers (Deblinger & CARES Institute, R. U., 2013; NCVRTC, MUSC, 2010). Items were measured on a 5-point Likert scale (1 = not at all to 5 = exceptionally). Sample items include an assessment of confidence to: “Supervise clinicians in all of the TF-CBT components.” Higher scores indicate greater self-efficacy in TF-CBT supervision. Cronbach's alpha for this sample was .93.
PTS Symptoms
The 20-item UCLA Post Traumatic Stress Disorder Reaction Index (PTSD-RI; Steinberg et al., 2004) was administered by study staff to youth (ages 8 and higher) and their guardians to assess baseline PTS symptoms and determine youth study eligibility (severity cutoff of ≥21 or algorithm scoring for likelihood to meet diagnostic criteria). The UCLA PTSD-RI demonstrates good convergent validity and good to excellent test–retest reliability, with Cronbach's α .90 for the total scale (Steinberg et al., 2013).
Days until TN Receipt (Outcome Variable)
Days until TN receipt were calculated as days between the client's first session and the TF-CBT session focused on the TN component.
TF-CBT Adherence (Outcome Variables)
The 25-item, TF-CBT-specific version of the Therapeutic Process Observational Coding System for Child Psychotherapy (TPOCS-S Garland et al., 2010; McLeod & Weisz, 2010) was used to assess TF-CBT adherence by coding audiorecorded TF-CBT sessions. The measure includes 10 TF-CBT content area items (e.g., relaxation, TN), two general content items (i.e., assessment, other topics/crisis or case management), and 13 therapeutic techniques (e.g., assign/review homework, Socratic questioning). This study uses only the 10 TF-CBT content items. The scoring strategy includes extensiveness ratings to assess the degree to which clinicians use each element in a session, using a 7-point Likert-type extensiveness scale 0–6 1 (0 = not used to 6 = extensively). To determine extensiveness, coders note element delivery in 5-min intervals using symbols to denote thoroughness within that interval. At the end of the session, coders assign a total extensiveness score by item that reflects frequency and thoroughness; thus extensiveness ratings provide dosage information about each TF-CBT component. Coders were masked to clinician/youth condition.
Coder Training/Therapy Session Sampling and Reliability
Analysis Plan
Our analysis combined data from STEPS Phases I and II. Phase I data represents the SAU condition. Phase II included some continuing supervisors and clinicians from Phase I, and new supervisors and their clinicians. Therefore, some supervisors and clinicians contribute data to phases I and II. Descriptive statistics summarized participant demographics and baseline measures. To evaluate the effects of supervision conditions on adherence, we planned to use hierarchical generalized linear models to account for three-level clustering (i.e., client-level data within each clinician within their supervisor). However, the three-level model failed to converge in some analyses. For models that converged, the ICC of the null model showed that <5% of the total variance in outcomes occurred at the supervisor-level. We instead employed generalized estimating equations (GEEs), which allow for two-level clustering predicting adherence, using individual-mean fidelity scores for each client per clinician. Supervision condition was the main predictor, and SAU was the reference category.
Main Effects
Six GEEs were conducted to test the effect of supervision condition and clinician- and supervisor-level variables on outcomes of interest: (a) stabilization phase (i.e., PRAC) extensiveness, (b) gradual exposure occurrence during stabilization phase, (c) gradual exposure extensiveness during stabilization phase, (d) TN occurrence, (e) TN extensiveness, and (f) days until TN receipt. Stabilization phase occurrence was not included as an outcome because of lack of variability: the stabilization phase of TF-CBT involves the first set of treatment components and thus occurred for all cases that began treatment. When the outcome variable reflected occurrence (i.e., a binary yes/no outcome), we used binomial models; Gaussian models were used for extensiveness outcome variables. For each analysis, we included supervision condition and the following covariates: child baseline PTS, clinician TF-CBT objective knowledge, clinician TF-CBT self-efficacy, supervisor TF-CBT objective knowledge, and supervisor self-efficacy in supervising TF-CBT. For the model predicting TN occurrence, we added one additional covariate, the total number of sessions submitted by each clinician, as more sessions submitted means that clinicians likely delivered more TF-CBT sessions, which may naturally increase the likelihood of TN occurrence. Analyses were conducted in R 4.1.2 using the gee package. G*Power 3.1 was used to assess whether our analyses were powered for main effects and moderation analyses (Faul et al., 2009). Assuming power of 0.8, our sample size was powered to detect small-to-moderate effect sizes (Cohen's f2 = 0.1). Given that our data had limited missingness (≤5%), we used a listwise deletion approach.
