
Abstract
Background
Communication research demonstrates that messages often have unintended consequences, but this work has received limited attention in implementation science. This dissemination experiment sought to determine whether state-tailored policy briefs about the behavioral health consequences of adverse childhood experiences (ACEs), compared to national policy briefs on the topic, increased state legislators’/staffers’ perceptions of the policy brief relevance and parental blame for the consequences of ACEs, and whether effects differed between Democrats and Republicans.
Method
A preregistered, web-based survey experiment with U.S. state legislators/staffers was conducted in 2021 (n = 133). Respondents were randomized to view a policy brief about the behavioral health consequences of ACEs that included state-tailored data (intervention condition) or national data (control condition) and then answered survey questions. Dependent variables were perceived policy brief relevance and parental blame for the consequences of ACEs.
Results
The mean policy brief relevance score was 4.1% higher in the intervention than in the control condition (p = .24), but the mean parental blame score was 16.5% higher (p = .02). When outcomes were dichotomized, 61.2% of respondents in the intervention condition rated parents as “very much to blame” for the consequences of ACEs compared to 37.1% in the control condition (p = .01). When the sample was stratified by political affiliation, the effect of the state-tailored policy brief on parental blame was larger in magnitude among Democrats and not significant among Republicans. The intervention policy brief increased the mean parental blame score by 22.8% among Democrats relative to the control policy brief (p = .007) and doubled the proportion rating parents as “very much to blame” (52.2% vs. 26.1%, p = .03).
Conclusions
Despite limited statistical power, state-tailored policy briefs significantly increased state legislators’/staffers’ perceptions of parental blame for the behavioral health consequences of ACEs, relative to a policy brief with national data. Unintended messaging effects warrant greater attention in dissemination research and practice.
Plain Language Summary
Prior studies have tested the effects of dissemination strategies on policymakers’ engagement with research evidence. However, little research has assessed the potential unintended consequences of disseminating evidence to policymakers. This knowledge gap is important because a large body of communication research has found that messages often have negative and unintended effects. This paper adds to the literature on disseminating evidence about behavioral health issues to policymakers. A web-based survey experiment was conducted in which U.S. state legislators/staffers were randomized to view a policy brief about adverse childhood experiences (ACEs) that was tailored to present data from their state (intervention condition) or a policy brief that presented national data and then completed a survey. Legislators/staffers who viewed the state-tailored policy brief perceived the brief as slightly more relevant, but also rated parents as being significantly more to blame for the behavioral health consequence of ACEs. The effect of the state-tailored policy brief on parental blame is an unintended messaging effect that signals cause for caution when disseminating evidence about ACEs to policymakers and other practice audiences. More broadly, the findings highlight a need to consider unintended messaging effects in dissemination research and practice.
Introduction
Dissemination research—defined as the study of the packaging and communication of research evidence for public health and clinical practice audiences (National Institutes of Health, 2022)—is underdeveloped in the field of implementation science (Ashcraft et al., 2020; Baumann et al., 2022; Brownson et al., 2018; Purtle, Marzalik, Halfond, et al., 2020). Dissemination research that informs how evidence about mental health and substance use (i.e., behavioral health) issues is communicated to policymaker audiences is important given the influence that policymakers have on service systems and the structural determinants of behavioral health (Dopp & Lantz, 2020; Purtle et al., 2017; Purtle, Nelson, Bruns, et al., 2020; Purtle, Nelson, Counts, et al., 2020). Policymaker-focused dissemination research has historically been understudied in implementation science (Hoagwood et al., 2020; Purtle et al., 2015).
However, recent field experiments have tested the effects of manipulating the framing of research evidence on U.S. policymaker engagement with research evidence (e.g., measured by email view and link click rates) and survey-based experiments have tested framing effects on support for evidence-based policies (Brownson et al., 2011; Levine, 2020, 2021; Long et al., 2021; Niederdeppe et al., 2016, 2021; Purtle et al., 2022; Scott et al., 2022; Winett et al., 2021). Although this work contributes a limited evidence base that can inform dissemination practice, it does not shed light on any potential unintended consequences of dissemination. Both of these areas have received very limited attention in dissemination research, among policymakers or other practice audiences.
Petty and Cacioppo’s (1986) elaboration likelihood model of persuasive communication posits that the perceived relevance of dissemination materials is a key construct that spurs engagement with, and cognitive processing of, research evidence. Increased cognitive engagement with dissemination materials, prompted by heightened perceived relevance, may have the benefit of changing knowledge and attitudes in ways that are aligned with evidence (Purtle, Marzalik, Halfond, et al., 2020). However, such cognitive engagement could also have unintended consequences.
