
Abstract
Background:
Implementation researchers have sought ways to use simulations to support the core components of implementation, which typically include assessing the need for change, designing implementation strategies, executing the strategies, and evaluating outcomes. The goal of this article is to explain how agent-based modeling could fulfill this role.
Methods:
We describe agent-based modeling with respect to other simulation methods that have been used in implementation science, using non-technical language that is broadly accessible. We then provide a stepwise procedure for developing agent-based models of implementation processes. We use, as a case study to illustrate the procedure, the implementation of evidence-based smoking cessation practices for persons with serious mental illness (SMI) in community mental health clinics.
Results:
For our case study, we present descriptions of the motivating research questions, specific models used to answer these questions, and a summary of the insights that can be obtained from the models. In the first example, we use a simple form of agent-based modeling to simulate the observed smoking behaviors of persons with SMI in a recently completed trial (IDEAL, Comprehensive Cardiovascular Risk Reduction Trial in Persons with SMI). In the second example, we illustrate how a more complex agent-based approach that includes interactions between patients, providers, and site administrators can be used to provide guidance for an implementation intervention that includes training and organizational strategies. This example is based in part on an ongoing project focused on scaling up evidence-based tobacco smoking cessation practices in community mental health clinics in Maryland.
Conclusion:
In this article, we explain how agent-based models can be used to address implementation science research questions and provide a procedure for setting up simulation models. Through our examples, we show how what-if scenarios can be examined in the implementation process, which are particularly useful in implementation frameworks with adaptive components.
Plain Language Summary:
The goal of this paper is to explain how agent-based modeling could be used as a supplementary tool to support the components of complex implementation processes. Such models have not yet been widely used in implementation science, partly because they are not straightforward to develop. To promote the use of agent-based modeling we provide a stepwise procedure using non-technical language and emphasizing the relationships between the model and implementation processes.
We used two detailed examples to demonstrate our proposed approach. In the first example, we simulate the observed smoking behaviors of persons with serious mental illness in a recently completed trial (IDEAL, Comprehensive Cardiovascular Risk Reduction Trial in Persons with Serious Mental Illness). In the second example, we illustrate how agent-based models that include interactions between patients, providers and site administrators can be used to provide guidance for an implementation intervention that includes training and organizational strategies. This example is based in part on an ongoing project focused on scaling up evidence-based tobacco smoking cessation practices in community mental health clinics in Maryland. For this example, we show how the visual user interface of an agent-based model can be in the form of a dashboard with levers for simulating what-if scenarios that can be used to guide implementation decisions.
In summary, this paper shows how agent-based models can provide insights into the processes in complex interventions, and guide implementation decisions for improving delivery of evidence-based practices in community mental health clinics.
Keywords
Brief description
The goal of this article is to explain how agent-based modeling could be used as a supplementary tool to support the components of complex implementation processes. Such models have not yet been widely used in implementation science, partly because they are not straightforward to develop. To promote the use of agent-based modeling, we provide a stepwise procedure using non-technical language and emphasize the relationships between the model and implementation processes.
We used two detailed examples to demonstrate our proposed approach. In the first example, we simulate the observed smoking behaviors of persons with serious mental illness in a recently completed trial (IDEAL, Comprehensive Cardiovascular Risk Reduction Trial in Persons with Serious Mental Illness). In the second example, we illustrate how agent-based models that include interactions between patients, providers, and site administrators can be used to provide guidance for an implementation intervention that includes training and organizational strategies. This example is based in part on an ongoing project focused on scaling up evidence-based tobacco smoking cessation practices in community mental health clinics in Maryland. For this example, we show how the visual user interface of an agent-based model can be in the form of a dashboard with levers for simulating what-if scenarios that can be used to guide implementation decisions.
In summary, this article shows how agent-based models can provide insights into the processes in complex interventions and guide implementation decisions for improving the delivery of evidence-based practices in community mental health clinics.
