
Abstract
Background
Effective teams are essential to high-quality healthcare. However, teams, team-level constructs, and team effectiveness strategies are poorly delineated in implementation science theories, models, and frameworks (TMFs), hindering our understanding of how teams may influence implementation. The Exploration, Preparation, Implementation, Sustainment (EPIS) framework is a flexible and accommodating framework that can facilitate the application of team effectiveness approaches in implementation science.
Main Text
We define teams and provide an overview of key constructs in team effectiveness research. We describe ways to conceptualize different types of teams and team constructs relevant to implementation within the EPIS framework. Three case examples illustrate the application of EPIS to implementation studies involving teams. Within each study, we describe the structure of the team and how team constructs influenced implementation processes and outcomes.
Conclusions
Integrating teams and team constructs into the EPIS framework demonstrates how TMFs can be applied to advance our understanding of teams and implementation. Implementation strategies that target team effectiveness may improve implementation outcomes in team-based settings. Incorporation of teams into implementation TMFs is necessary to facilitate application of team effectiveness research in implementation science.
Plain Language Summary
Teams and team-level constructs are neglected in implementation theories, models, and frameworks (TMFs). This paper calls attention to the importance of teams in implementation research and practice and provides an overview of team effectiveness research for implementation science. We illustrate how the EPIS framework can be applied to advance our understanding of how teams influence implementation processes and outcomes. We identify future directions for research on teams and implementation, including developing and testing implementation strategies that focus on team effectiveness.
Background
Team effectiveness research examines how people work together to accomplish shared goals. Over a century of research on teams and numerous meta-analyses have identified team constructs critical to team effectiveness (Mathieu et al., 2017, 2019), and findings are widely applied in business, industry, healthcare, aviation, and military settings with proven results (Mathieu et al., 2019; Salas, Goodwin et al., 2008; Salas et al., 2013, 2017). Effective teams are productive, efficient, and innovative, while problems in teamwork can cause serious errors and failures (Burke et al., 2018; Gregory et al., 2013; Salas et al., 2017). In healthcare settings, interventions that improve teamwork improve clinical outcomes (Buljac-Samardzic et al., 2020; Hughes et al., 2016; Weaver et al., 2014). However, despite the increasing use of teams in healthcare, team effectiveness research is underutilized, and teams are poorly delineated in the implementation TMFs.
In this paper, we define teams, provide an overview of key constructs in team effectiveness research, and highlight examples of studies that test associations of team constructs with implementation outcomes. Next, we demonstrate how the Exploration, Preparation, Implementation, Sustainment (EPIS) framework (Aarons et al., 2011; Moullin et al., 2019) can be used to integrate and apply team research in implementation science. We describe how to conceptualize different types of teams within the EPIS framework and illustrate them with examples. Finally, we discuss future directions to advance research on teams in implementation science and practice.
Defining Teams
Across healthcare and related service sectors, work is increasingly completed by teams of professionals (Institute of Medicine, 2001; Kerrissey et al., 2023; Mitchell et al., 2012; Rosen et al., 2018; Rosland et al., 2013; Sandoval et al., 2018). A team is “a distinguishable set of two or more people who interact dynamically, interdependently, and adaptively toward a common and valued goal/objective/mission” (Salas et al., 1992, p. 4). Teams engage in both taskwork and teamwork. Taskwork refers to the work-related activities that teams are doing; teamwork describes how teams are doing their work (Dinh & Salas, 2017; Marks et al., 2001). Hackman (2002) described “real teams” as those with a shared task, clear boundaries, authority to manage their work, and reasonable membership stability. Other traditional definitions of teams also emphasize the importance of stability and clear team member role definitions (Kozlowski & Bell, 2003; Rousseau et al., 2006). Many modern teams, however, exhibit dynamic fluctuations in membership and boundaries, making defining teams an ongoing challenge (Benishek & Lazzara, 2019; Kerrissey et al., 2020, 2023; Mathieu et al., 2019).
A key feature distinguishing teams from small groups is interdependence—the extent to which team members are interconnected (Courtright et al., 2015; Kozlowski & Bell, 2003). Task interdependence is “the degree to which taskwork is designed so that team members depend upon one another for access to critical resources and create workflows that require coordinated action” (Courtright et al., 2015, p. 4). Outcome interdependence is “the degree to which the outcomes of taskwork are measured, rewarded, and communicated at the group level” (Courtright et al., 2015, p. 4). Although interdependence varies across teams, task interdependence is an essential feature of teams (Courtright et al., 2015; Kozlowski & Bell, 2003).
Teams can be differentiated from groups of individuals who may work together but who do not constitute a team. For example, in the patient-centered medical home model for primary care practices, providers work as part of a care team that may include medical assistants, nurses, and care coordinators. Instead of primary care providers holding sole responsibility, team members provide different but coordinated types of care and share responsibility for patient outcomes at the team level (Fiscella & McDaniel, 2018). In contrast, consider outpatient mental health clinicians delivering psychotherapy in the same organization. This group is clearly bounded and may have a shared supervisor, but the clinicians can complete their clinical work independently and are evaluated separately. Thus, they would not be classified as a team.
