
Abstract
Plain Language Summary
Latino men who have sex with men (LMSM) are diagnosed with HIV and experience mental health and substance use problems more than their non-Latino/non-MSM peers. This means there is a disparity: one group is burdened by a disease more than another group. There are interventions, like pre-exposure prophylaxis and mental health/substance use treatment that can address this disparity. But, LMSM do not have enough access to these. This means there is a healthcare disparity: one group does not have as much access to healthcare as another group. The purpose of this study was to create a program to help LMSM get these services and consider how to implement it. LMSM and potential implementers talked about factors to consider in developing this program and implementation. They said the program and implementation need to (1) consider the cultural context in which LMSM are embedded, (2) leverage LMSM and implementers’ networks, (3) increase LMSM and implementers’ ability to navigate complex health systems, (4) be tailored to the resources available to consumers and implementers, and (5) build consumer and implementer motivation. These factors are important to address when developing and implementing programs to help LMSM get HIV-prevention and behavioral health treatments.
Keywords
Latino men who have sex with men (LMSM) 1 face substantial HIV disparities. For example, LMSM experienced 22% of all new HIV diagnoses in 2019 (Centers for Disease Control and Prevention, 2020). Yet, evidence-based interventions, such as pre-exposure prophylaxis (PrEP), have not been sufficiently scaled up and out to LMSM (Blashill et al., 2020; Harkness et al., 2021b; Kimball et al., 2020). PrEP use in the past year was reported by only 28% of US-born LMSM (Trujillo, 2019). This gap in the successful implementation and dissemination of PrEP perpetuates HIV disparities (Pinto et al., 2018) and inhibits progress toward the Ending the HIV Epidemic (EHE) plan (Fauci et al., 2019).
LMSM are also impacted by behavioral health (i.e., mental health and substance use) disparities, which worsen HIV disparities. The synergistic nature of HIV and behavioral health disparities is a “syndemic,” whereby both epidemics, situated in social inequities, synergistically worsen one another (Singer et al., 2006, 2017). In addition to behavioral health disparities, one type of syndemic driver, LMSM simultaneously navigate the impacts of racism and homophobia, which add to and amplify the multiplicative effects of HIV and behavioral health disparities (Mizuno et al., 2012). The additive impact of syndemic drivers, including but not limited to behavioral health problems, is associated with sexual behavior that can lead to HIV acquisition (Martinez et al., 2016; Mizuno et al., 2012). Yet, as with PrEP, evidence-based behavioral health treatments are insufficiently scaled up and out to LMSM. Among LMSM diagnosed with a mental health disorder, less than half received treatment (Burns et al., 2015), underscoring the need to link LMSM to treatment.
Prior research has identified barriers to LMSM’s PrEP, HIV testing, and behavioral health treatment uptake. Psychosocial (e.g., depression, substance use, childhood sexual abuse, intimate partner violence) and structural (e.g., incarceration, unstable housing, poverty) syndemic drivers are associated with lower PrEP use among LMSM (Blashill et al., 2020). PrEP, HIV, and mental health stigma are pervasive barriers that impede PrEP use, HIV testing, and behavioral health treatment among LMSM (Hatzenbuehler, 2009; Lelutiu-Weinberger & Golub, 2016; Solorio et al., 2013). Low perceived need or relevance of services can also impede PrEP, HIV testing, and behavioral health treatment among LMSM (Breslau et al., 2017; Cook et al., 2014; Harkness et al., 2021a).
Additionally, our formative research (the DÍMELO study) with LMSM and stakeholders (individuals who delivered HIV-prevention and behavioral health treatments to LMSM in South Florida) identified barriers and facilitators that need to be addressed to increase the reach of these services to LMSM. The qualitative aim of DÍMELO included LMSM (∼50% born outside the United States) and stakeholders and identified implementation determinants (Harkness et al., 2021a) using the Consolidated Framework for Implementation Research (Damschroder et al., 2009). Key determinants of HIV-prevention and behavioral health treatment use among LMSM included complexity of service access, perceived benefits of services, policies influencing service availability, patient needs and resources that could affect service use (e.g., transportation, education, immigration status, mental health/substance use), peer influence (e.g., peer stigma vs. normalization), LMSM and provider knowledge, provider/organizational relationships (e.g., stigma vs. affirmation, trust, personalism), and the availability of services. The quantitative aim of DÍMELO surveyed 290 LMSM in South Florida (∼50% born outside the United States) and identified additional determinants of LMSM’s demand for PrEP and behavioral health treatments (Harkness et al., Manuscript Under Review). For PrEP, key facilitators included knowledge, self-efficacy, community norms, and navigation support, whereas low perceived need was a barrier. For behavioral health treatment, key facilitators included a medical provider or personal contact recommending treatment, perceived need, and community norms, knowledge, and attributing mental health concerns to one’s environment or culture. In contrast, those who relied on family/friend support were less likely to engage in behavioral health treatment.