Motivation
Tobacco smoking in persons with serious mental illness (SMI) is the largest contributor to the 10- to 20-year premature mortality of this population (S. Brown, 1997; Colton & Manderscheid, 2006; Daumit et al., 2010; Olfson et al., 2015; Osby et al., 2001; Parks et al., 2006; Saha et al., 2007). Persons with SMI continue to smoke tobacco at an alarmingly high rate with an estimated prevalence of 50% compared to only 15% of adults overall (McClave et al., 2010). Quitting tobacco smoking has substantial benefits; smoking cessation in mid-life can eliminate 90% of smoking-related mortality (Pirie et al., 2013). Studies have shown that the vast majority of persons with SMI would like to quit smoking (Siru et al., 2009). Furthermore, evidence-based smoking cessation programs that combine pharmacotherapy with behavioral counseling have been shown to be effective in this population (Evins et al., 2008; Tsoi et al., 2013). There are, however, multi-level and multi-component challenges which impede the widespread implementation of such programs (Brown, Medoff, et al., 2015; Dickerson et al., 2018; Prochaska, 2011; Thorndike et al., 2001). For therapists or others who would deliver smoking cessation counseling, these challenges include time limitations in clinic visits and knowledge and self-efficacy barriers. Challenges at the mental health organizational and policy levels include lack of clinic-level systems to address smoking among persons with SMI and inadequate insurance reimbursement (Mechanic & Surles, 1992). Additional complexities in implementation include variations in provider characteristics, counseling format, length of treatment, and patient-level behavioral and social network factors that likely influence the effectiveness of smoking cessation programs. Hence, there is a pressing need to identify strategies for scaling up evidence-based smoking cessation programs for individuals with SMI that account for multiple challenges at the patient, provider, organizational, and policy levels.
Implementation Science Has Been Successful In Facilitating The Translation Of Other Complex Evidence-Based Practices In Public Health (Damschroder et al., 2009; Rongey et al., 2011). A Formal Framework Is Often Used To Guide Implementation Through A Process That Typically Includes Assessing The Need For Change, Designing Implementation Strategies, Executing The Strategies, And Evaluating Outcomes (Sales et al., 2006). Frameworks Such As The Plan-Do-Study-Act (Pdsa) Model (Taylor et al., 2014) And The Define, Measure, Analyze, Improve, And Control (Dmaic) Approach (Shankar, 2009) Also Include An Iterative Component For Adaptively Improving The Implementation. In Recent Studies, Researchers In Implementation Science Have Sought Ways To Use Simulation Methods To Support These Frameworks (Atkinson et al., 2015; Brown, PoVey, et al., 2015; Mckay et al., 2018; Moretto et al., 2019; Padek et al., 2018). In These Studies, Computer Models Are Used To Simulate Service Changes And Predict Impacts On Provider Efficacy And Patient Outcomes. Such Models Allow Decision Makers To Perform Simulated Scenario Analyses Of A Suite Of Candidate Service Changes To Help Inform Implementation Planning And Design (Powell et al., 2015). Current Efforts In This Research Area Have Been Focused On Improving Accuracy And Enhancing Modeling Capabilities Of These Computational Methods (Aarons et al., 2017; C. H. Brown et al., 2013).
The goal of this article is to explain how a specific simulation approach, known as agent-based modeling, can be applied to implementation studies, using non-technical language that is broadly accessible. To provide focus, we use a case study of the implementation of evidence-based smoking cessation practices for persons with SMI in community mental health clinics.
We begin by noting the limitations of using randomized clinical trials to answer research questions in complex interventions. Such trials are useful for analyzing the isolated effect of one particular intervention or intervention component, but generally require holding context and other factors constant. Trials with adaptive, factorial, and other innovative designs have been useful for more complex research questions, but randomized clinical trials, large enough to address multiple contextual factors, are likely to be prohibitively resource-intensive to conduct. Systems science methods have been suggested as an alternative approach to gain insight on the intervention effects in settings with complex features (Higgins et al., 2019). A systems model aims to represent a complex system, using a combination of data and expert knowledge, to understand how the components of the system fit and work together (Spadaro, 2007; Tracy et al., 2018).