The use of heuristics (i.e., cognitive shortcuts) when processing evidence is common and can lead to overly simplistic conceptualizations of the causes of complex problems and negative attitudes toward social groups related to the problem (Cairney & Kwiatkowski, 2017; Mousavi, 2018). A large body of communication research has documented backlash, or “boomerang,” effects in which messages have unintended consequences among some segments of an audience (Byrne & Hart, 2009; McGinty et al., 2018). For example, a 2019 survey-based experiment with state legislators found that the inclusion of narratives about people who would benefit from evidence-based childcare policies in evidence summaries decreased support for these policies among Republicans, while it increased support among Democrats (Winett et al., 2021).
One domain of behavioral health evidence that could be highly susceptible to unintended messaging effects is evidence about adverse childhood experiences (ACEs, e.g., child abuse and neglect, exposure to violence in the home and community; Ellis & Dietz, 2017; Felitti et al., 1998). ACEs are well-established risk factors for behavioral health problems and suicide in adulthood (Afifi et al., 2008; Hughes et al., 2017). Public-, provider-, and policymakers-targeted communication campaigns have sought to spread evidence about ACEs. However, some researchers and practitioners have expressed concerns that haphazard dissemination of ACEs evidence could have unintended consequences (Bethell et al., 2017; Campbell, 2020; Lacey & Minnis, 2020; Macvarish & Lee, 2019; McEwen & Gregerson, 2019).
Recent public opinion research provides some support for these concerns. A 2019 public opinion survey of U.S. adults found that 62.5% perceived parents as “very much to blame,” for the consequences of ACEs (Purtle, Nelson, and Gollust, 2021)—despite the survey emphasizing that ACEs include experiences outside the home (e.g., community violence). A 2020 public opinion experiment found that evidence about the economic impacts of ACEs increased support for policies to address ACEs, but also increased parental blame for the consequences of ACEs (Gollust et al., 2022). These findings are consistent with public opinion research indicating parental blame for childhood obesity (Wolfson et al., 2015) and maternal blame for developmental issues (Richardson et al., 2014; Sharp et al., 2018).
Study Aims
This Short Report presents results from a survey-based dissemination experiment conducted with U.S. state legislators and staffers about the evidence of ACEs being risk factors for behavioral health conditions. The experiment was the final component of a multiple-year dissemination research project focused on communicating evidence about ACEs (Gollust et al., 2022; Purtle et al., 2023; Purtle, Nelson, Gebrekristos et al., 2022; Purtle, Nelson, & Gollust, 2021; Purtle, Nelson, Srivastav et al., 2021). Among other project findings, a field experiment with state legislators found that state-tailored dissemination materials increased engagement with evidence among Democrats but not Republicans (Purtle, Nelson, Gebrekristos et al., 2022). The current study's aims were to (a) determine whether state-tailored policy briefs increase the perceived relevance of policy briefs compared to national policy briefs, (2) determine whether state-tailored briefs affect perceptions of parental blame for the behavioral health consequences of ACEs compared to national policy briefs, and (c) assess whether the direction and magnitude of these effects differ between Democrats and Republicans.
Methods
A preregistered (https://osf.io/cgh64), clustered randomized survey-based dissemination experiment with U.S. state legislators/staffers was conducted. Complete details about the cluster randomization approach and design are provided elsewhere (Purtle, Nelson, Gebrekristos et al., 2022). In short, each U.S. state was randomized to one-of-three policy brief conditions. The intervention policy brief contained state-tailored data about rates of ACEs and state-tailored economic evidence about the costs of ACEs, the enhanced control policy brief contained state-tailored data about rates of ACEs but no economic evidence, and the control policy brief included national data about rates of ACEs and no economic evidence (see Supplemental File A, e.g., policy briefs). The study was approved by the Drexel University Institutional Review Board.
Procedure
All U.S. state legislators were postmailed a one-page letter providing information about the survey and then three email invitations were sent (one per week). The survey was fielded between April 8, 2021, and May 2, 2021. Recruitment materials stated that the survey could be completed by the legislator or a staffer. The survey was sent to 6,153 state legislative officials with valid email addresses in the KnowWho legislative database and completed by 133 respondents (response rate = 2.16%; CONSORT Diagram is Figure 1) from 40 states.

