
Abstract
Purpose
The objective of this study was to determine how to optimize implementation of tobacco cessation treatment interventions in cancer care by (1) investigating the feasibility and acceptability of a multi-level approach to tobacco cessation treatment intervention, (2) identifying barriers and facilitators to implementation, and (3) eliciting additional strategies to improve implementation of the intervention.
Methods
We conducted qualitative interviews with oncologists (n = 15) from one large academic health center in the Southeastern United States. We asked about their knowledge, attitudes, and current practices regarding tobacco use screening and treatment. We also asked about two proposed strategies to support implementation of tobacco cessation treatment: (1) developing a registry of tobacco users in collaboration with the state-run tobacco cessation program, and (2) providing on-site tobacco cessation counseling from trained professionals.
Results
Oncologists saw addressing tobacco use as valuable; however, they felt restricted from consistently addressing tobacco use by multi-level barriers such as workload, electronic health record (EHR) design, patient anxiety, and low self-efficacy for treating tobacco dependence. Oncologists responded positively to on-site treatment and felt this strategy would increase treatment accessibility and enhance engagement. Reaction to developing a registry of tobacco users was mixed, with concerns regarding lack of oncologist involvement and patient privacy expressed. Other suggested strategies for supporting implementation of tobacco cessation treatment included reducing referral complexity, establishing financial or quality incentives for oncologists, and leveraging existing EHR tools to facilitate integration of cessation interventions into clinic workflows.
Conclusions
We identified several challenges to implementing tobacco use treatment in cancer care; however, we considered strategies to overcome these barriers that were viewed as feasible and acceptable. Our work highlights the importance of engaging stakeholders in implementation efforts. Future work should explore the impact of the implementation strategies identified in this study.
Plain Language Summary
Tobacco cessation significantly improves cancer patients’ treatment outcomes, quality of life, and chances of survival; however, tobacco cessation interventions are not routinely delivered in oncology care. Interviews with oncologists identified barriers to delivering tobacco cessation interventions at multiple levels. Suggested strategies for overcoming these barriers included simplifying cessation intervention processes, establishing incentives for oncologists to address tobacco use, and using the electronic health record to support intervention activities. Oncologists generally supported implementing on-site tobacco cessation counseling for cancer patients. Although there was support for developing a registry of tobacco users with an external tobacco cessation program, more reservations were expressed. Our work identifies several stakeholder-endorsed strategies for implementing tobacco cessation interventions in cancer care. Future research should test the effectiveness of these strategies.
Background
About 12% of the 15 million cancer survivors in the United States are smokers (Gallaway et al., 2019; Salloum et al., 2019). Smoking after a cancer diagnosis results in reduced treatment effectiveness, increased risk of cancer recurrence and secondary cancers, increased treatment toxicity, and reduced quality of life (Do et al., 2004; Duffy et al., 2008; Gajdos et al., 2012; Johnson et al., 1997; Kenfield et al., 2011; Mason et al., 2009; U.S. Department of Health and Human Services, 2014, 2020; Warren, Kasza, et al., 2013). Smoking cessation is associated with improved survival among cancer patients (Gritz et al., 2014; U.S. Department of Health and Human Services, 2014, 2020); however, most quit attempts are made without evidence-based treatment, greatly reducing the chances of success (Fiore et al., 2008). Therefore, supporting smoking cessation has been referred to as the “fourth pillar” of cancer care, along with chemotherapy, radiotherapy, and surgery (Fiore et al., 2019). Accordingly, the National Comprehensive Cancer Network (NCCN) guidelines recommend the delivery of evidence-based smoking cessation counseling and pharmacotherapy to all cancer patients who smoke (National Comprehensive Cancer Network, 2019).
Despite the availability of effective smoking cessation treatment (Fiore et al., 2008), delivery of these evidence-based interventions in cancer care remains suboptimal (Price et al., 2019; Warren et al., 2013a, 2013b). Previously identified barriers to the delivery of tobacco cessation treatment in cancer care include lack of clinician time, competing demands and priorities, and inadequate procedures to triage smokers to smoking cessation treatment (D'Angelo et al., 2019; Warren et al., 2015; Warren et al., 2013a, 2013b). In order to overcome these barriers, tailored implementation strategies are needed to effectively integrate smoking cessation treatment into routine cancer care.