Teams may be constructed from groups. For example, if clinicians formed a workgroup to revise their clinic's intake process, they would become a team. The team members have a shared purpose, depend on one another to complete tasks, and are evaluated on shared output. Similarly, organizations may choose to create multidisciplinary teams of clinicians who work together to provide patient care and share responsibility for outcomes (Miller et al., 2022). In some team-based models, the patient and their family are explicitly included as part of the team (Drake et al., 2009; Katkin et al., 2017).
Attention to teams in implementation science has focused primarily on implementation support teams (Higgins et al., 2012; Metz & Bartley, 2020). An implementation team is “a group of stakeholders that oversees, attends to, and is accountable for facilitating key activities in the selection, implementation, and continuous improvement of an intervention” (Metz & Bartley, 2020, p. 200). In an early synthesis of the implementation science literature, D. L. Fixsen et al. (2005) identified the creation of implementation teams as a critical strategy during the exploration phase. The Active Implementation Frameworks highlight the importance of implementation teams at multiple levels with competencies in implementation, innovation, and change management (A. A. M. Fixsen et al., 2021; Metz & Bartley, 2020; Metz et al., 2014). Similarly, the updated Consolidated Framework for Implementation Research now includes “implementation team members” in the individuals domain and “teaming” (“intentionally coordinating and collaborating on interdependent tasks to implement the innovation”) in the implementation process domain (Damschroder et al., 2022).
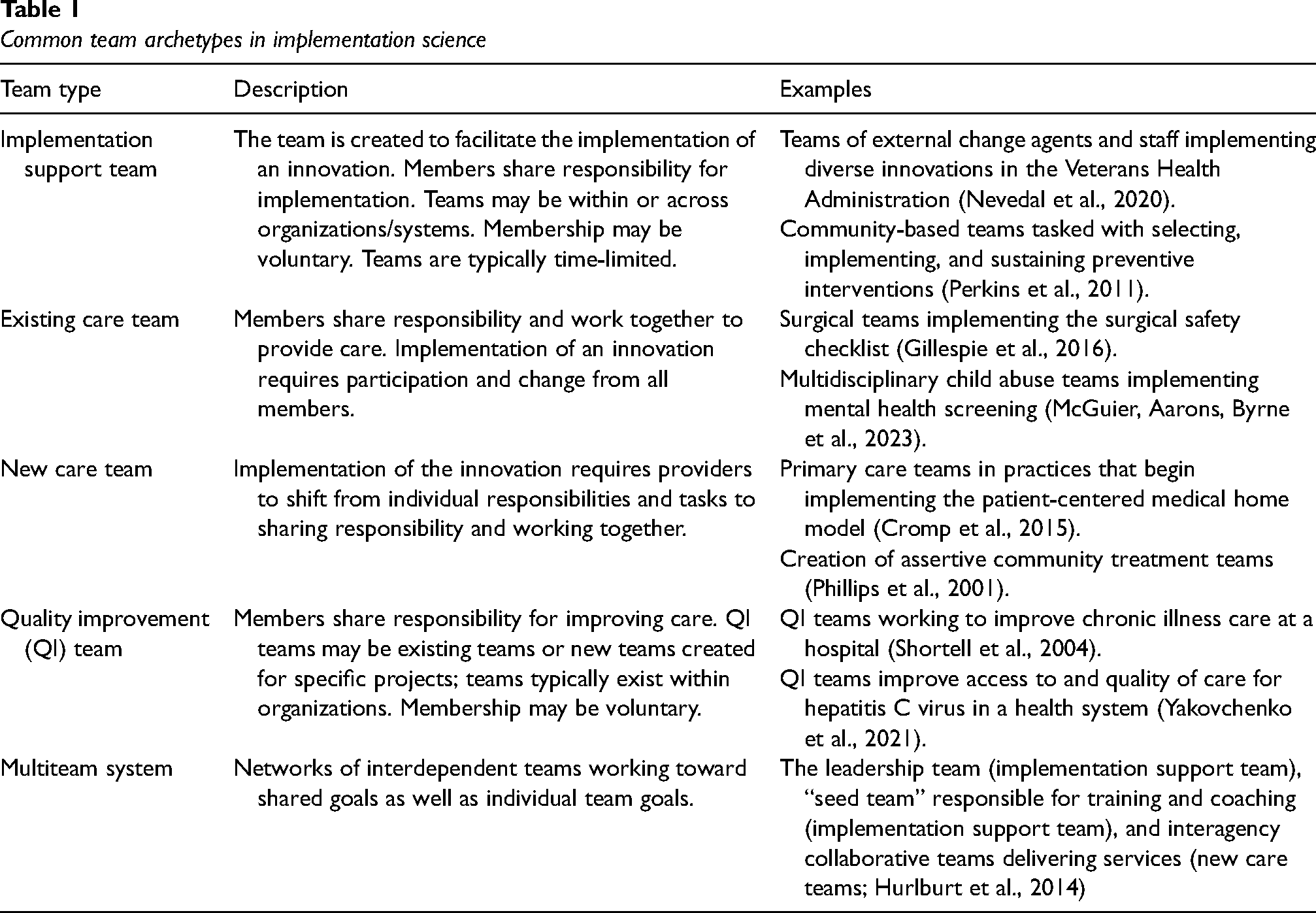
Other types of teams are also relevant for implementation science. Common team archetypes in the implementation science literature (in addition to implementation teams) include existing care teams selected to implement an innovation, care teams formed as part of the innovation (i.e., team-based service models such as assertive community treatment; Bond et al., 2001), and quality improvement teams (Mosel & Shamp, 1993; Tyler & Glasgow, 2021). Some implementation efforts may involve multiteam systems, in which several types of teams interact with one another in pursuit of shared goals (Luciano et al., 2018; Marks et al., 2005; Shuffler et al., 2015). Multiteam systems are “two or more teams that interface directly and interdependently in response to environmental contingencies toward the accomplishment of collective goals” (Mathieu et al., 2001, p. 290). For instance, an implementation effort could include existing teams expected to provide a new service, a team to train and coach service providers on the new practice, and support teams (e.g., technical assistance team and evaluation/research team). Each team has its own goals, but the teams depend on one another and must work together to achieve the broader shared goal of implementing the new practice. Table 1 describes the characteristics of these common team archetypes with examples from implementation studies. 1
Common team archetypes in implementation science
Team constructs for implementation science
In this section, we briefly describe key team constructs for implementation scientists, guided by the input-mediator-outcome-input (IMOI) framework of team effectiveness (Ilgen et al., 2005; Mathieu et al., 2008). The IMOI model is widely used in team effectiveness research and has been applied to healthcare teams specifically (Rosen et al., 2018). It provides a broad framework to organize the diverse array of team constructs that may be relevant to implementation science. As shown in Figure 1, inputs are features of team members, teams, and their tasks and context that shape mediators and outcomes. Mediators are team processes and emergent states that are influenced by inputs to subsequently partly or fully affect outcomes (Ilgen et al., 2005; Mathieu et al., 2008). Outcomes are valued results of team activities, including diverse metrics of team effectiveness (Kozlowski & Bell, 2003; Mathieu et al., 2008; Rosen & Dietz, 2017).