Herein, we explain how systems models can be used to address implementation science questions, provide a procedure for setting up a simulation model, suggest opportunities for subject-matter experts to guide model development, and show how implementation leaders and stakeholders can use simulation model results. We examine implementation at several ecological levels and explain how a systems science method can be selected for each level. This selection process is guided primarily by the availability and completeness of data at each level and the research questions of interest. We also explain how the systems science methods at each level can be integrated to produce a single comprehensive model for simulating the implementation. Such a model can be used to examine what-if scenarios that can be used to make adjustments in the implementation process, which are particularly useful in implementation frameworks with adaptive components (Coury et al., 2017; DelliFraine et al., 2014; Rycroft-Malone et al., 2013).
In the “Methods” section, we describe systems science approaches known as microsimulation and agent-based models, which are particularly well suited for the study of complex implementations. We then provide a stepwise procedure for developing simulation models of implementation processes. In the “Results” section, we present two example applications that are relevant to the implementation of smoking cessation practices, with descriptions of the motivating research questions, specific methods used to answer these questions, and a summary of the insights that can be obtained from these methods. In the “Discussion” section, we explain the broader potential roles of systems science in implementation science.
Methods
Basic concepts of systems science
Systems science can be broadly defined by methods for modeling complex systems (Green, 2006; Hauptman, 1995), along with the theories that underlie these methods. In “systems science,” the word science refers to the algorithmic and statistical aspects of the numerical model and the domain knowledge associated with the system under study. The word system refers to a set of interacting entities that operate together as a complex whole, with boundaries that provide scope to the model (Klir, 2001). In the implementation of smoking cessation programs in community mental health clinics, the system boundary would not only include the clinic but also could expand beyond the clinical setting to include the people who interact closely with persons with SMI and other parts of the outer context (Aarons et al., 2011), such as government policies on reimbursement that can impact service availability.
Systems science is an evolving discipline, with sub-disciplines that have been led by experts from multiple research domains, including social and natural sciences, statistics, and engineering (Hauptman, 1995; Phillips & Kuhn, 1976). Herein, our primary interest is on agent-based methods, where agents are computer-simulated individuals embedded in a simulated environment. These agents can be endowed with physiological and behavioral features so that they respond to treatments, peer influences, and site-level directives. As explained below, these features make agent-based methods well suited for modeling the multiple processes associated with the scale-up of evidenced-based treatments, ranging from counselor–patient interactions in tobacco smoking cessation counseling sessions to site and geographically broader processes associated with implementation interventions (Burke et al., 2015; Luke & Stamatakis, 2012).
Before proceeding with more details about agent-based methods, it is useful to briefly review two other closely related methods. We begin with subject-specific time-series approaches that, while not usually classified as systems science methods, do provide a level of complexity that go beyond what is essentially a population-averaged approach typically generated by randomized trials and “standard” non-experimental studies. Subject-specific time-series approaches model longitudinal data to investigate variability in individual trajectories over time (Cook & DeMets, 2007; Eren-Oruklu et al., 2010). Microsimulation is a systems science approach that offers a higher level of complexity than subject-specific approaches by incorporating behavioral rules in the models of the individuals. For instance, in a microsimulation of a smoking cessation program, the model of the individual participants may include a mathematical rule for choosing to continue smoking or abstain, based on the rewards or other incentives offered by the program. Hence, microsimulation generates outcomes at the individual level; these are aggregated to provide population-level statistics. While microsimulation has found application in implementation studies, it is more widely used to evaluate policy impacts (Ballas et al., 2005; Crooks & Heppenstall, 2012; Hammar & Carlsson, 2005).