Qualitative approaches are especially useful for exploring the context in which an intervention will be implemented by identifying potential barriers and facilitators to implementation and assessing key drivers of implementation success such as acceptability, appropriateness, and feasibility (Hamilton & Finley, 2019; Proctor et al., 2011). Further, qualitative methods are critical to eliciting stakeholder perspectives and informing implementation strategies (Hamilton & Finley, 2019; Palinkas, 2014). To date, few published studies have applied qualitative methods to explore implementation of tobacco cessation treatment in cancer care (Rodgers-Melnick & Webb Hooper, 2021). We sought to fill this evidence gap by interviewing oncology providers to elicit their perspectives on implementation of tobacco cessation treatment in oncology settings.
The objective of this study was to determine how to optimize implementation of tobacco cessation treatment interventions in cancer care by (1) investigating the feasibility and acceptability of a multi-level approach to tobacco cessation treatment intervention, (2) identifying barriers and facilitators to implementation, and (3) eliciting strategies to improve implementation of the intervention.
Methods
Setting and Participants
This qualitative study was conducted alongside a clinical trial investigating the feasibility of implementing multi-level strategies to improve delivery of tobacco cessation treatment to cancer patients, described in detail elsewhere (LeLaurin et al., 2020). The study was conducted at a cancer center in a large academic health system in North Florida. The cancer center serves a population that is 37% rural and includes counties with some of the highest smoking rates in the state (UF Health Cancer Center, 2019). All practicing oncologists in radiation oncology, medical oncology, surgical oncology, and otolaryngology clinics were eligible for the study if they currently treated cancer patients. Oncologists were identified through the cancer center directory and invited to participate via email. All oncologists provided informed consent prior to participating in the interviews. This study was approved by the local Institutional Review Board.
Intervention—Tobacco Treatment Guidelines
Clinical practice guidelines issued by the NCCN state tobacco cessation should be an integral component of oncology treatment and continue throughout the cancer care continuum (Shields, 2015; Shields et al., 2016). Best practices for assessing and treating tobacco use in clinical care consist of screening all patients for tobacco use, documenting tobacco use status, advising and counseling patients on quitting, and providing tobacco cessation treatment or referral to cessation services (Fiore et al., 2008; Shields et al., 2016). In our study setting, healthcare providers can send referrals to the state’s tobacco cessation program, which offers free counseling and nicotine replacement therapy (Fiore et al., 2008). The healthcare system had introduced electronic health record (EHR)-based referrals to the state tobacco program in February 2018, the year prior to the study initiation.
In this study, we proposed multi-level approaches to support implementation of best practices in tobacco cessation treatment through two strategies. The first strategy was to develop a registry of tobacco users with cancer to share with the state tobacco cessation program, that would then perform direct outreach to patients. The second proposed strategy was to offer on-site counseling by tobacco treatment specialists from the state tobacco cessation program.
Data Collection
Data were collected from April to July 2019. A semi-structured interview guide was developed by the team and included questions and prompts about knowledge, attitudes, and current practices regarding tobacco use screening and referral and tobacco cessation treatment. The oncologists were also asked for feedback on the two proposed strategies to facilitate tobacco treatment in cancer care. This permitted an understanding of contextual factors, barriers, and facilitators to implementation that were specific to the study clinics. Two faculty and one graduate student on the research team (RGS, RPT, JHL) trained in qualitative methods conducted the interviews at the oncologists’ offices. One team member served as the primary interviewer while the other team member took field notes. Interviews lasted approximately 20 min and the participants received $20 gift cards for their participation. Interviews were audio recorded and transcribed verbatim.