Conceptual model of team effectiveness
The IMOI framework is nonlinear, as teams are affected by complex temporal dynamics (see Mathieu et al., 2019 for a nonlinear visualization of the model). Teams develop over time, respond to changing tasks and contextual demands, and receive cyclical feedback (Georganta et al., 2021; Ilgen et al., 2005; Marks et al., 2001; Mathieu et al., 2008, 2014). Teams are also situated within organizational and system contexts and subject to external influences (Salas et al., 2003). We describe below some well-studied team constructs relevant to implementation science. Figure 2 illustrates examples of team constructs, organized by the IMOI model, integrated into an Implementation Research Logic Model (Smith et al., 2020).

Implementation Research Logic Model with examples of team constructs and team-focused implementation strategies
Inputs: Team Structure and Composition
Team inputs include structural and compositional factors. Structural features of teams include task and outcome interdependence, task characteristics (e.g., complexity and scope of work), location in time and space (e.g., synchronous vs. asynchronous and virtual vs. in-person), and differentiation of skills and authority within the team (Hollenbeck et al., 2012; Kozlowski & Bell, 2003; Mathieu et al., 2017, 2019). Compositional features refer to the combination of team members’ characteristics. Examples include team size, demographic and professional diversity, team member attributes (e.g., skills and personality), and changes in team members (i.e., “churn” or turnover; Jackson et al., 2003; Kozlowski & Bell, 2003; Mathieu et al., 2017, 2019).
Mediators: Team Processes and States
Mediators are team processes and states that may be affective, behavioral, or cognitive (Grossman et al., 2017; Ilgen et al., 2005; Mathieu et al., 2008; Mitropoulos & Memarian, 2012). Affective/motivational and cognitive mediators are conceptualized as emergent states arising from behavioral team processes; they can also serve as inputs that impact behavioral team processes (Marks et al., 2001). Team functioning is a broad term referring to multiple, intertwined processes and states. Many specific processes and states, as well as overall team functioning, are associated with team effectiveness.
Behavioral team processes describe what team members do—how they interact with one another, their task(s), and their resources to produce outcomes. Marks et al. (2001, p. 357) define team processes as “members’ interdependent acts that convert inputs to outcomes through cognitive, verbal, and behavioral activities directed toward organizing taskwork to achieve collective goals.” Their conceptual framework of team processes identifies three broad categories of processes: transition processes occurring between performance episodes, action processes occurring as members engage in active work, and ongoing interpersonal processes (Marks et al., 2001; Mathieu et al., 2020). Processes can be narrowly or broadly defined; research supports a hierarchical structure of processes consistent with Marks et al.’s (2001) framework (LePine et al., 2008; Mathieu et al., 2020). Examples of behavioral processes are mission analysis, goal specification, communication, coordination, backup/supporting behavior, learning behavior, and conflict management (Bisbey & Salas, 2019; Grossman et al., 2017; Kozlowski & Ilgen, 2006). These processes can be further delineated into types of behaviors or specific dimensions, such as communication quality and frequency (Marlow, Lacerenza et al., 2018) or types of learning behaviors (Wiese et al., 2022).