Interaction Effects
We ran separate models to examine whether four covariates—clinician TF-CBT objective knowledge, clinician TF-CBT self-efficacy, supervisor TF-CBT objective knowledge, and supervisor self-efficacy in supervising TF-CBT—were potential moderators of supervision condition on our six outcomes (i.e., four potential moderators for six outcomes; total of 24 additional analyses). Each analysis had one interaction term (Potential Moderator × Supervision Condition). Similar to the main effects models, the only analyses with one additional covariate (i.e., total number of sessions submitted) were the ones where TN occurrence was the outcome. We used corrections to adjust for multiple testing to reduce false discovery rate (Benjamini & Hochberg, 1995).
Results
Randomization tests were conducted to ensure that the distribution of our clinician and child client variables were balanced across randomized conditions. There were no statistically significant differences across conditions (p > .05; Cohen's d range = 0.06–0.31). Table 1 presents participants’ demographic information. Supervisors and clinicians were predominantly white (supervisors = 90%, clinicians = 83%), female (supervisors = 75%, clinicians = 86%), held a master's degree (supervisors = 94%, clinicians = 93%), and ascribed to a primarily CBT orientation (supervisors = 73%, clinicians = 66%). Youth were racially and ethnically diverse, mostly female, from households with an income less than $25,000, and receiving Medicaid-funded services. The average age for youth was 11.7 (SD = 3.0) and the average baseline PTS score was 36.8 (SD = 14.2).
On average, across supervision conditions, clinicians submitted around the same number of TF-CBT sessions (MSAU = 8.60, MSFM alone = 8.32, and MSFM + BR = 8.09), and adherence outcomes were very similar (Table 2). For example, clinicians use of TN with youth was 64% in the SAU condition, 62% in TN in the SFM condition, and 61% in the SFM + BR condition, suggesting limited variation in TN occurrence across conditions. Moreover, days until TN receipt were also similar. The only adherence outcome with some (nonsignificant) variation by condition was TN extensiveness. TN extensiveness, and all other adherence scores, ranged from 0 to 6 in our data. The average level of TN extensiveness was 4.24 (SD = 0.79) in the SAU condition, 4.42 (SD = 1.17) in the SFM condition, and 4.35 (SD = 0.94) in the SFM + BR condition. In the SFM and SFM + BR conditions, clinicians had a .2 or .1 increase in TN extensiveness compared to SAU, but differences in TN extensiveness were not significant, F(2,150) = 1.03, p = .36. One-way ANOVAs were computed to determine effect sizes across conditions and all effect sizes were small (Cohen's f range = 0.03–0.07). Table 2 summarizes all fidelity outcomes by supervision condition.
Summarizing Adherence Outcomes by Supervision Conditions

Note. SP = stabilization phase components (PRAC components; from the TF-CBT PRACTICE acronym); GE = gradual exposure; TN = trauma narrative; TF-CBT = trauma-focused cognitive behavioral therapy; SFM + BR = symptom and fidelity monitoring plus behavioral rehearsal; SAU = supervision-as-usual.
Occurrence outcomes are frequencies and extensiveness outcomes are in means (range 1–6).
GE adherence assessed during during the stabilization phase of TF-CBT.
Table 3A and B presents the estimates from the six GEE models examining effect of the supervision conditions (SFM and SFM + BR) relative to supervision-as-usual on TF-CBT adherence, controlling for hypothesized covariates. Two models had occurrence outcomes (i.e., binary): gradual exposure and TN phase occurrence. Adjusting for covariates, supervision condition was not significantly associated with either of the binary fidelity outcomes (Table 3A). The remainder of the GEE models had continuous outcome variables: stabilization phase extensiveness, gradual exposure extensiveness, TN extensiveness, and days till TN. Adjusting for covariates, supervision condition was not significantly associated with any of the continuous fidelity outcomes (Table 3B).