Data Coding and Analysis
Coding and management of qualitative interview data were conducted using NVivo 12 (QSR International) concurrent with data collection. Two study team members (RPT, JHL) coded interview transcripts following a team-based approach to coding and codebook development and flexible, abductive coding methods (Deterding & Waters, 2021; MacQueen et al., 1998). We used an initial coding framework with categories related to the intervention component (screening, documentation, counseling, referral, treatment), intervention level (patient, provider, clinic), barriers and facilitators, and recommendations. Inductive coding was performed by both coders to account for emerging themes within these categories. We followed an iterative process of independent coding, comparison, and reconciliation. Both analysis team members independently coded the first five transcripts. For each coded transcript, inter-coder reliability was assessed using Cohen’s kappa at both the code- and transcript-level. Codes with both a low kappa statistic (< 0.40) and a high level of disagreement between coders (> 20%) were flagged for detailed review. Each independently coded transcript was discussed in a team meeting during which coding discrepancies were reconciled, changes to code structure and definitions were established, and new codes identified. A third team member with subject-matter expertise (RGS) provided input for resolving coding discrepancies. Following each coding meeting, the codebook was updated and previously coded transcripts were back-coded to account for changes made. The remaining 10 transcripts were fully coded by one of the team members, whose coding was then reviewed by the other team member. A table was developed to establish an audit trail of code changes and assess thematic saturation, which was reached after the 10th transcript.
After coding was complete, codes were mapped to corresponding constructs from the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2009). The CFIR is a comprehensive framework which describes constructs influencing implementation success. CFIR domains and constructs used are presented in Table 1. Member and expert checking were conducted at the conclusion of analysis.
CFIR domains and constructs used (Damschroder et al., 2009).

Results
We invited 27 oncologists to participate, of which 15 completed interviews, 11 did not respond, and one declined. Oncologists specialized in medical oncology (n = 6, 40.0%), radiation oncology (n = 4, 26.7%), otolaryngology, head and neck surgery (n = 3, 20.0%), and surgical oncology (n = 2, 13.3%). Nine (60.0%) oncologists were male and six (40.0%) were female.
Barriers and Facilitators to Tobacco Cessation Treatment
Table 2 presents themes relevant to barriers and facilitators to tobacco cessation treatment, organized by CFIR domains and constructs. Quotations provided for each theme include information on the intervention component being addressed and the participant’s specialty.
Barriers and facilitators to implementation of tobacco cessation interventions by CFIR constructs.

Inner Setting
The complexity of the EHR served as both a barrier and facilitator to addressing tobacco use depending on the intervention component. The EHR was a strong facilitator to screening and documentation due to availability of tools such as visit templates, prompts, and smart phrases, which allowed for easy navigation to relevant EHR modules. Participants also noted that smoking status was easy to retrieve from the EHR. Conversely, the EHR was the most discussed barrier to electronic referral. Some oncologists had trouble finding the referral order in the EHR, and four remarked that the referral order required too much information, such as the best time to call and the patient’s treatment preferences. This problem was compounded by the fact that referrals were often entered when the patient was not in the room to provide this information.
Workload was one of the few reported barriers to screening. Oncologists described how the growing patient volume combined with increasing requirements for practice and documentation, such as regulations related to prescribing narcotics, exerted pressure on oncologists and staff. Although oncologists felt that addressing tobacco use was important, it was described as “just one of a million things” they needed to complete in a visit.
In relation to the relative priority construct, screening was prioritized for new patient visits. One oncologist noted research studies requiring smoking status data also facilitated documentation to tobacco use. Oncologists explained that tobacco use screening was prioritized due to its clinical impact as well as reimbursement requirements. Most oncologists stated screening at return visits was less of a priority, though one oncologist who primarily treated lung and head and neck cancer patients stated they screened at every visit out of habit.
The compatibility of tobacco use screening with the clinic workflows also differed between new and return patient visits. Standardized workflows typically supported screening for new patient visits, but not returning patients. Oncologists described multiple screening opportunities during new patient visit workflows; however, screening at return visits was not part of routine workflows and usually not included in EHR note templates.