Agent-based approaches go even further than microsimulation by incorporating more complex behavioral mechanistic rules to govern a wide variety of interactions between agents and their environment. Here, the term agent can refer to a simulated individual, such as a patient, health care provider, or clinical site administrator, or entities, such as a group of individuals or a government agency. Agents can be endowed with intelligence to handle complex decisions, engage in complex interactions with other agents, and achieve one or more identifiable objectives (Crooks & Heppenstall, 2012). Interactions could include therapy sessions led by smoking cessation counselors, which affect the smoking abstinence behaviors of the patients and other intervention activities (Finch et al., 2013). Network approaches are often used to define the configuration of agents who interact with each other. For example, a network for a person with SMI may include their smoking cessation counselors and peer patients. These networks can be activated by motivational interactions that may positively influence the patient through group therapy sessions, follow-up phone calls or text messaging from counselors, and observation of peers exhibiting smoking abstinence (Schaefer et al., 2012, 2013).
Agent-based investigations typically begin with a baseline set of environmental conditions along with a synthetic population, which is a set of simulated individuals with properties drawn from a random distribution representing the population of interest. The initial run of the model produces simulated behaviors of each individual of this synthetic population in the specified environment. Subsequent model runs are done under alternate environmental conditions, such as those arising due to a policy or intervention. The simulated behaviors from these runs are analyzed to evaluate the impact of environmental changes on the population.
Application of systems science methods to the study of tobacco smoking cessation interventions
Table 1 displays systems science studies for tobacco smoking cessation interventions along with their research questions, specific methodologies, and primary outcomes. This table includes early system science studies using Markov and system dynamics models for representing behavioral characteristics, including Killeen (2011) and Timms et al. (2012), who studied time-varying trends of treatment effects of a population undergoing a smoking cessation intervention. Examples of microsimulation approaches are Martin et al. (1996), who used a transition analysis within each individual to model the effects of a smoking cessation intervention, with a latent variable representing incremental stages of change in the smoking cessation process and Chaloupka (1990) and Hammar and Carlsson (2005), who modeled tobacco smoking behavior as rational behavior reflecting the maximization of the smoker’s utility function. These examples are followed by more complex studies using agent-based modeling to examine aggregate patterns of addictive behaviors arising from peer interactions and their relationships with socioeconomic and other environmental characteristics (Chao et al., 2015; Macal & North, 2005; Pathak et al., 2007). Examples include Schaefer et al. (2012, 2013) and Sukthankar and Beheshti (2019), who used network models to investigate the effects of peer influences and social networks on smoking behaviors. The studies summarized in Table 1 are for interventions in general populations; these studies do not consider the particular complexities of smoking cessation interventions for individuals with SMI.
Systems science studies on interventions for tobacco smoking cessation.

PEM: prediction-error methods.
Conceptual map of systems science methods
To describe the data requirements of systems science methods, we use a simplified conceptual map of the models (Figure 1), with two axes. The vertical axis represents the degree of model complexity as reflected by the interactions between model components and by the simulated behavioral rules. The horizontal axis represents the input requirements, that is, the extent of information needed in the form of numerical data and/or domain expertise to describe the system of interest. Horizontal bars are used to indicate the complexity and input requirements of various systems science methods, mapped with respect to these two axes.

Conceptual map of systems science methods.