Affective/motivational states reflect shared feelings and attitudes that emerge from team members’ interactions with each other (Bisbey & Salas, 2019; Grossman et al., 2017). Examples include team cohesion, collective efficacy, trust, and psychological safety (Grossman et al., 2017; Kozlowski & Bell, 2003). Well-studied cognitive states include team mental models and transactive memory (DeChurch & Mesmer-Magnus, 2010; Mohammed et al., 2017; Ren & Argote, 2011). Mental models are “organized mental representations of the key elements within a team's relevant environment that are shared across team members” (Mohammed et al., 2010, p. 877). When team members are “on the same page” about what to do and how to do it, teams perform better (Mohammed et al., 2010). Transactive memory refers to how teams encode, store, and retrieve information by building a shared awareness of who knows what, allowing increasing specialization and greater cognitive efficiency (Ren & Argote, 2011).
Processes and states are closely intertwined. For example, the affective state of psychological safety (i.e., the extent to which interpersonal risk-taking is safe) is associated with learning behaviors (e.g., seeking feedback and discussing errors; Edmondson, 1999). Shared mental models increase coordination, therefore improving team performance (Marks et al., 2002). Because of reciprocal associations between processes and states, they may be conceptualized as inputs, mediators, or outcomes, depending on the research question.
Outcomes: Team Effectiveness
We use the term “team effectiveness” as an overarching term for team outcomes, acknowledging that an outcome can vary across studies given the complexity of temporal dynamics within teams. Hackman and colleagues’ model of team effectiveness (Hackman, 1983, 2012; Hackman & Wageman, 2005) specifies three dimensions of team effectiveness: (a) perceptions of the team's output by those who receive, review, or use it (i.e., performance); (b) the extent to which the team improves their capacity to work together and the sustainment of the team over time (i.e., team viability), and (c) the impact of the team on members’ learning and development. Teams can be effective in different ways and at multiple levels.
Although effectiveness and performance are sometimes used interchangeably, we use team performance to indicate the first dimension of effectiveness. Team performance refers to the quality, efficiency, and productivity of teams (Rosen & Dietz, 2017; Slyngstad et al., 2017). For example, a team may increase organizational profits, produce innovative products, or attain effective implementation or service outcomes (e.g., reach, fidelity, and safety; Proctor et al., 2011). Performance is context-specific and depends on the goals of the team; it is typically assessed at the team or organizational level. The latter two dimensions of effectiveness (i.e., team viability and impact on members) are often assessed at the team and individual levels. Effectiveness may be demonstrated through member satisfaction and team viability (e.g., members want to continue on the team) as well as gains in team members’ skills, knowledge, and self-efficacy (Bisbey & Salas, 2019; Slyngstad et al., 2017). Importantly, given the dynamic nature of teams, these team outcomes serve as inputs into recurring and dynamic cycles of team interactions.
Research on Teams and Implementation
Relatively few studies have examined how team constructs impact implementation of evidence-based practices (EBPs; McGuier et al., 2022). In existing care teams, more adaptive team functioning has been associated with greater improvements in chronic care delivery (Cramm et al., 2014), implementation of more elements of a mental health EBP (Ditty et al., 2015), and greater EBP sustainment in outpatient mental health clinics (Mohr et al., 2018). A study of implementation support teams found that “early adopter” teams had better team functioning than later adopters (Yakovchenko et al., 2021). Some studies have examined how team effectiveness affects implementation outcomes. One study of teams responding to child abuse found that team members’ subjective perceptions of overall team performance were positively associated with innovation acceptability, appropriateness, and feasibility, but not reach (McGuier, Aarons, Byrne et al., 2023).
Overall, prior studies support the relevance of team constructs and approaches for implementation. However, team constructs are often poorly specified, and findings are rarely situated in the well-developed literature on teams. The small number of studies and heterogeneity in team types and constructs limits our capacity to identify team-level targets and mechanisms of change. Building our understanding of how teams affect implementation requires a better conceptualization of team-level constructs in implementation science TMFs.
Application of the EPIS Framework to Implementation Research With Teams
Conceptualizing Teams Within the EPIS Framework
Teams and team constructs are not explicitly included in most implementation TMFs, hindering our capacity to understand the diverse ways that teams influence implementation processes and outcomes. The EPIS framework (Aarons et al., 2011; Moullin et al., 2019) is a widely used process and determinant implementation framework (Moullin et al., 2019). Although EPIS, like other TMFs, does not highlight teams, EPIS is a flexible framework that can facilitate the application of team effectiveness approaches.