Outer Setting
External policies and incentives were a strong facilitator for screening and counseling due to documentation requirements for new patient visit reimbursement. Several factors related to patient needs and resources were also identified. Over half of oncologists noted distress and anxiety related to a cancer diagnosis makes patients unreceptive to counseling on tobacco cessation, and some patients do not have any interest in quitting. Oncologists recognized that the most important time for patients to quit was at diagnosis, but that patients were often not receptive to addressing tobacco use until later in the course of their treatment. Many oncologists also noted they were more likely to discuss tobacco use and other behavioral changes after treatment was complete because they had fewer competing demands and patients were more open to discussing cessation.
Characteristics of Individuals
Oncologists frequently expressed a lack of awareness related to tobacco cessation resources both within and outside the health system. All oncologists in this study were asked if they were aware of the EHR referral to the state tobacco program, with only about half replying they were familiar with the tool. Another oncologist was aware of the referral order but unsure how to use it. Many oncologists were also unfamiliar with the tobacco cessation resources available to patients in the healthcare system, although one oncologist who was familiar with the EHR referral was uninterested in knowing details, stating, “As long as it gets done, I don’t care who does it.”
Some oncologists expressed frustration or difficulty with the EHR in general, which extended to the EHR-based components of tobacco cessation treatment. Their frustration stemmed from factors such as frequent changes and updates, number of clicks required, and hard stops, which force the provider to enter data before moving to the next screen. Although oncologists acknowledged the value of the EHR, it was often described as overwhelming and difficult to navigate.
In terms of self-efficacy, some oncologists noted that while they were confident in their ability to routinely screen for tobacco use and advise patients to quit, they were less confident in their ability to provide counseling and discuss treatment options. Although tobacco use was seen as relevant to patient treatment and outcomes, engaging patients in treatment was seen by many oncologists as beyond their scope of expertise, with one noting it was an issue that would be better addressed by primary care physicians.
At return patient visits, prioritization of addressing tobacco use was described as dependent on the patient’s condition and stage of treatment. Most oncologists noted their decision to address tobacco use was often dependent on whether they felt tobacco use was relevant to the patient’s diagnosis (e.g., tobacco-related cancers), impacting the patient’s treatment, or detrimental to their quality of life. This was especially salient for surgeons, who were invested in encouraging patients to quit prior to surgery due to the negative impact of tobacco use on surgical outcomes; however, once surgery was complete, cessation was no longer a priority.
Feedback on Proposed Strategies
We solicited feedback on two proposed strategies to increase uptake of tobacco cessation treatment in cancer care: building a registry of tobacco users in collaboration with the state-run tobacco cessation program and co-located treatment. Whereas response to building a registry was mixed, co-located treatment was widely viewed as an acceptable and effective strategy to address tobacco use in cancer care.
Tobacco User Registry
Reactions to the registry strategy were mixed. While oncologists acknowledged this approach would increase the reach of the intervention, they felt that effectiveness of the treatment would be decreased without oncologist involvement. One surgical oncologist stated, “…if the conversation isn’t started with the physician who’s providing the chemotherapy, it’s probably not going to be as effective as you’d think.” Another frequent concern was the issue of patient privacy. About half of oncologists expressed concerns about sharing health information or felt patients would react negatively to unsolicited contact about tobacco cessation. One noted this strategy could damage the patient-provider relationship. Proposed strategies to mitigate privacy concerns were to offer patients the opportunity to opt-in during visit check-in and to notify patients they would be contacted regarding tobacco cessation. Finally, capacity of the state-run program to handle referrals was a concern, although one suggested that resources could be conserved by using text or automated messaging.
On-site Treatment
Oncologists expressed positive responses to offering on-site treatment to patients who use tobacco. They felt that this model would increase the accessibility of tobacco treatment and enhance engagement. Several suggested that treatment should be available on demand, with one radiation oncologist explaining, “You know, something where it’s right there in the moment, because oftentimes it’s sort of an emotional discussion of getting them ready to do it and boy, if you call them back even a day later they go, ‘Oh, I’ll think about doing it next month.’ You’ve got to really strike while the iron is hot.”