On the far left, near the bottom of this conceptual map, we place population-averaged approaches typically used in the studies that allow unbiased inferences about overall average effects without need for additional assumptions (e.g., randomized study designs). These would be models with no mechanistic rules, and hence low modeling complexity, which explains the low vertical position of the bar representing these models. This bar is also on the far left side because the data requirements, generally limited to patient characteristics, treatment indicator, and outcomes, are relatively low. When a research question can be answered through a standard experiment or non-experimental study, then complex models, such as agent-based models, would not be recommended. Following principles of statistical parsimony, the level of complexity of the model should be commensurate with and should not exceed the complexity of the processes being studied. Implementation scientists have, however, noted that there has been a trend toward increasingly complex implementations and more complex methods should be used for their study (Braithwaite et al., 2018; May, 2013). As we proceed to increasingly complex models, such as microsimulation and agent-based models with interacting agents, the position of these models in the conceptual map becomes progressively higher and trends toward the right. This is because models with higher complexity require more structure and a larger number of parameters to characterize their internal behavioral and decision-making algorithms, as well as more comprehensive data, which may come from multiple studies, to calibrate these parameters. While the horizontal bars do not extend all the way to the left at the low end of input requirements, it is still possible to develop preliminary models even when there is limited data available. In that case, such preliminary models would need to use assumed parameter values in lieu of available data, which would limit their accuracy as predictive models. These models, however, can still serve a purpose in investigating what-if questions at the conceptual level (Charfeddine & Montreuil, 2008; Diez Roux, 2012; Rongey et al., 2011). For instance, Greenwood-Lee et al. (2016) formulated a model that allowed researchers to see the pathways through which patient-provider gaming can influence patient outcomes, giving insights into how gaming behaviors can arise within an intervention and introduce unanticipated effects. Such models may be the only option in the beginning of the implementation process, when there is generally very limited available data. These models can be helpful in uncovering potential issues and identifying barriers and strengths in the critical early phases of implementation (S. Lin, 2017; Powell et al., 2015). Below, we use the term conceptual agent-based models to emphasize their focus on developing insights and possible explanations for observed behaviors (Boero & Squazzoni, 2005).
General procedure for applying systems science methods
The procedure for applying systems science to the study of implementation processes has these basic steps:
Articulate research questions relevant to the implementation.
Identify one or more systems science models that could be used to answer the research questions. The conceptual map of Figure 1 can be used as a guide for selecting candidate models with the levels of complexity needed for each question and with input requirements commensurate with available data and other sources of information. Models for more complex interventions involving implementation processes at the provider, site, and policy levels would typically be selected from those in the upper portion of this conceptual map.
Formulate the models using data and domain expertise from researchers and practitioners familiar with the implementation.
Run the models to obtain numerical results that can be used to explore possible emergent patterns of behavior. What-if scenarios can be investigated by rerunning the models with alternate implementation strategies. Variance estimates and confidence intervals can be obtained using synthetic populations to generate an ensemble of model runs.
Use the model outputs to give guidance toward the answers to the original research questions.
Construct a dashboard, if this is of interest, to provide implementation leaders and other decision-making stakeholders with a practical interactive tool to gain insights into the implementation processes.
The above general procedure can be applied to many kinds of complex interventions; in Table 2, we provide specific models, research questions, and parameter requirements that are applicable to the study of implementations of smoking cessation treatment practices for persons with SMI. The models in the top rows of the table focus on the interactions between persons with SMI and mental health providers, including therapists, physicians, and nurse practitioners. As noted earlier, population-averaged approaches and microsimulation are appropriate approaches for analyzing such interactions. The next rows of Table 2 include increasingly complex modeling approaches, including agent-based simulations of intervention implementations with adaptive and iterative processes. Below this are models for interactions through peer influence networks, such as in-group intervention programs. Finally, the last rows of Table 2 include approaches with hierarchical representations of implementations that incorporate site and program administration.
Systems science models for the study of smoking cessation programs.

SMI: serious mental illness.
Results
We demonstrate the procedure for applying systems science with two examples related to smoking cessation. In the first example, we use microsimulation to model the observed smoking behaviors of persons with SMI in a completed trial (Dalcin et al., 2018). In the second example, we illustrate how a conceptual agent-based approach can be used to provide guidance for an implementation intervention that includes training and organizational strategies. This example is based in part on an ongoing pilot project focused on scaling up evidence-based tobacco smoking cessation practices in community mental health clinics in Maryland (McGinty et al., 2021).