CONSORT Flow Diagram
After informed consent and introductory survey questions, the survey displayed the one-page policy brief that corresponded with the condition to which the respondent's state was randomized. After viewing the policy brief, respondents answered survey questions about the policy brief and their attitudes related to ACEs.
Outcomes and Measures
The independent variable was a categorical indicator of the policy brief condition to which the respondent was randomized. In the preregistration, we planned to combine the two state-tailored conditions and compare results to the control condition and compare all three conditions separately. Because the response rate was lower than anticipated, and thus sample sizes were small across the three study conditions, the analyses reported here combined the two state-tailored conditions (hereafter referred to as the intervention condition).
The primary dependent variable measured the perceived relevance of the policy brief. This was the sum of two 7-point Likert scale items—adapted from prior work (Brownson et al., 2011; Purtle, Dodson, et al., 2018)—which assessed the extent to which the brief was perceived as relevant to respondents “in [their] work” and “residents in [their] state” (1 = Not relevant, 7 = Very relevant; α = .70, r = .56). The secondary dependent variable measured parental blame for the behavioral health consequences of ACEs, also adapted from prior work (Barry et al., 2013; Wolfson et al., 2015). This 7-point Likert scale item assessed the extent to which “parents of children who have experienced [ACEs] are to blame for mental health and substance use problems their children develop as adults” (1 = Not all to blame, 7 = Completely to blame). Consistent with how similar measures have been used in prior work (Purtle, Nelson, & Gollust, 2021), we also created dichotomous measures of the policy brief being perceived as “very relevant” (summed score ≥12) and parents being perceived as “very much to blame” (score ≥ 6).
Covariates included a range of demographic characteristics, including whether the survey was being completed by a legislator or staffer. Covariates also assessed whether the respondent had heard of ACEs prior to the survey and whether the respondent had seen the policy briefs sent during the field experiment portion of the study (Purtle, Nelson, Gebrekristos et al., 2022). These questions were asked before the policy brief was displayed.
Analysis
Consistent with prior dissemination experiments with state legislators (Brownson et al., 2011; Long et al., 2021; Niederdeppe et al., 2016, 2021; Purtle et al., 2022; Scott et al., 2022; Winett et al., 2021) and methodology standards in the field (De Boer et al., 2015; Mutz et al., 2019), our primary analytic approach was unadjusted and used independent sample two-tailed t tests to compare means and chi-square tests to compare differences in dichotomized outcomes. Our secondary analytic approach adjusted for demographic differences across the study conditions, significant at p < .05, in logistic regression models in which the dichotomized outcomes were the dependent variable. We also stratified the sample by political party affiliation and repeated the analyses to assess differences in the intervention effect between Democrats and Republicans.
Results
The sample was comprised of 98 respondents from the intervention condition (state-tailored policy brief) and 35 from the control condition (national policy brief). Table 1 shows demographic characteristics across the study conditions. The proportion of respondents that were legislators, as opposed to staffers, was significantly higher in the intervention than in the control condition (78.6% vs. 57.1%, p = 0.01) as was the proportion with a postgraduate degree (62.1% vs. 27.3, p < .001). Eighty-three percent of respondents had previously heard of ACEs, with no significant difference in the proportion between the study conditions.