(A) Main Effects Model Estimates for Relations Between Covariates and Adherence (Binary Outcomes)

Note. OR = odds ratio; SE = standard error; TF-CBT = trauma-focused cognitive behavioral therapy; PTS = posttraumatic stress; SFM + BR = symptom and fidelity monitoring plus behavioral rehearsal; SAU = supervision-as-usual.
For conditions SFM and SFM + BR, the reference category was SAU.
Estimate indicates statistical significance (p < .001).
(Continued) (B) Main Effects Model Estimates for the Relation Between Covariates and Adherence (Continuous Outcomes)
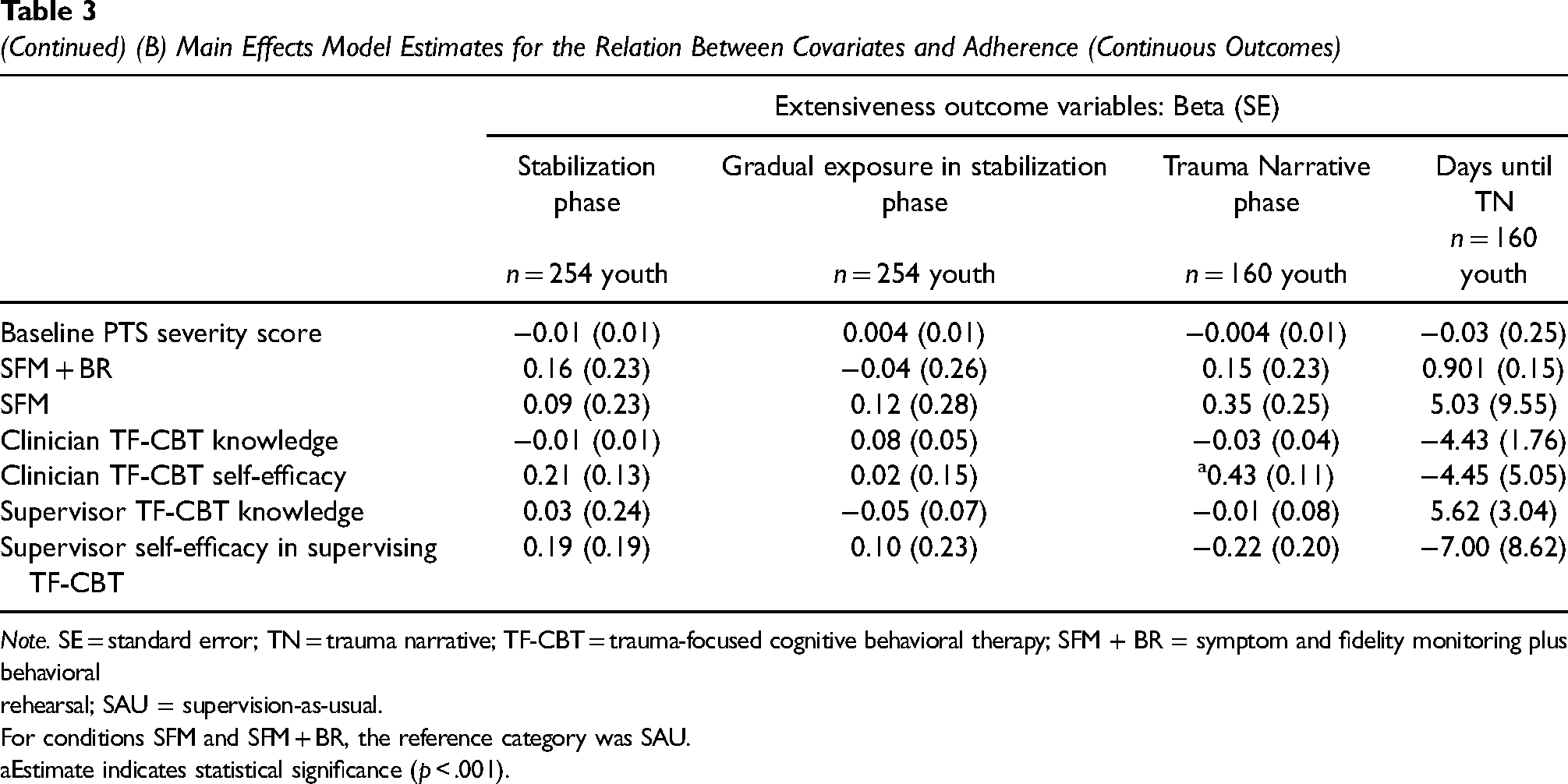
Note. SE = standard error; TN = trauma narrative; TF-CBT = trauma-focused cognitive behavioral therapy; SFM + BR = symptom and fidelity monitoring plus behavioral rehearsal; SAU = supervision-as-usual.