To address the ongoing, synergistic HIV and behavioral health disparities affecting LMSM, multilevel implementation strategies are needed that will: (1) increase LMSM demand for PrEP and behavioral health treatments and (2) equip implementers to deliver consumer-facing implementation strategies to increase LMSM demand for PrEP and behavioral health treatments. Here, we define implementation strategies as “methods or techniques used to enhance the adoption, implementation, and sustainability of a clinical program or practice,” (Proctor et al., 2013, p. 2) with PrEP and behavioral health treatments being the clinical interventions. The current study’s goal is to engage in formative research to refine the consumer-facing and implementer-facing components of one potential implementation strategy to improve the reach of HIV-prevention and behavioral health treatments to LMSM, which we call “Dime Más” (“Tell me More”). Further, we seek to develop the implementation strategy with substantive community input, with community defined as both potential consumers of Dime Más, HIV-prevention services, and behavioral health treatments, as well as potential implementers of Dime Más. This is consistent with Pinto and colleagues’ (2021) guidance, who articulate the need for community engagement to be integrated more fully into existing dissemination and implementation models and efforts.
Based on our findings from the DÍMELO study (Harkness et al., Manuscript Under Review, 2021), we developed an initial framework for this implementation strategy, including a consumer-facing and provider-facing component (see Figure 1). We entitled the consumer-facing component, which aims to increase consumer demand, Dime Más. As shown in Figure 1, based on our findings from DÍMELO, we developed a preliminary version of Dime Más. The preliminary version is one session (approximately 60 min with three brief monthly boosters to balance ongoing engagement with feasibility) in which an LMSM outreach worker would utilize motivational interviewing, problem-solving, healthcare needs assessment and tailored referrals, and peer ambassador stories to increase LMSM consumers’ PrEP, HIV testing, and behavioral health treatment uptake. The implementation strategy was anticipated to take place in community health clinics (i.e., locations where outreach workers are already employed). Of note, although Dime Más unifies evidence-based behavior change techniques such as motivational interviewing (Naar-King et al., 2012; Outlaw et al., 2010), problem-solving (Gardner et al., 2014), peer education and linkage (Shangani et al., 2017), and self-affirmation (Walton & Cohen, 2011), Dime Más has not yet been tested on its own. The preliminary components of Dime Más were developed based on findings from the DÍMELO study; the current study seeks to refine Dime Más using LMSM and stakeholder feedback to enhance its impact and feasibility, while also identifying themes that could apply to other implementation strategies to achieve similar goals.

Implementation research logic model.aImplementation determinants were identified in the DÍMELO study (Harkness et al., 2021).bThe focus of the current project is to conduct formative research to refine the implementation strategy.cHypothesized mechanisms and outcomes will be assessed in a subsequent pilot trial.
With the development of the preliminary version of Dime Más, there was a simultaneous need to develop an implementer-level component of the implementation strategy to facilitate delivering Dime Más. A key issue when researchers develop health promotion programs to increase consumers’ uptake of a clinical intervention is that implementation is not considered in the planning phase (Wisdom et al., 2014). This is evidenced by the traditional translational pathway, in which programs are developed, tested in controlled efficacy trials, followed by effectiveness trials, and finally, implementation trials (Brown et al., 2017). There is often a “voltage drop” with each step of the translational pathway (Chambers et al., 2013). As such, our goal in developing Dime Más is to consider implementation from the outset by centering the voices of potential implementers and LMSM consumers. Therefore, the current study also examined stakeholders’ (defined in this study as individuals who work with LMSM in HIV-prevention or behavioral health services in the Miami area) perspectives regarding potential implementation barriers and facilitators for Dime Más in their setting and sought feedback on strategies to implement Dime Más in their settings. As such, the findings suggest strategies needed to implement Dime Más and programs like it in community settings.
Methods
Participants and procedures
Participants included 13 LMSM and 12 stakeholders across three focus groups and three individual interviews. Focus groups (N = 3) were held in English and Spanish for LMSM (n = 2) and in English for stakeholders (n = 1). Three stakeholders who were not available to participate in the focus group were interviewed individually. LMSM were recruited via social media advertisements, a consent-to-contact database, and word of mouth. Stakeholders were recruited through our community partner network.
Eligible LMSM (a) identified as Latino/Hispanic, (b) identified themselves as a man who has sex with men (including gay, bisexual, and other MSM), (c) were between 18 and 39 years, (d) spoke English/Spanish, (e) self-reported HIV-negative or unknown HIV status, and (f) resided in the Miami area. Eligible stakeholders (a) were 18 to 65 years old and (b) worked with LMSM in HIV-prevention or behavioral health in the Miami area. Inability to provide consent, risk of harm from the study, or having a medical or psychiatric condition that would interfere with participation (determined as needed by PI, a licensed psychologist) were exclusion criteria.