Demographic and Baseline Characteristics of Experiment Participants
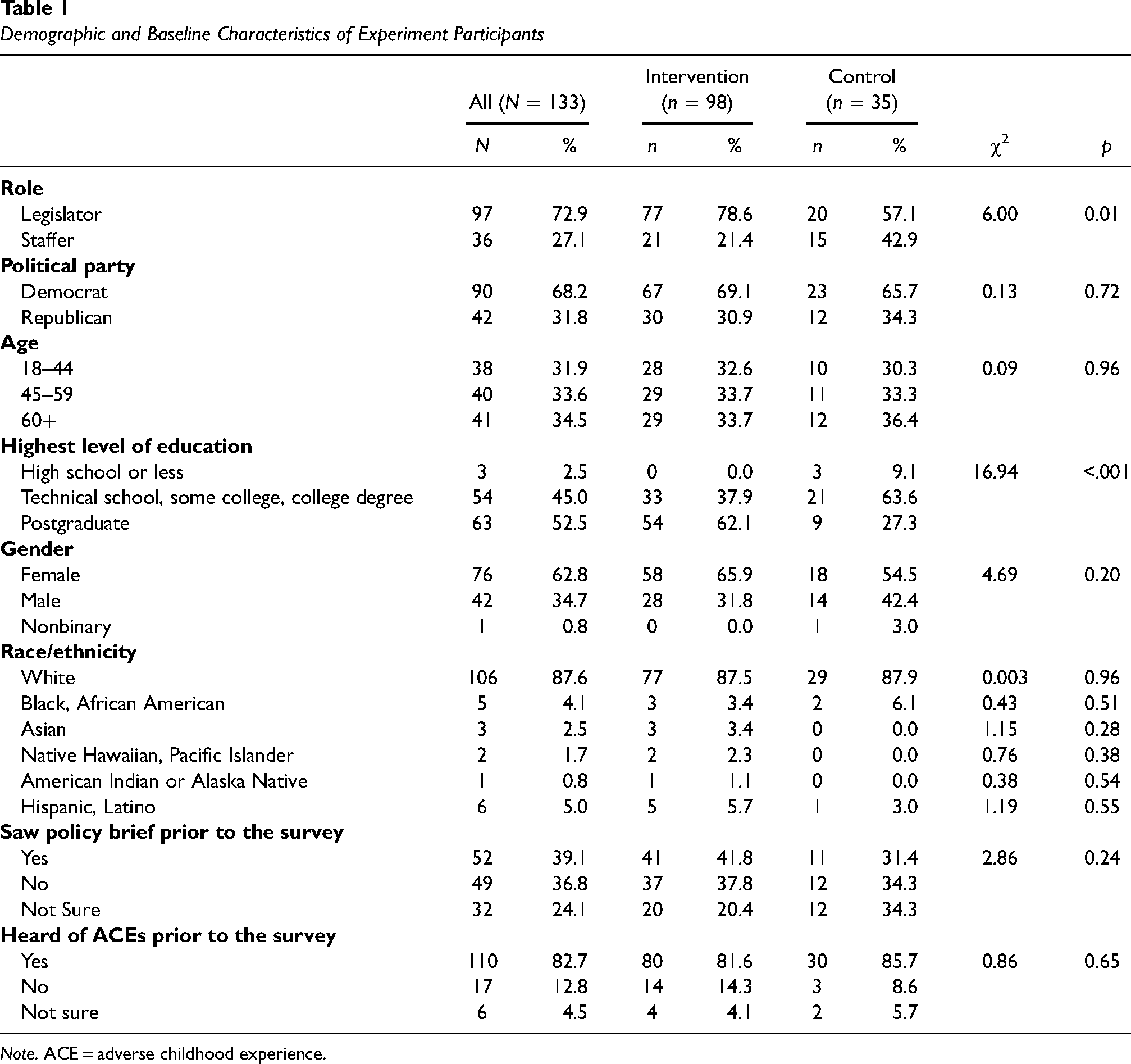
Note. ACE = adverse childhood experience.
Main Effects of State-Tailored Policy Briefs on Perceived Relevance and Parental Blame
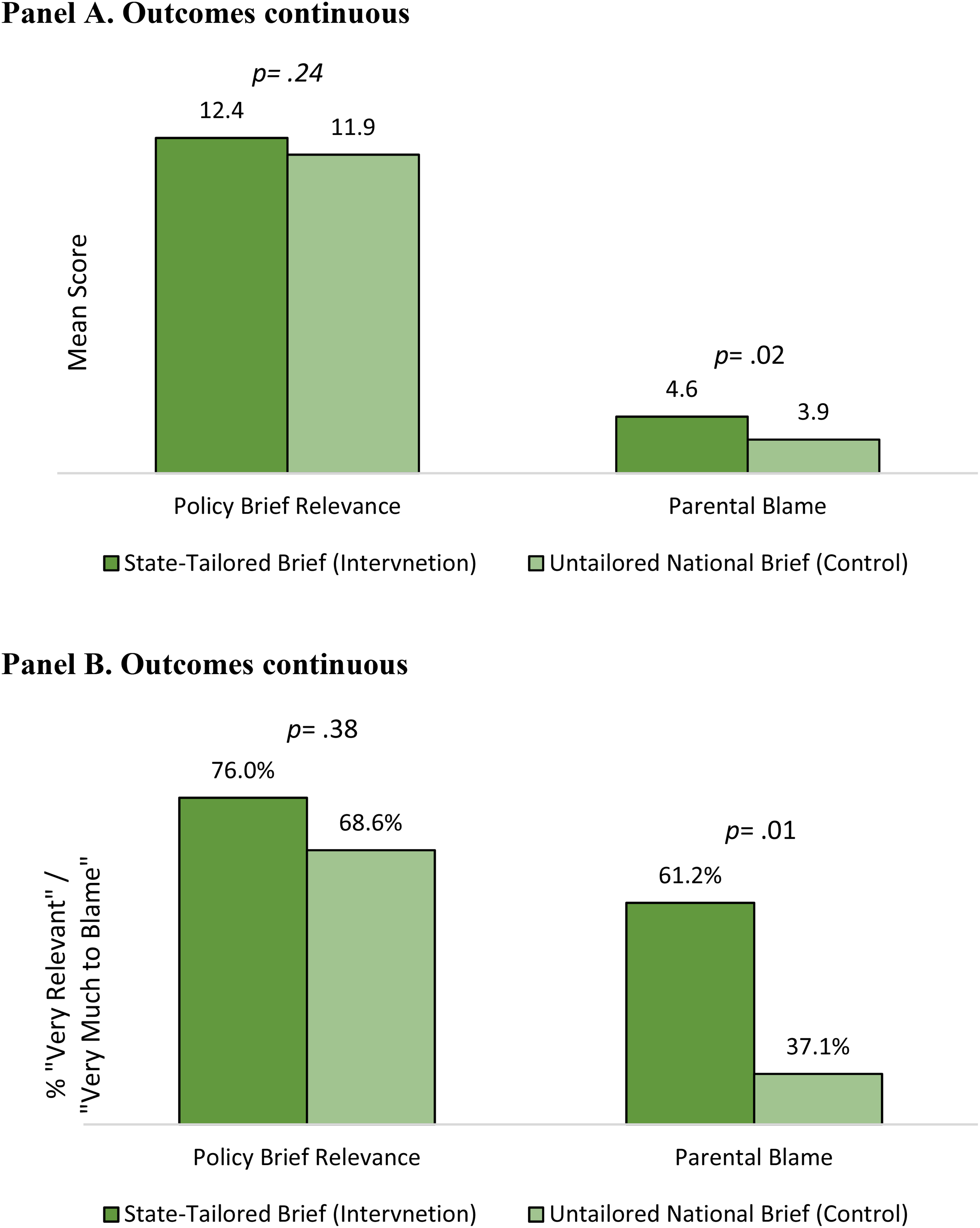
The state-tailored policy brief slightly increased the perceived relevance of the brief but also significantly increased parental blame for the behavioral health consequences of ACEs. The mean relevance score was 4.1% higher in the intervention than in the control condition (12.4 vs. 11.9, t = 1.12, p = .24) and the mean parental blame score was 16.5% higher (4.6 vs. 3.9, t = 2.37, p = .02; Figure 2A). The magnitudes of these differences were large when the variables were dichotomized (Figure 2B). Among intervention condition respondents, 76.0% rated the policy brief as “very relevant” compared to 68.6% in the control condition (χ2 = 0.75, p = .76) while 61.2% of respondents in the intervention condition rated parents as “very much to blame” compared to only 37.1% in the control condition (χ2 = 6.04, p = .01). The effect of the state-tailored policy brief on parents being perceived as “very much to blame” remained significant after adjusting for demographic differences between the study conditions (adjusted odds ratio [AOR] = 3.11; 95% CI = 1.23, 7.90, p = .02; Table 2).
Unadjusted Experiment Results (N = 133)
Adjusted Effects of State-Tailored Policy Briefs (Intervention) on the Policy Brief Being Perceived as “Very Relevant” and Parents Being Perceived as “Very Much to Blame” for the Behavioral Health Consequences of ACEs, Relative to an Untailored National Policy Brief (Control)

Note. ACE = adverse childhood experience; AOR = adjusted odds ratio; CI = confidence interval.
Logistic regression results. Reference group = respondents assigned to the control condition. Models adjusting for legislator/staffer role and the highest level of education, variables that differed significantly between the intervention and control conditions. Models 1–3 run separately. “Very relevant” = score ≥12 on a 14-point scale, “very much to blame” = score ≥ 6 on a 7-point scale.