EPIS invokes the outer system context, inner organizational context, bridging factors that span and link outer and inner contexts, innovation characteristics and developers, and interconnections and linkages within and across contexts (Lengnick-Hall et al., 2021; Moullin et al., 2019). EPIS identifies four implementation phases within which teams may function (Moullin et al., 2019). Teams can be conceptualized in multiple ways within EPIS depending on their composition, level, functions, and existence across implementation phases. EPIS can accommodate existing teams within and across outer and inner contexts, the creation and efforts of implementation support teams, and multiteam systems. In the following sections, we illustrate how team constructs fit within the EPIS framework.
Inner Context
The EPIS inner context refers to factors within an organization (e.g., leadership, staffing, and individual characteristics) that may be associated with implementation processes and outcomes. Many teams operate within the inner context, as teams within organizations. Within the inner organizational context, different types of teams may be identified. For example, within a hospital, there may be surgical teams, care teams on specific units, and administrative teams. For teams within organizations, team characteristics can be considered part of the inner context, alongside individual and organizational characteristics.
Outer Context
The outer context refers to factors in the environment outside the organization, such as policy/regulatory context and patient/client population characteristics that may be associated with implementation processes and outcomes. Some teams exist within the outer context and shape service environments, funding, and inter-organizational networks. For example, in the United States, state service systems may be characterized by functions or focus areas such as public health, behavioral health services, adult services, child services, funding, and contracting. Individuals from different divisions may work together as a team on initiatives such as creating dedicated EBP funding streams (Crable et al., 2022). Similarly, state leadership teams may be created to improve public health through cross-system collaboration (Brown et al., 2023).
Bridging Factors
While teams can operate within outer or inner contexts, some teams span system and organization levels and can be conceptualized as engaging in bridging or being bridging factors (Lengnick-Hall et al., 2021). Bridging factors include “relational ties, formal arrangements, and processes” that link the inner and outer context (Lengnick-Hall et al., 2021, p. 2), such as research-community partnerships (Brookman-Frazee et al., 2016, 2020). For example, in one study, community and academic partners interacted to develop system-level contracting arrangements to support implementation of EBPs for substance use disorders (Crable et al., 2022). These contracting arrangements are a bridging factor formally connecting the outer context of the system to the inner context of community-based organizations.
Interconnections and Linkages
EPIS also explicitly includes “interconnections, interactions, linkages, and relationships” within and across domains. In contrast to bridging factors which formally link outer and inner contexts, interconnections and linkages are more informal and can exist within and across domains, between individuals, or between formal entities such as groups or organizations. Interconnections and linkages can shape implementation processes and outcomes through individuals’ influence on one another, personal relationships, and interaction histories.
Implementation Phases
The EPIS phases provide a way to stage team activities through the implementation process. This may include the creation of implementation support teams and the act of “teaming” during implementation (i.e., a dynamic “way of working that brings people together to generate new ideas, find answers, and solve problems”; Edmondson, 2012, p. 24). The phases also provide a framework for considering planned and ad hoc changes to team configuration and/or relevant teams over time and across phases (Becan et al., 2018). Lastly, EPIS phases are recursive and can be used to identify potential team challenges during each phase and consider additions or revisions to team-based implementation strategies as teams evolve.
Case Examples Illustrating Application of the EPIS Framework
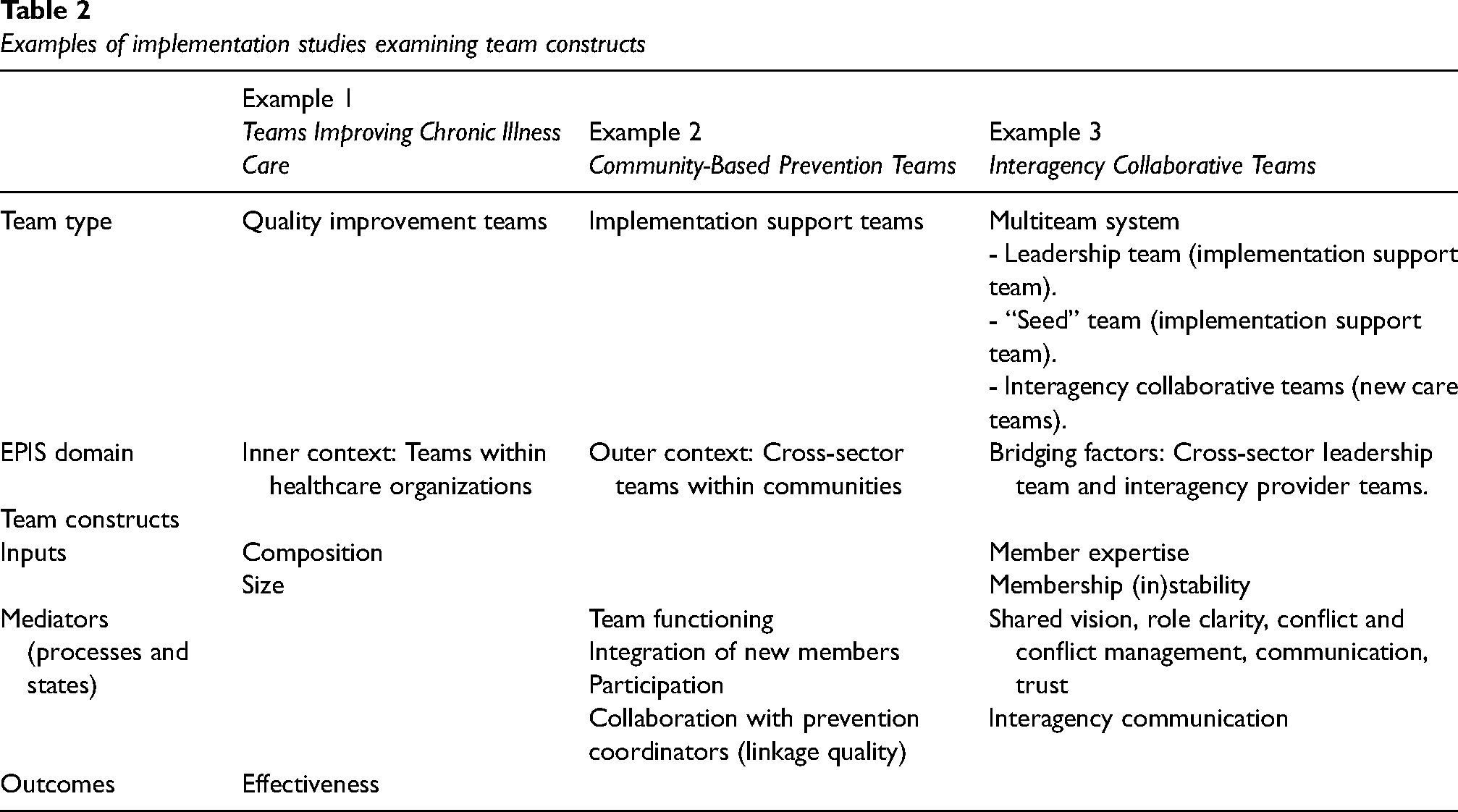