Example 1: microsimulation of smoking behaviors
Research question
In the first example, the research question of interest is: What are the characteristics that relate to willingness to quit in smokers with SMI? We used control group data from the IDEAL trial, which was an NHLBI-funded randomized controlled trial of a comprehensive cardiovascular risk reduction program for persons with SMI (Daumit et al., 2019). There were 73 control group participants who were smokers at baseline with missing data on the variables needed for this analysis for only 4 of them. Given this low missingness, for this illustrative example, we restricted our analysis to the 69 individuals with complete data on the analysis variables. Smoking status was recorded at 18 months and we took this as the final outcome. Table S1 summarizes the baseline characteristics of the sample, and Table S2 summarizes the subset of longitudinal data that is related to smoking status and willingness to quit.
Model selection
The most appropriate systems science models for this research question are in the lower portion of Figure 1 because of the emphasis on individual-level behaviors. Since the control group participants did not receive tobacco smoking cessation counseling in the study, we did not need to use agent-based models with interacting agents. We had access to longitudinal and other data needed to develop a microsimulation model; hence, this is the model we selected.
Model formulation
The modelers held meetings with implementation team members to review the trial data and to obtain assistance in selecting a subset of the data that was considered to be most relevant to smoking behavior. Subsequently, the modelers presented an overview of microsimulation methods, so that the implementation team could choose modeling components that they felt would be most useful from the implementation perspective. It was found that their primary interest was on the time-varying nature of smokers’ quitting processes; they noted the importance of understanding these processes particularly in adaptive interventions. Based on these suggestions, a microsimulation model with explicit time dependence of the internal state and smoking status of each individual smoker was chosen by the modelers. To keep this analysis as simple as possible, we used a single-state variable, S, to represent the patient’s willingness to quit smoking. Three ordinal levels for this state variable (low, medium, and high) were assigned to each participant using the longitudinal data summarized in Table S2 and the rules explained in Table 3. An ordinal logistic equation is used to calculate the likelihood of state variable S at baseline, and the transition probabilities from one state to another during the time intervals from baseline to 6 months and from 6 months to 18 months are obtained by logit functions. A Markov analysis is then used to propagate the probabilities of the states of willingness to quit at baseline to the probabilities of the states at 6 and 18 months. This analysis is based on the Markov property that the state at each time point depends explicitly on the state at the prior time point; in this manner, we retain and quantify the highly correlated nature of longitudinal data. Using this formulation, we computed for each patient the probabilities of willingness to quit at 0, 6, and 18 months. Lasso regression is used to select and reduce the number of regression variables in the final predictive model of quit status at 18 months; details of the model formulation are given in Supplementary Material 1. While it is possible to develop a simpler model for predicting smoking status at 18 months by regressing on baseline characteristics, the proposed system model has the advantage of capturing the dynamic time-varying nature of the quitting process, including intermediate levels of willingness to quit prior to abstinence. As noted in the “Discussion” section, such time-dependent models can be useful for adaptive interventions.
Definitions of the state variable S representing willingness to quit smoking.

Note. Based on survey questions: 1. Are you seriously thinking of quitting smoking? 2. Do you now smoke cigarettes every day, some days, or not at all? 3. During the past 12 months, have you stopped smoking for 1 day or longer because you were trying to quit smoking?
Model guidance
Our model predicts that over half of the control group participants do not increase their willingness to quit smoking and only a few participants attained abstinence at 18 months (Table S6). This is in line with previous studies, which have emphasized the importance of including both pharmacotherapy and behavioral counseling in smoking cessation practices for persons with SMI (Evins et al., 2008; Tsoi et al., 2013). Our model also indicates the association of baseline characteristics with initial willingness to quit (Table S3), the Markov transition probabilities between states of willingness to quit (Table S4), and the final abstinence status at 18 months (Table S5). While the tables indicate that only race is significantly associated with willingness to quit (p = .007), it is noted that the purpose of this example is to illustrate the procedure of developing a microsimulation model for smoking interventions rather than providing conclusive results based on such a model. Most of the microsimulation model components, including the state variable S for the willingness to quit, the Markov analysis of this state over time, and the predictive model of quit status, will be used as a starting point in the future versions of the models that would include the effects of evidence-based interventions. These microsimulation models could be then used in guiding implementation interventions for smoking cessation practices, particularly when the intervention spans multiple sites with varying patient characteristics. The model would identify sites with patient populations that are predicted to have lower quit rates and may hence require more resources and effort. To illustrate this last point, an extension of this example is included in Supplementary Material 1. Here, we generate simulated patients based on the population characteristics of two sites in another recently completed smoking cessation trial and use our microsimulation model to compare predicted quit rates at each site.