Effects of Policy Briefs, Stratified by Political Party Affiliation
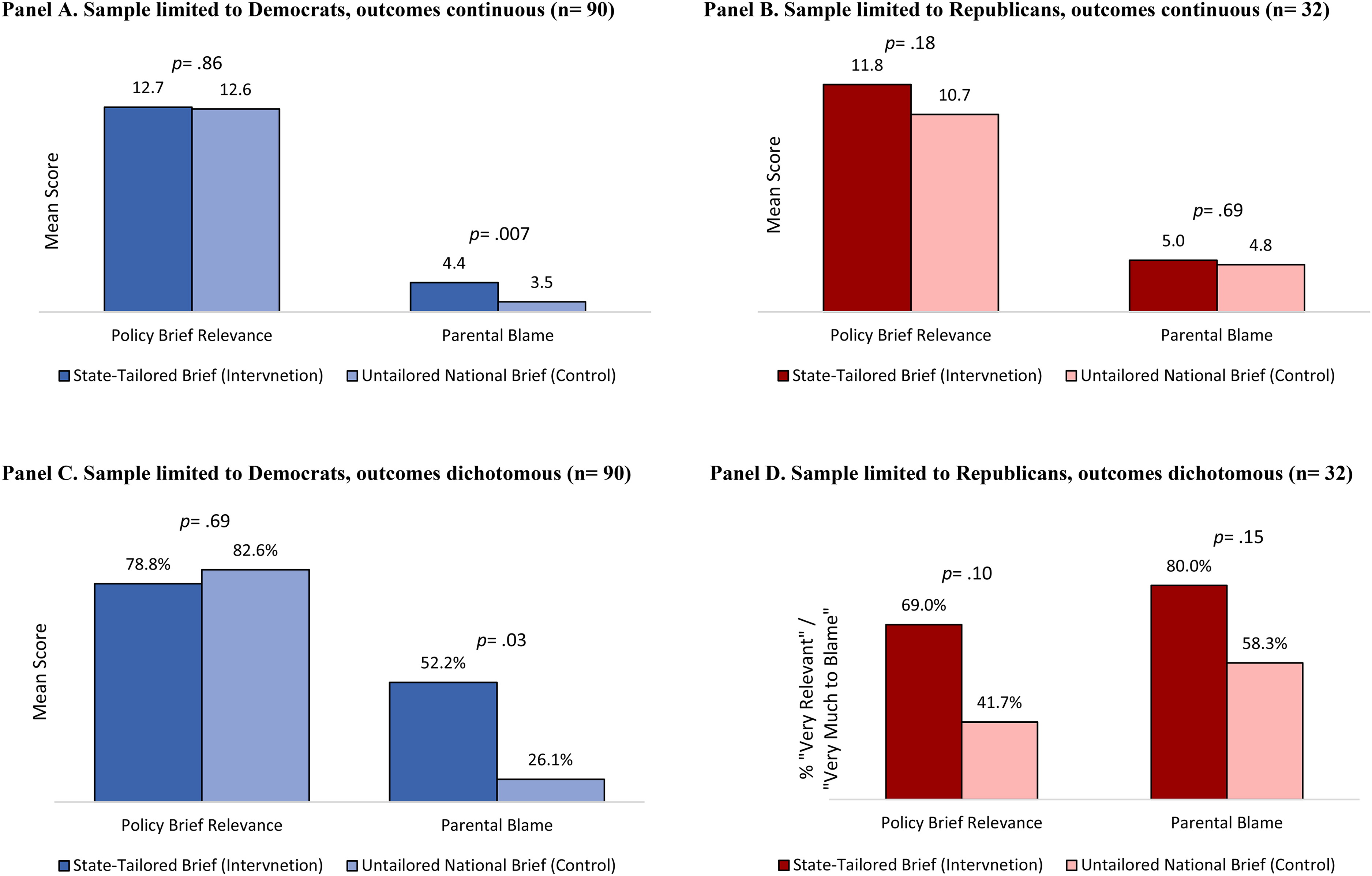
When analyses were limited to Democrats (n = 90), perceptions of policy brief relevance were nearly identical between the intervention and control conditions (mean = 12.7 vs. 12.6, t = 0.18, p = .86; proportion rating the brief as “very relevant” 78.8% vs. 82.6%, χ2 = 0.15, p = .69). However, the intervention increased parental blame among Democrats (Figure 3A and C). The mean parental blame score was 22.8% higher among Democrats in the intervention than in the control condition (4.4 vs. 3.5, t = 2.74, p = .007) and the proportion rating parents as “very much to blame” was also significantly higher (52.2% vs. 26.1%, χ2 = 4.72, p = .03). This effect persisted after adjusting for demographic differences between the study conditions (AOR = 4.70; 95% CI = 1.32, 16.86, Table 2).