In the following section, we describe three case examples of implementation studies involving teams, situate the teams within the EPIS framework, and describe how team constructs influenced implementation processes and/or outcomes. Table 2 lists the type of teams studied, their position within EPIS domains, and the team constructs examined in each study.
Examples of implementation studies examining team constructs
Example 1: Teams Improving Chronic Illness Care (Quality Improvement Teams)
Shortell et al. (2004) assessed healthcare system teams participating in a learning collaborative to improve chronic care management using quality improvement methods (Cretin et al., 2004). The collaborative was sponsored by an external organization with the goal of creating a network and empowering teams to make effective changes. Participating healthcare organizations were expected to create interdisciplinary teams supported by organizational leadership (Cretin et al., 2004). The teams in this example were situated within the inner context of healthcare organizations with strong interconnections with the collaborative, a bridging factor.
The study tested associations between team composition (i.e., presence of champion and proportion of physicians), size, effectiveness, and the number of changes made and the depth of changes (i.e., expert ratings of expected impact on patient outcomes; Shortell et al., 2004). The reported presence of a team champion and a greater proportion of physicians were positively associated with team members’ ratings of effectiveness. Team composition was not directly associated with the number or depth of changes. Team size was negatively associated with effectiveness and curvilinearly associated with the depth of changes, with a positive association initially and then a negative association as teams became larger (>10 members). Team effectiveness was positively associated with both the number and depth of changes, indicating that teams who consider themselves more effective take more actions (and more impactful actions) to improve care (Shortell et al., 2004). Importantly, team-level constructs in this study were examined alongside organization-level measures (e.g., organizational culture). These findings suggest that team- and organization-level constructs have unique influences on implementation, even when teams are situated within the inner context of an organization.
Example 2: Community-Based Prevention Teams (Implementation Support Teams)
The PROSPER study created teams in participating communities to select, implement, and sustain evidence-based prevention programming for youth and families. Prevention teams included Cooperative Extension Service educators, representatives from schools and community agencies, parents, and youth. They worked closely with academic researchers and prevention coordinators who provided consultation and technical assistance. The PROSPER model resulted in high implementation quality that was sustained over time (Spoth et al., 2007, 2011).
Prevention teams are conceptualized as part of the outer context, with strong interconnections/linkages to academics and prevention coordinators who act as intermediaries (bridging factors). Although individual members of the prevention teams were part of organizations, the teams themselves were not situated within any one organization or inner context. Prevention teams were formed early in Exploration and remained active through Preparation, Implementation, and Sustainment (Spoth et al., 2007).
Perkins et al. (2011) examined whether prevention team functioning during early phases predicted sustainability planning two years later. Using a global measure of team functioning, they found strong positive correlations between team functioning and the team's expertise for sustainment and funding plans, as rated by both team members and external consultants (Perkins et al., 2011). Integration of new team members, team participation, and perceptions of leadership and community support was also associated with later expertise and funding plans (Perkins et al., 2011). Another study from this project found that the quality of collaboration between the prevention team and prevention coordinator predicted later team functioning (Chilenski et al., 2016). These findings indicate that the quality of linkages between the outer context and bridging factors influences the functioning of teams, which in turn influences EBP sustainment.