Concerns with co-located treatment generally centered on space limitations and logistical challenges. When asked about the format of counseling treatment, most oncologists noted individual counseling was more feasible than group counseling. Other suggestions included tailoring treatment by offering brief counseling sessions, performing intensive follow up, and offering prescription medications. One oncologist noted that for billing purposes, tobacco treatment should be delivered in a separate visit to generate additional reimbursement.
Clinician Proposed Strategies
In addition to comments on the proposed strategies, oncologists offered suggestions on other ways to improve tobacco cessation treatment in cancer care. Recommended strategies organized by the CFIR are presented in Table 3.
Recommended strategies organized by the CFIR.
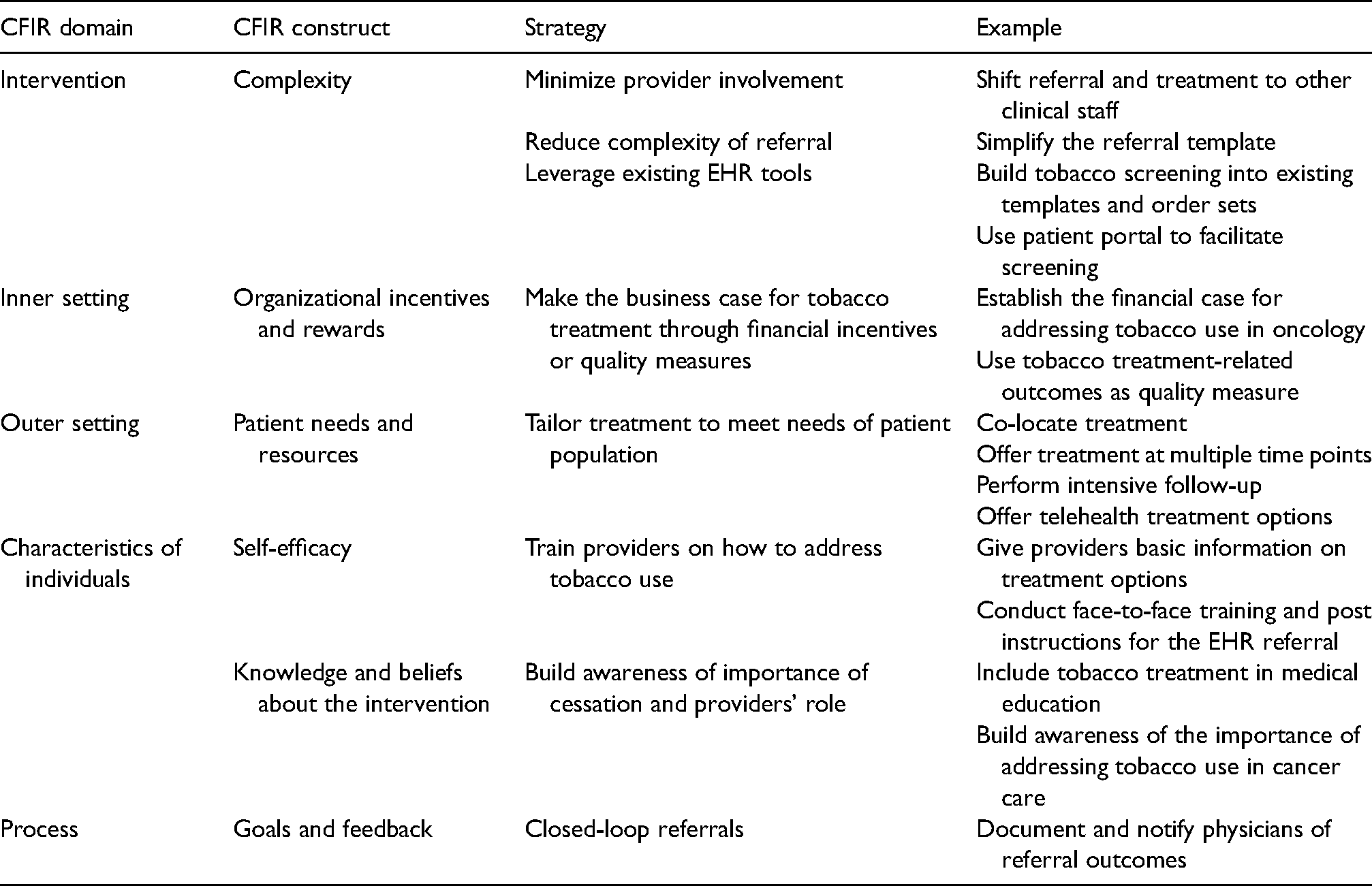
Intervention Characteristics
Many suggestions related to methods of reducing the complexity of the tobacco treatment intervention referral process. Recommendations included leveraging existing EHR tools (e.g., order sets, patient portal) and simplifying the existing referral template. While oncologists generally felt that it was their role to encourage patients to stop using tobacco, they felt facilitating treatment could be handled by another member of the clinical team. One medical oncologist stressed the importance of minimizing oncologist involvement in the referral process, stating, “I think you’re fooling yourself if you think, ‘Well, it’s just one click, it’s just one piece of paper to fill out. Just sign this piece of paper and it’ll be done for you.’ It won’t happen. It has to happen outside of the input from the physician.”