Unadjusted Experiment Results Stratified by Political Party Affiliation of the Respondent
When analyses were limited to Republicans (n = 42), the intervention increased the perceived relevance of the policy brief, although not significantly. The rating of policy brief relevance was 7.9% higher in the intervention than control condition among Republicans (mean = 11.8 vs. 10.9, t = 1.37, p = .18) and 69.0% rated the brief as “very relevant” in the intervention condition compared to 41.7% in the control condition (χ2 = 2.65, p = .10; Figure 3B and D). The mean ratings of parental blame were nearly identical in the intervention and control conditions (mean = 5.0 vs. 4.8, t = 0.40, p = .69). However, the proportion of Republicans rating parents as “very much to blame” was notably higher in the intervention than in the control condition (80.0% vs. 58.3%, χ2 = 2.08, p = .15).
Discussion
Despite a small sample size and limited statistical power, we found that state-tailored policy briefs significantly increased legislators’/staffers’ perceptions of parental blame for the behavioral health consequences of ACEs, relative to an untailored policy brief with national data. Among Democrat legislators/staffers, we found that the state-tailored policy brief more than quadrupled the odds of a respondent perceiving parents as “very much to blame” for these consequences of ACEs.
We found some evidence that state-tailored policy briefs are perceived as more relevant than national policy briefs among Republicans, but these differences were not statistically significant (which is not surprising given the small sample size of Republicans, n = 42). While we observed that state-tailored policy briefs had almost no effect on perceived relevance among Democrats, levels of perceived relevance were high in the intervention and control conditions (means 11.6 and 11.7, respectively, on a 14-point scale) and the lack of difference could be due to a ceiling effect. High ratings of policy brief relevance among Democrats are consistent with prior research indicating that Democrat state legislators greatly value research evidence about behavioral health (Purtle, Dodson, et al., 2018; Purtle, Lê-Scherban, et al., 2018).
The finding that certain framings of ACE evidence can produce parental blame is consistent with results from the aforementioned public opinion experiment which found that framing ACE evidence in economic terms generated policy support but also parental blame (Gollust et al., 2022). Taken together, these results signal cause for caution when disseminating evidence about ACEs to help ensure that this evidence does not produce or perpetuate parental blame. In dissemination practice, such caution could be expressed by emphasizing that many ACEs occur outside of the home that structural inequities contribute to ACEs and the intergenerational nature of ACEs and historical trauma (Gehlert & Cuestas, 2021). However, such messages should also be tested to help ensure that they do not produce unintended consequences.
Strengths and Limitations
A strength of the study is its randomized design, which enhances internal validity. A key limitation of the study, however, is its low response rate of 2.16%, which creates uncertainty about external validity. The sample skewed Democrat (68.2% of respondents compared to 44.7% of state legislative offices at the time of the study; National Conference of State Legislatures, 2022) and 83% of respondents had heard of ACEs prior to the survey. This proportion having heard of ACEs is substantially higher than that among state legislators in a 2017 survey (33%; Purtle et al., 2019) and among the general public in a 2020 survey (13%; Gollust et al., 2022). Thus, is likely that the sample overrepresents legislators/staffers who are knowledgeable about ACEs. The fact that the state-tailored policy brief had the effect of increasing parental blame among these policymakers—who presumably rely less on heuristics when engaging with evidence about ACEs, given their prior knowledge of the topic—raises questions about whether the magnitude of this effect would be even larger among legislators/staffers who did not have prior knowledge about ACEs.
An additional limitation relates to parental blame being measured by a single item. Although consistent with prior measures of parental blame (Barry et al., 2013; Gollust et al., 2022; Wolfson et al., 2015), study results would be strengthened if replicated using a multiitem parental blame measure.
Conclusions
State-tailored, opposed to national, policy briefs about the behavioral health consequences of ACEs could produce parental blame for the consequences of ACEs among U.S. state legislators/staffers. This effect may be particularly pronounced among Democrats. Dissemination researchers and practitioners should be cognizant of the fact that packaging certain evidence in specific ways can have unintended consequences among some segments of a target audience. The unintended effects of disseminating research evidence warrant greater attention in the field of implementation science.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Robert Wood Johnson Foundation (grant no 76069).