Example 3: Interagency Collaborative Teams (Multiteam System)
The Interagency Collaborative Team (ICT) model is an example of how implementation support teams, new care teams, and their interactions in a multiteam system can be leveraged to support EBP implementation (Aarons et al., 2014; Hurlburt et al., 2014). The ICT model was used to implement an EBP for child neglect in a large urban county. Teams were created within and across levels to support implementation, funded by a large investment from a philanthropic organization.
Core components of the ICT model included creating a cross-level, interagency leadership team focused on practice change, a “seed team” trained and certified to be a local training and coaching resource, and service-level interagency collaborative teams that were trained by the seed team and delivered the EBP across the service area. Although each team had its own specific goals, the teams needed to interact directly and interdependently with one another to achieve the superordinate goal of EBP implementation (Hurlburt et al., 2014).
The leadership team was a bridging factor linking the outer and inner context. It was composed of representatives from the philanthropic funder, child welfare system, and advocacy organizations (outer context), as well as representatives from community-based service agencies (inner context). It had strong linkages to other bridging factors, including academic partners and intervention developers. The seed team had members from two organizations and the interagency collaborative teams were comprised of providers from two or more organizations working under a common supervisor to provide services across different regions. Both the seed team and the interagency collaborative teams were composed of staff from multiple agencies to distribute local expertise and enhance interagency communication (Hurlburt et al., 2014). The ICT model was successful in implementing the EBP, which has been sustained for over six years.
Each team played a critical role in the multiteam system created by the ICT model, with their importance and influence varying across implementation phases (Aarons et al., 2014). During the Exploration phase, the funder collaborated with the child welfare system, community-based provider organizations, and advocacy organizations to identify population service needs, select an EBP, and create a vision for sustained evidence-based services for child neglect. During the Preparation phase, the cross-level leadership team developed strategies and processes to support implementation and sustainment. The seed team was developed during the Implementation phase and was closely linked to EBP developers and key stakeholders, especially early in implementation. Throughout the Implementation phase, the seed team provided ongoing supervision and coaching for newly trained interagency collaborative teams. Contracts, funding, and detailed statements of work were bridging factors that formalized and strengthened the multiteam system (Aarons et al., 2014; Hurlburt et al., 2014). Informal connections between individuals varied in nature and degree and influenced team interactions.
Key themes identified during implementation included the quality of collaboration between key stakeholders, communication within and between teams, and leadership (Hurlburt et al., 2014). At times, differences in expectations and ambiguity in roles, responsibilities, and authority created power dynamics, conflicts, and strained relationships (Aarons et al., 2014; Hurlburt et al., 2014). Without a clear communication structure, breakdowns occurred, and some stakeholders reported feeling “out of the loop” or unsure who to contact with questions. Critical to overcoming these challenges were a clear goal for EBP sustainment, a shared vision, realistic expectations for implementation, and a willingness to persevere (Aarons et al., 2014). Although complex, the process of contract negotiation was effective in clarifying roles and responsibilities and resolving fiscal and operational concerns. Early successes in implementation helped reduce power struggles, increase trust, and facilitate communication and joint problem-solving (Aarons et al., 2014; Hurlburt et al., 2014). Results suggest that explicit processes for communication and conflict management, a shared problem-solving orientation, and commitment to a shared vision are critical to teams’ capacity to provide the structural and process supports needed for implementation success (Aarons et al., 2014; Hurlburt et al., 2014).
Future Directions
Conducting Rigorous Implementation Research with Teams
Teams have received little attention in implementation science. Incorporating teams into TMFs may increase attention to their importance and provide new team-level targets for implementation strategies. Increasing attention to teams in implementation research must be accompanied by efforts to improve the description of teams and reporting of team-level findings. An ongoing systematic review of teams in implementation research found that the term “team” was often used without any description and sometimes used to refer to groups that did not actually constitute a team (e.g., staff in an organization who work independently; McGuier et al., 2021, 2022). Better description and reporting of team structures, processes, and outcomes will allow us to identify and replicate associations between team constructs and implementation outcomes to isolate robust predictors that can be targeted in implementation efforts.
Measurement of team constructs should be informed by existing theory and research. While the IMOI framework is a helpful starting point, other models of team effectiveness provide more specific theories about drivers of team effectiveness (e.g., Hackman, 2012; Tannenbaum & Salas, 2020), developmental processes in teams (e.g., Tuckman, 1965), and team interventions (Hackman & Wageman, 2005; Tannenbaum & Cerasoli, 2013); these models may be useful in developing and testing specific research questions. An array of well-validated measures of team constructs are available, including measures that are aligned with theories of team effectiveness (e.g., Mathieu et al., 2020; see Marlow, Bisbey et al., 2018; Valentine et al., 2014). Team constructs can also be assessed through observational measures and unobtrusive methods using existing data. For example, natural language processing methods can be applied to routinely produced materials (e.g., agendas, notes, and recordings/transcripts) to evaluate team functioning during meetings. Improving the measurement of team constructs is critical to enhancing the rigor of research on teams and implementation.