Recruitment took place from December 2020 to April 2021. Prospective participants completed a phone screen and were scheduled if eligible. Some who consented to participate did not end up participating (N = 11). Following our IRB-approved protocol, participants reviewed consent information (e.g., study procedures, risks/benefits, voluntariness) within REDCap and checked “Yes, I consent to participate,” before completing study procedures via REDCap (demographic survey) and videoconferencing (interviews). Following participation, focus group participants received $50 and individual interviewees received $25.
Data collection
Demographic surveys
Demographic surveys assessed race, ethnicity, gender identity, sexual orientation, and other key demographics. LMSM were asked about employment status, nativity, and citizenship. Stakeholders provided information about their organizational role.
Focus groups and interviews
Semi-structured focus group interview guides (see Supplemental File) were developed to assess the extent to which the initial version of Dime Más was acceptable, appropriate, and feasible to LMSM and stakeholders, and refinements to align Dime Más with the needs and priorities of LMSM and stakeholders. We adapted the focus group guide for individual interviews with stakeholders to ensure representation of stakeholders (e.g., across levels of organization and different organizations). Although the interview guides were not pilot tested, revisions were made based on feedback from research team members before administration. The first author wrote the first draft of the interview guide, which was iteratively revised across a series of consultations with coauthors with expertise in implementation science, health disparities, and HIV prevention. Feedback resulted in changes such as adding questions to probe the acceptability and appropriateness of specific innovative components of Dime Más (e.g., the peer ambassadors, the need for implementers to be LMSM) and streamlining the interview guide to reduce participant burden while still obtaining key information.
Interviewers first explained the purpose of the interview, which was to develop a program to increase PrEP, HIV testing, and behavioral health treatment uptake among LMSM in South Florida, and ensure this program addresses the needs and priorities of potential consumers and implementers. We presented the initial version of Dime Más, including its content, format, and design, and the basic framework of the training for Dime Más implementers. Participants were asked about the acceptability, appropriateness, and feasibility of Dime Más. Stakeholders were probed about implementing Dime Más, including implementation barriers and facilitators within their settings. Focus groups and interviews were conducted via videoconferencing and lasted approximately 90 min and 30–60 min, respectively. Although transcripts were not shared with participants, LMSM and stakeholders were given the option to provide additional comments after the interview via a web-link or email (none elected to do so). Only participants and interviewers were present for data collection.
Research team
Five research team members conducted the focus groups and individual interviews. Interviewers varied by gender/sexual orientation (cisgender heterosexual women and cisgender sexual minority men), race/ethnicity (Latina/o, White), and academic training/discipline (psychologist/faculty in public health, doctoral students in public health and psychology, and research assistants in psychology). We strived to “match” interviewers with participants. For example, LMSM focus groups were conducted by interviewers with shared identity concerning sexual orientation, gender, and/or ethnicity. Bilingual/bicultural interviewers carried out the Spanish-language focus group. Stakeholder interviews were conducted by team members who delivered HIV-prevention and behavioral health treatments. Although the degree to which qualitative interviewers reflect “insider” versus “outsider” status has been debated in the literature in terms of benefits and drawbacks (Hoong Sin, 2007; Wray & Bartholomew, 2010), we had a team of researchers with shared experiences and therefore elected to leverage the potential benefits of this in terms of building trust and engagement while also utilizing reflexive engagement to address the reality that all interviewers still brought their lived experiences which may have shaped their probing and interpretation of participant responses.
The first author developed the team based on their academic backgrounds and commitments to health equity among sexual minority and Latino/a/x 2 communities. Most team members conducted prior research and/or had preexisting relationships with local stakeholders, facilitating recruitment, and rapport. Some participants previously participated in the DÍMELO study (Harkness et al., Manuscript Under Review, 2021) and were aware of the team’s goals and research. Although all team members had prior experience conducting qualitative research on HIV and behavioral health among LMSM, the first author provided initial training on the interview guide and analytic approach. Analyses were carried out by the first author and two doctoral students (second and third authors) and verified by all team members. Team meetings provided opportunities to practice reflexivity (Morrow, 2005) surrounding the extent to which our identities and experiences influenced our interviewing and data analysis approach.
Qualitative analysis
All interviews were audio-recorded, transcribed, and analyzed. Two qualitative analytic approaches were used: the framework and the general inductive approaches. The framework approach, recommended for qualitative implementation research (National Cancer Institute, 2018), involves applying an existing framework to analyze qualitative data. In our case, the Health Equity Implementation Framework (HEIF; Woodward et al., 2019, 2021) served as the framework. This framework articulates domains that impact the implementation of an innovation, including (a) the innovation itself, (b) the consumers of the innovation, (c) the implementers of the innovation, (d) the clinical interaction between implementers and consumers, (e) the inner context in which the innovation is delivered, and (f) the outer context in which consumers, implementers, and inner contexts are situated.