For conditions SFM and SFM + BR, the reference category was SAU.
Estimate indicates statistical significance (p < .001).
After adjusting for multiple comparisons, only one statistically significant interaction effect was found. Clinicians’ TF-CBT self-efficacy moderated the relationship between supervision condition and trauma narration extensiveness. Specifically, higher clinician TF-CBT self-efficacy increased the effectiveness of SFM (vs. SAU) on TN extensiveness by 0.64 (p = .03) and of SFM + BR (vs. SAU) on TN extensiveness by 0.53 (p = .04; see Figure 2). None of the remaining moderators examined were significant (i.e., clinicians’ TF-CBT knowledge or self-efficacy; supervisors’ TF-CBT knowledge or self-efficacy in supervising).

Clinician TF-CBT Self-efficacy Moderates the Effect of Supervision Condition on Trauma Narrative Extensiveness
Discussion
This is one of the first RCTs testing specific supervision techniques, delivered by workplace-based supervisors in community settings. We expected to find that systematic use of more active, gold-standard supervision techniques, such as those in our experimental conditions, would improve clinician treatment adherence. In particular, we expected that adding BR to SFM would have the greatest impact on clinician fidelity, given that this technique provides an opportunity for supervisors to observe how clinicians might deliver a particular treatment element to a client. However, our hypotheses were not supported; clinicians randomized to Phase II experimental conditions, SFM or SFM + BR, did not have higher adherence scores than those in the SAU phase, where adherence was already acceptable or high. Additionally, the SFM + BR condition did not outperform SFM. Only one of the moderators examined, clinician TF-CBT self-efficacy, clarified the relation between condition and adherence.
While these findings were unexpected, there may be a few reasons the experimental conditions did not outperform SAU. The most plausible explanation among these is that adherence scores on our six indicators in the SAU phase were already high. For example, the TN was delivered about 60% of the time. While that rate may be low for an efficacy trial, for CHMCs, where there can be high no-show rates and cancelations, and exposure use can be inconsistent (Borntrager et al., 2013; McLeod & Weisz, 2010), TN occurrence for 60% of the cases within 6 months is positive. Perhaps most surprisingly, the dosage or extensiveness (McLeod et al., 2015) of TN delivery during the SAU was also quite high. Considering a common threshold of 70% as indicative of acceptable levels of fidelity where treatment may be potent enough to be beneficial for clients (Dorsey, Lyon et al., 2017); the TN extensiveness scores in the SAU phase (4.24 on our 0–6 scale, ≥70% of the total possible score) meet this threshold. In two studies using similar extensiveness coding systems to examine child anxiety treatment adherence in research settings (efficacy trials) versus community settings, our rates were closer to the efficacy trial ratings (McLeod et al., 2019; Smith et al., 2017).
What might have supported this high rate of adherence in SAU? We suspect the context of our longstanding state-funded EBT initiative offers some explanation. While the funding is modest (200–250k), it supports EBT expertise through ongoing training and consultation for clinicians, with expectations for documented CBT delivery (in the online, deidentified dashboard system). The initiative also explicitly supports supervisors, offering supervisor-specific learning and training opportunities. Supervisors in CMHCs help lead the initiative and provide training. If the initiative supports are partially responsible for the high SAU adherence, our findings provide some good news for what is possible for EBT in other states and systems. However, without financial support, these activities and potential use of the supervision strategies from our experimental conditions could be challenging to implement. The structure of TF-CBT may also have supported clinicians’ high levels of adherence in SAU, given clearly defined elements and ways to conduct exposure with clients. It is also likely that the supervisors who enrolled in the study were highly motivated to provide adherence-focused supervision, and/or that clinicians’ awareness of the recording of sessions and participation in research may have influenced the high adherence rates we saw in our study.