Implementation Strategies Targeting Teams
In team-based settings, implementation strategies that target team effectiveness may improve implementation outcomes (see Figure 2). Teams are promising targets because they can remain relatively stable even when individual members leave or change positions. Teams may also change more quickly than organizations. In addition, strategies that improve care team effectiveness may improve clinical outcomes above and beyond the effects of the EBP. However, implementation strategy compilations do not provide sufficient guidance for how to target the team level or include strategies to improve team effectiveness (Powell et al., 2015).
Implementation strategies targeting team effectiveness are intended to change how teams work together (i.e., teamwork) and can be applied to teams engaged in diverse taskwork. These strategies may take three forms: (a) existing implementation strategies that create teams, (b) existing implementation strategies that can be modified to target teams, and (c) novel implementation strategies that draw from team development interventions (TDIs) and aim to improve teams. Some strategies included in the Expert Recommendations for Implementing Change (ERIC) compilation involve the creation of teams (e.g., create new clinical teams, organize clinician implementation team meetings; Powell et al., 2015). However, little guidance is provided about how to apply these team-based strategies or evaluate their effectiveness in the context of implementation. Future research could examine team structure and processes as potential moderators or mediators of the effectiveness of these strategies, as well as ways to support new teams over time and across different phases of the implementation process. Other frequently used ERIC strategies could be easily adapted to target the team level. For example, audit and feedback could be leveraged to increase outcome interdependence in teams (i.e., attention to team vs. individual outcomes). Alongside support for collaboration, this strategy may improve work performance (Markon et al., 2017).
Another approach is to add or incorporate effective TDIs. TDIs can improve team functioning and patient outcomes in real-world settings (Hughes et al., 2016; Klein et al., 2009; McCulloch et al., 2011; McEwan et al., 2017; Miller et al., 2018; Salas, DiazGranados et al., 2008; Shuffler et al., 2018). Two well-established types of TDIs are team training (Salas, DiazGranados et al., 2008) and team building (Klein et al., 2009; Miller et al., 2018). Team training targets team members’ knowledge, skills, and attitudes through strategies such as team self-correction, coordination training, and cross-training and is effective in improving team functioning (Hughes et al., 2016; Salas, DiazGranados et al., 2008; Sheppard et al., 2013; Weaver et al., 2014). Team building targets goal-setting, relationship management, role clarification, and/or problem-solving and is effective in improving behavioral processes and affective states (Klein et al., 2009; Miller et al., 2018). Other effective TDIs include team debriefs (Tannenbaum & Cerasoli, 2013), team coaching (Hackman & Wageman, 2005), team charters (Sverdrup & Schei, 2015), and team leadership (Burke et al., 2011). For more information on effective TDIs, see Buljac-Samardzic et al. (2020), Lacerenza et al. (2018), and Shuffler et al. (2011, 2018).
Despite strong evidence for TDIs, they have not been considered in the implementation TMFs. TDIs can be delivered alongside implementation strategies or integrated into specific implementation strategies. For example, an implementation effort could include training providers in the EBP (implementation strategy) as well as training in communication skills (TDI). As another example, the organization of clinical implementation team meetings (implementation strategy) could incorporate the creation of team charters (TDI). In this case, the TDI adds additional structure to enhance the effectiveness of the implementation strategy. Team processes and states should be considered as possible mechanisms of effectiveness when testing team-based implementation strategies.
To date, there has been limited attention to teamwork processes and their relevance to implementation strategies. Ongoing research on teams and team-based models in healthcare highlights the importance of teams in healthcare settings. Incorporating evidence-based team interventions may improve the effectiveness of implementation strategies. A new research center (P50MH126231) and ongoing research studies (Kolko et al., 2022; McGuier, Aarons, Wright et al., 2023) focused on developing and testing novel team-based strategies will advance understanding of these implementation strategies.
Conclusions
Effective teams are critical to high-quality healthcare. Despite the increasing use of teams to provide services and reliance on teams to implement new practices, teams, and team-level constructs are neglected in implementation TMFs. We integrated teams and team constructs into the EPIS framework, demonstrating how EPIS can be applied to advance our understanding of teams and implementation. We encourage implementation scientists to consider how the complexity of teams and team dynamics impact implementation research and practice. Integration of team effectiveness research, including testing implementation strategies targeting teams, can optimize the efficiency and effectiveness of implementation efforts in team-based service settings.
Footnotes
Acknowledgments
The conceptualization of team-based implementation strategies was informed by the development of the Implementation Science and Team Effectiveness in Practice (IN STEP) Children's Mental Health Research Center (P50MH126231; PIs: Brookman-Frazee [contact], Aarons).
Authors’ contributions
EAM and GAA conceptualized the manuscript. EAM led manuscript development and writing. DJK, NAS, LBF, CBW, CSB, and GAA reviewed multiple drafts of the manuscript and provided critical input and editing. CTY contributed to manuscript revisions. All authors approved the final manuscript.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GAA is a member of the Implementation Research and Practice Editorial Board; all decisions on this paper were made by other editors. The authors declare that they have no other conflicting interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse, National Institute of Mental Health, and Agency for Healthcare Research and Quality (grant numbers DA049891, MH123729, MH124914, MH126231, and HS026862).