We combined the framework approach with the general inductive approach (Thomas, 2006). Using this approach allowed us to identify emergent themes from the qualitative data that were mapped onto the HEIF domains. Two analysts repeatedly reviewed the transcripts and independently identified lists of codes and their corresponding HEIF domains. The lead author then reviewed transcripts and analyst notes to develop the codebook. The codebook formed a matrix, with codes (later consolidated into higher order themes) identified on the vertical axis and the HEIF domains on the horizontal axis. Each code could intersect with any HEIF domains (Table 1). The analysts then independently applied the codebook to the transcripts. The lead author reviewed for consensus and documented in NVivo 12. Where there was disagreement between analysts, the team discussed to consensus and added/revised codes. Throughout the data collection process, we were coding the data and tracking thematic saturation. Evidencing saturation, no new codes were added for the final three transcripts (Guest et al., 2016). In other words, as we were collecting and coding data from the first three transcripts, new codes emerged, whereas we stopped identifying new codes in the final three, which informed us that we had reached saturation and could discontinue enrolling new participants. Upon coding completion, the team identified five major content themes within which the codes were consolidated. Of note, we utilized several recommended methods for enhancing the trustworthiness of our qualitative findings, including using multiple coders for all transcripts, including a multidisciplinary team with a range of lived experiences/identities, implementing a reflexive consensus-building process with a third analyst at each coding meeting, using coding disagreements and unique perspectives to enrich the analysis, and transparently reporting our analytic approach (Armstrong et al., 1997; Hemmler et al., 2020; Mays & Pope, 2000; Morrow, 2005; Saldana, 2015; Sweeney et al., 2013).
Codebook matrix.
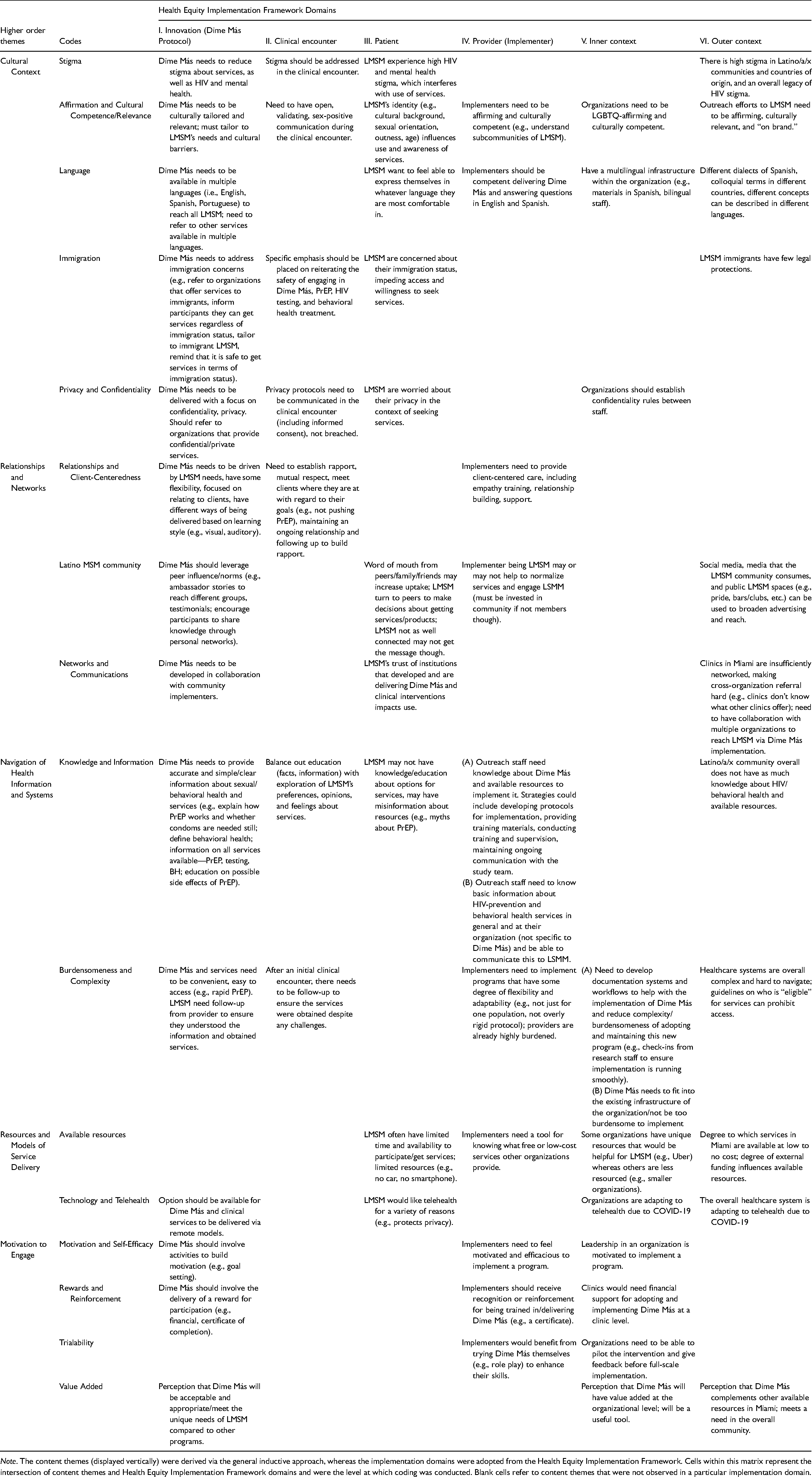
Note. The content themes (displayed vertically) were derived via the general inductive approach, whereas the implementation domains were adopted from the Health Equity Implementation Framework. Cells within this matrix represent the intersection of content themes and Health Equity Implementation Framework domains and were the level at which coding was conducted. Blank cells refer to content themes that were not observed in a particular implementation domain.