A recurring suggestion related to this issue was to allow more members of the clinical team to issue the referral order, rather than requiring oncologists to sign off.
Outer Setting
Physicians emphasized the need to present a financial case to the healthcare system for integrating tobacco treatment into cancer care. One oncologist suggested that addressing tobacco use could be used as a quality measure if the financial case could not be established. Another suggestion was to tailor treatment options to the patient population. Oncologists discussed how the optimal time for patients to quit is prior to treatment, but patient distress and care complexity at this stage were barriers to addressing tobacco use. In light of this tension, they indicated that tobacco treatment should be offered consistently at multiple timepoints. Given the large proportion of rural patients who travel significant distances to receive care at the healthcare system, telehealth options were also encouraged.
Characteristics of Individuals
To overcome barriers related to oncologists’ self-efficacy, brief trainings for providers with information on the electronic referral to tobacco cessation treatment options were recommended. To build awareness of the oncologist role in tobacco cessation, it was suggested that the topic should be emphasized in medical education.
Process
A frustration with referral to the state-run program was that oncologists sent the order “into the void” and did not receive information on the outcome of the referral. One radiation oncologist stated that receiving referral outcomes would “reinforce [her] good behavior.” Another oncologist emphasized the importance of receiving referral outcomes to enable assessment of clinic performance on tobacco-related measures.
Discussion
We elicited oncologist perspectives on factors affecting delivery of evidence-based tobacco cessation treatment and strategies to integrate this treatment into routine cancer care. We found that oncologists see addressing tobacco use in their patients as valuable, but barriers at multiple levels prevent them from consistently doing so. Oncologists also expressed support for specific implementation strategies to enhance the delivery of tobacco cessation treatment. Although previous qualitative research has explored tobacco cessation treatment in cancer care (Khodadadi et al., 2021; Rodgers-Melnick & Webb Hooper, 2021; Wells et al., 2017), our study is unique because of its explicit focus on implementation strategies and use of an established implementation science framework.
In an effort to support the implementation of tobacco cessation treatment in cancer care, the National Cancer Institute launched the Cancer Center Cessation Initiative (C3I) in 2017 (Croyle et al., 2019). Participating NCI-designated cancer centers receive funding to implement or expand tobacco cessation treatment programs. Although our study was not conducted at a C3I site, our findings are similar to those of studies conducted in C3I cancer centers. For example, a qualitative study with oncologists at a C3I site also found themes of tobacco cessation treatment prioritization being dependent on patients’ clinical status, low clinician self-efficacy in delivering tobacco cessation treatment compared to screening, and barriers related to the EHR, patient stress, and lack of time (Rodgers-Melnick & Webb Hooper, 2021). A quality improvement project at another site reported limited time and reliance on clinicians for referrals as barriers (Gali et al., 2020). Our finding that oncologists are often unaware of available cessation resources is also consistent with previous studies (Gali et al., 2020; Rodgers-Melnick & Webb Hooper, 2021; Warren et al., 2013a). Notably, our targeted exploration of implementation determinants uncovered factors such as workflow compatibility and intervention complexity which have not been emphasized in previous work.