Another plausible explanation for nonsignificant differences across conditions, given other analyses on SAU is that examining the dose of the supervision techniques and/or different clusters of techniques used in conjunction might be a more nuanced approach. In Meza et al.’s (2023) examination of naturally occurring clusters, supervision that included frequent use of directive techniques (e.g., clinical suggestions, didactic instruction), was associated with higher TN delivery. A third explanation is that there may be important moderators of experimental condition effects that we did not examine (e.g., clinician motivation, TF-CBT buy-in, or burnout). However, this seems unlikely given that among moderators we did examine, we found evidence for only one: clinician self-efficacy and TN extensiveness, clinicians reporting higher self-efficacy in either experimental condition—SFM or SFM + BR—demonstrated higher TN extensiveness compared to SAU. Potentially, this suggests that clinicians who perceive themselves as more capable in TF-CBT may be more “ready” to take advantage of active supervision techniques like SFM and/or BR. There was no support for any of the supervisor-level moderators.
Limitations
The study has limitations that should be considered. First, clinician attrition in CMHCs can be high (30–60%/year; Barak et al., 2001; Beidas et al., 2016). Throughout our study, a substantial number of clinicians left their organizations and thus we had fewer youth per clinician than planned (as clinicians who left had shorter periods to enroll youth). We cannot be sure that enrolled clients are representative of clinicians’ practice with other clients who received TF-CBT. We also cannot be sure that clinicians and supervisors did not give more attention to TF-CBT with study-enrolled clients. While youth participant diversity was high, as in many CMHCs, supervisors, and clinicians were mostly White. Although CBT+ state support is modest, many states do not have initiatives or the developed EBT expertise to rely on workplace-based supervisors. Our findings would be most generalizable to community mental health settings where supervision occurs regularly (e.g., on a weekly basis) and providers have received some training in EBTs. Our findings would be least generalizable to settings where supervision is infrequent or non-existent. Treatment adherence is an important outcome; however, we did not examine clinician competence (were BR could be most beneficial) or clinical outcomes. The true “test” of any implementation strategy is if outcomes for clients are improved. Finally, we note that we did not control for baseline adherence levels for clinicians who participated in Phase I SAU and the Phase II RCT.
Conclusions
Clinicians in publicly funded CMHCs who participated in this study appeared to deliver TF-CBT well, within the context of our supportive state-funded EBT initiative. In other contexts or for other EBTs where there is not an established EBT initiative with similar supports, systematic use of techniques in our experimental supervision conditions may have an effect on adherence, or other outcomes like competence or clinical outcomes. Within our sample, we did not see an effect of experimental supervision conditions examined, in large part due to clinicians’ high-quality delivery in the supervision-as-usual phase. If this is mostly due to the state-funded EBT initiative with its training method and focus on building and supporting strong supervisors, this would actually be good news for usual care, academic–community partnerships and implementation supports that may be needed to support EBT. We imagine aspects of our state-supported EBT initiative would be highly relevant for supporting other EBTs.
Supplemental Material
sj-pdf-1-irp-10.1177_26334895251330523 - Supplemental material for A randomized controlled trial testing supervision strategies in community mental health
Supplemental material, sj-pdf-1-irp-10.1177_26334895251330523 for A randomized controlled trial testing supervision strategies in community mental health by Shannon Dorsey, Rashed AlRasheed, Suzanne EU Kerns, Rosemary D Meza, Noah Triplett, Esther Deblinger, Nathaniel Jungbluth, Lucy Berliner, Lavangi Naithani and Michael D Pullmann in Implementation Research and Practice
Footnotes
Acknowledgments
We acknowledge the Washington State Division of Behavioral Health and Recovery for funding and supporting the Washington State TF-CBT and CBT+ initiative for being supportive of this research partnership. We also thank all participating organizations, supervisors, clinicians, youth, and families who partnered with us on this research.
Author's Note
Rashed AlRasheed is also affiliated at Department of Community Medicine and Behavioral Sciences, College of Medicine, Kuwait University, Kuwait City, Kuwait.
Noah Triplett is also affiliated at Department of Psychology, University of Maryland, College Park, MD, USA.
Declaration of Conflicting Interests
Dorsey, Deblinger, and Berliner are international TF-CBT trainers and have received compensation for TF-CBT training and consultation. The authors declare no other conflicts of interest.
Funding
This research project was funded by the National Institute of Mental Health (Grant No. R01MH095749; Dorsey PI).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.