Results
Participant demographics
LMSM ranged in age from 22 to 37. Most identified as gay (92%) and White Latino (92.3%). The majority were born outside the United States (i.e., Chile, Colombia, Dominican Republic, Mexico, Nicaragua, Venezuela), and about half were US citizens.
Stakeholders ranged in age from 18 to 62, and most identified as Latino/a. Stakeholders included outreach workers, PrEP navigators, HIV test counselors, administrative assistants, managers, directors, and supervisors. Complete demographics are in Table 2.
Participant characteristics.
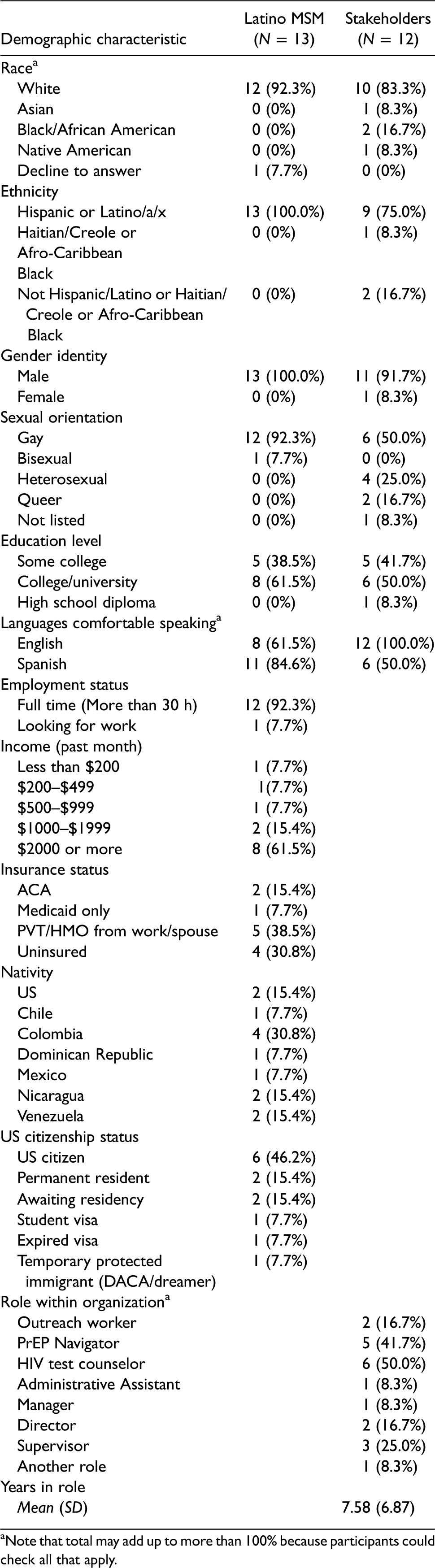
Note that total may add up to more than 100% because participants could check all that apply.
Qualitative findings
Here, we present our findings organized by higher order themes in which the relevant codes (in italics) and HEIF domains are described. Table 1 summarizes the codebook, and Table 3 provides quotations (numbered quotations can be matched to Table 3).
Example quotations illustrating content themes across implementation domains.

Implementation domain that the quote refers to (Implementation domains: I = Innovation, II = Clinical Encounter, III = Patient, IV = Provider, V = Inner Context, VI = Outer Context).
Cultural context
Due to the HIV, mental health, and sexual orientation/behavior stigma that LMSM experience within their communities, they suggested that Dime Más have a component to reduce HIV and mental health stigma (Q1). They described the importance of the clinical encounter, in which Dime Más is delivered, to be nonstigmatizing (e.g., Dime Más implementer using nonstigmatizing language to talk about mental health). Given that LMSM’s intersecting identities could influence the use of services, participants felt Dime Más needed to be affirming and culturally competent/relevant, accomplished by culturally tailoring to LMSM (Q2). Participants viewed the name “Dime Más” favorably, based on their impression that it was relatable and affirming for LMSM across identities. They also described the need for Dime Más implementers, implementing organizations, and outreach efforts to be affirming and culturally competent (Q3).