The EHR was often cited as a facilitator for tobacco use screening, but lack of awareness of the EHR referral and general frustration with the EHR emerged as significant barriers to connecting patients with treatment. Integrating tobacco cessation treatment referrals into EHR systems improves referral rates (Boyle et al., 2014; Fiore et al., 2019), but oncologists and clinic staff must be aware of referral options and willing to use them. In this study, oncologists familiar with the referral expressed frustration with the amount of information required for completing the referral. Modifications to the referral order could easily address this issue, but any changes to the EHR require an involved and lengthy process. For example, after 8 months of funding, less than one quarter of C3I sites had completed necessary EHR modifications to identify and refer tobacco users (D'Angelo et al., 2019). One helpful resource to facilitate EHR modifications for addressing tobacco use in cancer care is a C3I-developed EHR guide for building EHR tobacco cessation treatment functionalities (Cancer Center Cessaton Initatve (C3I) Coordinatng Center, 2019). Such resources and targeted implementation strategies can help promote the uptake and sustainability of EHR-based tobacco cessation treatment interventions (Cancer Center Cessation Initiative Sustainability Working Group, 2021).
The optimal time for cancer patients to quit tobacco is at diagnosis, but oncologists in our study discussed how cessation interventions are more feasible later in the cancer care continuum due to fewer competing clinical demands and greater patient receptivity. Some oncologists emphasized the importance of offering tobacco cessation treatment at multiple timepoints, in line with clinical practice guidelines (National Comprehensive Cancer Network, 2019). Nonetheless, tobacco cessation interventions show greater success rates when administered shortly after diagnosis (Cox et al., 2002; Garces et al., 2004; Schnoll et al., 2003), so it is important to identify strategies for addressing tobacco use in the early stages of cancer treatment that are sensitive to demands on providers and patient stress.
We presented two potential models for integrating tobacco cessation treatment into cancer care, building a registry of tobacco users to share with the state-run tobacco program and co-located treatment. Oncologists responded positively to co-located treatment, but opinions on the registry were mixed. One concern related to the registry was that while this approach may result in greater reach, tobacco cessation treatment engagement and effectiveness could be diminished without oncologist involvement. On the other hand, oncologists noted that co-located treatment would present logistical challenges and require additional resources. It remains unclear which tobacco cessation treatment model, or combination of models, is most effective (Salloum et al., 2021). More research is needed to determine the optimal design of tobacco cessation treatment programs and implementation strategies in cancer care in relation to effectiveness and sustainability while recognizing that this will likely be dependent on healthcare system context.
Strengths of this study include elicitation of stakeholder input from a range of oncology providers on specific implementation strategies and use of the CFIR. We conducted our research in the context of a clinical trial at a single academic healthcare system. Therefore, our findings may be reflective of institutional practice patterns and may not be fully transferrable to other oncology settings, which need to account for different stakeholder preferences and implementation barriers. Another limitation of this research is that we only interviewed oncologists, while input from other stakeholders (e.g., clinic staff, patients, healthcare system leadership) is critical for successful implementation of tobacco cessation treatment in cancer care. Finally, the CFIR was used to guide the development of the intervention in preliminary work for this study (not presented here), and also to guide our final analysis of interview findings. However, our interview guide did not incorporate CFIR constructs and was based only on questions of workflow and feasibility of new strategies specific to the study clinics. The inconsistency in our use of CFIR across these study phases may have led to missed opportunities to link our preliminary and main study efforts in meaningful ways.
Conclusions
This study identified factors affecting the implementation of tobacco cessation treatment in cancer care along with stakeholder perspectives on implementation strategies to address tobacco use in cancer patients. Our work highlights the importance of engaging stakeholders in implementation efforts. Our findings can inform the development of tailored implementation strategies to support the integration of tobacco cessation treatment into routine cancer care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Florida Health Cancer Center.