Language and immigration were additional cultural context factors that were important to consider in developing and implementing Dime Más. Participants underscored the need for Dime Más to be available in multiple languages (i.e., English and Spanish, but Portuguese and Haitian Creole could further extend reach), Dime Más implementers being bilingual, and having PrEP, HIV testing, and behavioral health referrals to Spanish-speaking providers (Q4, Q5). Due to LMSM’s immigration fears and lack of legal protections (Q6), participants explained the importance of Dime Más being tailored to address these immigration concerns by referring to providers who specifically serve immigrant communities, ensuring LMSM know they can legally access these services regardless of their immigration status, and making clear that Dime Más is inclusive of immigrants.
Because of the context in which LMSM seek services—including stigma and immigration fears—participants discussed the importance of privacy and confidentiality when participating in Dime Más and accessing services. They described the importance of Dime Más being presented to LMSM as confidential and referring to organizations that prioritize confidentiality (Q7). They also described the importance of organizations that implement Dime Más and other healthcare services establishing confidentiality rules, as some participants described experiences when their information was shared unnecessarily between staff, resulting in mistrust.
Relationships and networks
Participants explained that relationships and client-centeredness and leveraging relationships within the Latino MSM community were key to developing and implementing Dime Más. They explained that Dime Más needs to be client-centered and flexibly delivered, such that implementers honor LMSM’s own goals and focus on building and maintaining rapport (Q8). Relationships within the LMSM community and peer influence could also facilitate the development and implementation of Dime Más. Participants explained that word of mouth is a powerful influencer on the uptake of services among LMSM and that LMSM turn to their peers to make decisions about healthcare services to use or avoid. Given this, participants were enthusiastic about having “peer ambassadors” within Dime Más who could influence LMSM’s PrEP, HIV testing, and behavioral health treatment uptake (Q9). They underscored the importance of peer ambassadors being relatable and reflecting the diversity of LMSM (e.g., language, race, employment status, sexual orientation, gender expression, nativity, citizenship). Although participants generally agreed peer ambassadors would be important as a component of Dime Más, they were mixed on whether Dime Más implementers needed to identify as LMSM and also in some cases expressed concerns about the feasibility of always having an LMSM implementer. There was, however, consensus that if an implementer was not LMSM, they needed to be trained to communicate affirmation and respect (Q10).
Two additional considerations related to networks and communications arose related to the continued development and implementation of Dime Más. First, participants indicated Dime Más would be well received due to its affiliation with an academic institution and because it was developed in partnership with community organizations. Second, participants (mostly stakeholders) described the need to bridge networks between HIV and behavioral health organizations in Miami to implement Dime Más. Stakeholders explained that their organization might not have the resources to meet every LMSM’s needs, therefore if they implemented Dime Más, they wanted to be networked with other HIV and behavioral health organizations to deliver HIV and behavioral health treatments to LMSM (Q11).
Navigation of health information and systems
Due to a lack of access to knowledge and information, participants felt that HIV-prevention and behavioral health services could be burdensome and complex for both LMSM and stakeholders to navigate. Given the lack of access to knowledge and information about PrEP, HIV testing, and behavioral health treatments, they felt Dime Más needed to provide clear and accurate information to fill knowledge gaps, address misinformation, and enhance LMSM’s ability to navigate the healthcare system (Q12). To enhance Dime Más implementers’ knowledge and ability to navigate LMSM through the healthcare systems via Dime Más, they needed workflows, materials for outreach and delivering Dime Más, interactive and engaging training, supervision, and ongoing support from the study team (Q13).
Given the burdensomeness and complexity of the healthcare system, participants described the need for Dime Más to be simple and easy to access for LMSM (e.g., accessible in multiple ways, not overly time-consuming), and for Dime Más to simplify the process of obtaining PrEP, HIV testing, and behavioral health treatments. For example, they felt that after the initial Dime Más session, implementers should follow up with LMSM to address barriers they encountered to getting services and reduce the complexity of navigating these challenges, with some likening this to case management (Q14). Burdensomeness and complexity were also a consideration for implementers and within organizations. Stakeholders made suggestions for reducing the complexity and burden of implementing Dime Más, including creating flexible protocols, ensuring Dime Más integrates with the existing infrastructure of the organization, and receiving support from the Dime Más developers when implementing (Q15, Q16).
Resources and models of service delivery
The resources available to LMSM, implementers, and organizations within the local community were a concern for the development and implementation of Dime Más. Given the lack of available resources some LMSM may have (e.g., phone, time, transportation, financial), participants underscored the need for Dime Más implementers to be able to refer LMSM to free services and other support services that can facilitate access (e.g., free transportation to their clinics; Q17). Organizations also needed the financial resources and support to implement Dime Más, with participants commenting on the variability in resources within different organizations and the influence of external funding (e.g., CDC funding priorities) on resources. One resource that participants felt particularly strongly about was technology and telehealth, which they felt were more available in the context of COVID-19 and could facilitate the implementation of Dime Más (Q18).
Motivation to engage
Motivation and self-efficacy were additional considerations in developing and implementing Dime Más. Participants recommended Dime Más include activities, such as goal setting, to increase LMSM’s motivation to obtain PrEP, HIV testing, and behavioral health treatments. Participants also described the importance of attending to Dime Más implementers’ motivation (Q19) and building implementation motivation among leadership (e.g., ensuring managers and supervisors are motivated to implement Dime Más and invest in staff training). One way of building motivation was to provide rewards and reinforcement for participating in and implementing Dime Más. For example, participants suggested providing training certificates for implementers and organizations (Q20). Another strategy for building motivation and self-efficacy would be to leverage trialability, including offering implementers firsthand experience with Dime Más as part of their training and piloting Dime Más before proceeding to full-scale implementation (Q21). The degree to which Dime Más would add value for consumers, organizations, and the overall community could also influence implementation motivation, with many noting that it would add value by enhancing the reach of needed services to LMSM (Q22).
Discussion
Our findings inform refinements to one multilevel implementation strategy to scale up and out HIV-prevention and behavioral health treatments to LMSM, while also highlighting themes potentially relevant to developing other implementation strategies for the same purpose and demonstrating a community-engaged approach to doing so. The applicability of our findings beyond refining Dime Más is underscored by the fact that the EHE plan calls for implementation research to enhance the reach of evidence-based tools such as PrEP and HIV treatment to populations most impacted by the HIV epidemic (Fauci et al., 2019). As such, our findings and overall approach could be utilized to inform implementation research efforts aligned with the EHE plan. Finally, this project illustrates one approach to designing for implementation; Dime Más is being developed to meet both consumer and implementer/organizational needs, which may prevent a “voltage drop” (Chambers et al., 2013) as Dime Más proceeds through the translational pathway.
Pinto and colleagues (2021) describe the need for dissemination and implementation research models to include constructs of community engagement, and the relative gap between the community engagement and the dissemination/implementation literatures. Although our findings inform refinements to the implementation strategy that we are currently developing and other potential implementation strategies to achieve similar goals, another contribution of this work is that it demonstrates a community-engaged approach to developing an implementation strategy. Specifically, we included both consumer and implementer perspectives to shape the development and implementation plan for Dime Más, reflecting the strategy of “communication” identified by Pinto and colleagues. We will further expand on this community engagement as we refine Dime Más, seeking ongoing feedback from our Community Advisory Board of LMSM and implementing partners, reflecting Pinto and colleagues’ strategies of partnership exchange, leadership, and collaboration.
Our findings support many elements of the initial version of Dime Más (Figure 1), while also informing refinements. For example, we originally planned to include a peer ambassador component of Dime Más based on our DÍMELO findings and others’ research suggesting the importance of peer influence among racially/ethnically diverse MSM (Mutchler et al., 2015; O’Donnell et al., 2002; Quinn & Voisin, 2020). The current study suggests the need to expand and formalize the peer ambassador component to a greater extent than planned, which may also help address the stigma frequently discussed in the current study.
Similarly, we planned to provide Dime Más implementers with a referral list to enable tailored referrals based on LMSM’s needs (e.g., clinics that would not identify them as MSM, could deliver PrEP remotely, had bilingual providers, offer free transportation). We learned through the current study that this component also needs to be more robust and tailored to the local LMSM community. We are now in the process of developing a navigation tool, tailored to the needs of LMSM and stakeholders, to ensure they can identify local resources aligned with their needs. Based on our findings, we anticipate including within this tool a “review” feature that allows LMSM to comment on the degree to which organizations met their needs (e.g., were affirming, culturally competent, helpful). This tool can be used independently or within Dime Más and similar implementation strategies.
Additional refinements to Dime Más are informed by the convergence of the “available resources” and “cultural context” themes we identified. For example, given that some LMSM had privacy concerns linked to stigma (also observed by Harkness et al., 2021b), as well as a potential lack of resources to access in-person services, combined with the increased availability and infrastructure for telehealth, we plan to offer Dime Más as both an in-person and remote service, depending on participant preference. This is consistent with other research suggesting remote service delivery can enhance reach for behavioral and sexual health services among certain sexual minority men (Rogers et al., 2020; John et al., 2017), whereas others may prefer in-person (Turner et al. 2019). Although these findings are specifically relevant to Dime Más, they can inform the development of other implementation strategies with similar goals.
The findings also informed key decisions for implementers. Although we originally planned only to have LMSM implementers, our findings suggest this may not always be feasible. This echoes findings of minor improvements in care outcomes or overall perception of care for patients who were administered care from providers of the same race, ethnicity, or sexual orientation (see Cabral & Smith, 2011; Maramba & Nagayama Hall, 2002; O’Shaughnessy & Speir, 2018; Shin et al., 2005). Our findings suggested it would be ideal for LMSM to be implementers; however, non-LMSM could implement Dime Más if they were LGBTQ-affirming and skilled in working with Latino clients. At least some implementers in each organization implementing Dime Más need to be Spanish-speaking to ensure reach to monolingual Spanish-speaking LMSM. A related concern is considering the resources available within an inner setting before implementing Dime Más, a well-documented implementation determinant (Damschroder et al., 2009). Stakeholders raised important points such as the extent to which they had Spanish-speaking staff who could serve as implementers, the time existing staff had to implement a more intensive program like Dime Más, and the constraints placed upon them given the need to deliver services for which they received higher rates of reimbursement. As such, an addition to the provider-level implementation strategy is building a formal “implementation readiness assessment” to be conducted during the “preparation phase” (Aarons et al., 2011) of implementing Dime Más. Relatedly, we plan to conduct a cost analysis of Dime Más within our future pilot trial to understand the resources needed for implementation.
Secondarily, we observed that themes identified in this study, including cultural context, relationships and networks, and navigation of health information and systems are linked and can be addressed simultaneously through Dime Más and related implementation strategies. For example, enhancing LMSM’s ability to navigate health information and systems and increasing their awareness of their peers’ use of services may address stigma and further facilitate access to affirming resources. This is consistent with findings that among LMSM, stigma is associated with lower PrEP use intentions, an effect that PrEP knowledge may protect against (Hernandez Altamirano et al., 2020).
Despite this study’s strengths, it had limitations. Although we had broad representation from LMSM born in several countries outside the United States and with different citizenship statuses, White Latino MSM were represented to a greater extent than any other group. Despite being reflective of the demographics of Miami (Miami-Dade Matters, 2021) and the limitations of assessing race among Latino/a/x people as we did in the current study (Allen et al., 2011), we are working to increase the representation of non-White LMSM and exploring other ways of assessing race among Latino participants. Additionally, data were largely collected through focus groups, which have limitations, including potentially limiting dissenting viewpoints. Finally, we note that the interview guide included some direct questions that were less open-ended than our prior formative work (Harkness et al., 2021a), which evaluated barriers and facilitators to PrEP, HIV testing and behavioral health treatment in a more open-ended manner. Based on feedback from experts in intervention development and implementation science on our team, we needed to ask direct questions about specific components of Dime Más, given our goal of refining it using community and stakeholder feedback before developing a prototype. However, we acknowledge that asking direct questions in a qualitative interview can be limiting.
We also note the strengths and future directions for this research. We used an innovative analytic approach, integrating domains from an established implementation framework with inductively identified themes. This approach builds on guidance from Woodward and colleagues (2019, 2021) for integrating health equity into implementation science research and could be used in other health equity implementation research. Given the “voltage drop” often seen along the translational pathway (Chambers et al., 2013), this research centers the perspectives of both consumers and implementers, providing insights into how to tailor the consumer-facing component to LMSM needs and facilitate the implementation of Dime Más. Finally, our process in developing and refining Dime Más and the training program is iterative and multiphased. Based on the current findings, we will develop a prototype of Dime Más and the training program and theater test it with LMSM and stakeholders; this will provide another opportunity for feedback and alignment with community needs, resources, and priorities. Finally, although the current study guided refinements to Dime Más and the corresponding training program, the identified themes are potentially applicable to other implementation strategies that seek to achieve similar goals.
In summary, the current study identified LMSM and stakeholder perspectives regarding a multilevel implementation strategy to scale up and out HIV-prevention and behavioral health treatments to LMSM. The findings reveal the need for program developers, evaluators, and implementers to consider the needs of LMSM and stakeholders while developing and refining the implementation strategy. The study also illustrates a novel qualitative data analysis approach that integrates an established implementation science framework and allows for the inductive identification of themes.
Supplemental Material
sj-docx-1-irp-10.1177_26334895221096293 - Supplemental material for Refining an implementation strategy to enhance the reach of HIV-prevention and behavioral health treatments to Latino men who have sex with men
Supplemental material, sj-docx-1-irp-10.1177_26334895221096293 for Refining an implementation strategy to enhance the reach of HIV-prevention and behavioral health treatments to Latino men who have sex with men by Audrey Harkness, Elliott R. Weinstein, Alyssa Lozano, Daniel Mayo, Susanne Doblecki-Lewis, Carlos E. Rodríguez-Díaz, C. Hendricks Brown, Guillermo Prado and Steven A. Safren in Implementation Research and Practice
Footnotes
Acknowledgments
The authors would like to thank Daniel Hernandez Altamirano, Jaislene Viñas, and Michaela Larson for their assistance with this project. The authors also thank every participant in the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Safren receives royalties from Oxford University Press, Guilford Publications, and Springer/Humana press for books on cognitive behavioral therapy. Dr. Harkness receives royalties from Oxford University Press for a book related to LGBTQ-affirmative mental health treatment.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by K23MD015690 (Harkness), as well as author time supported by K24DA040489 (Safren). Additional research support was provided by U54MD002266 (Behar-Zusman), P30MH116867 (Safren), and P30DA027828 (Brown). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.