Example 2: agent-based modeling of a multi-site smoking cessation intervention
Research questions
In this example, the research questions of interest are: (a) During the early stage of implementation, which implementation components should be adjusted? (b) What would be the impact on persons with SMI who smoked if there was a state-level requirement for offering evidenced-based treatment for tobacco smoking cessation? The second research question is prompted by guidelines that recommend assessing and offering treatment to all tobacco users, not only those interested in quitting right away (Arnett et al., 2019; Cagan, 2019; Cather et al., 2017; Evins et al., 2015). Our modeling effort here is informed by a planned pilot implementation intervention in Maryland which includes several implementation strategies designed to improve the delivery of evidence-based smoking cessation treatment in mental health clinics targeting providers and the organization. The components include (1) clinician training and protocols for assessing smoking status and willingness to quit, behavioral counseling, and smoking cessation pharmacotherapy; (2) expert consultation on smoking cessation treatment; (3) meetings with organizational leadership to support organization-level changes; and (4) coaching for smoking cessation counselors to enhance evidence-based practice delivery.
Model selection
Given the complexity of the implementation intervention components, including multiple types of interacting individuals, an agent-based approach with a high level of complexity is needed. Agent-based modeling, as shown in previous studies in Table 1, can also include the dynamic time-varying nature of quitting. As indicated for the first example, such time-dependent models are particularly attractive for informing adaptive interventions. Since only limited data are currently available for calibrating an agent-based model, the goal of this modeling exercise is to gain insight into the implementation processes rather than obtaining numerical predictions for outcomes. In the following, we explain how we develop a conceptual model with large scope and high complexity, but with limited data, as represented in the upper left of Figure 1.
Model formulation
We worked with experts with experience in smoking cessation interventions to formulate a preliminary agent-based model to study research questions (a) and (b). We began by presenting the basic concepts of agent-based modeling to the domain experts and proceeded with the identification of the agents, such as providers and patients, and their behaviors that were most relevant to the research questions. Second, the experts identified the assumptions needed to model those agent’s behaviors. Using this initial model design, the modelers proceeded to formulate the governing equations to represent the interactions and behaviors of the agents. Details of the assumptions in the model and the equations governing agent interactions and behaviors are provided in Supplementary Material 2. We note that agent-based models typically rely on a relatively large number of assumptions, and a key part of the model-building process is the assessment of the sensitivity of the model to such assumptions (Klügl, 2008).
For our illustrative example in this article, we begin with a model of the simplest interaction, as shown in Figure 2(a). Here, there are two agents, one patient and one smoking cessation counselor; the model is formulated to include the interactions between the two agents and the influence of this interaction on smoking cessation. (Technical details can be found in Supplementary Material 2 in the section, Basic Model of Patient–Counselor Interactions.) It is assumed that the simulated patient who quits smoking will receive positive feedback from the smoking cessation counselor in the form of encouragement. This feedback would be quantified and explicitly modeled in the interaction between the simulated patients and smoking cessation counselors. Moreover, it is assumed that the effects of this feedback would influence subsequent patient behavior, particularly in regard to continued abstinence (Chao et al., 2015). An additional assumption is that this feedback would be reinforced if data from monitoring devices, such as CO-based smokelyzers, were consistent with the patient’s self-reported quit status.
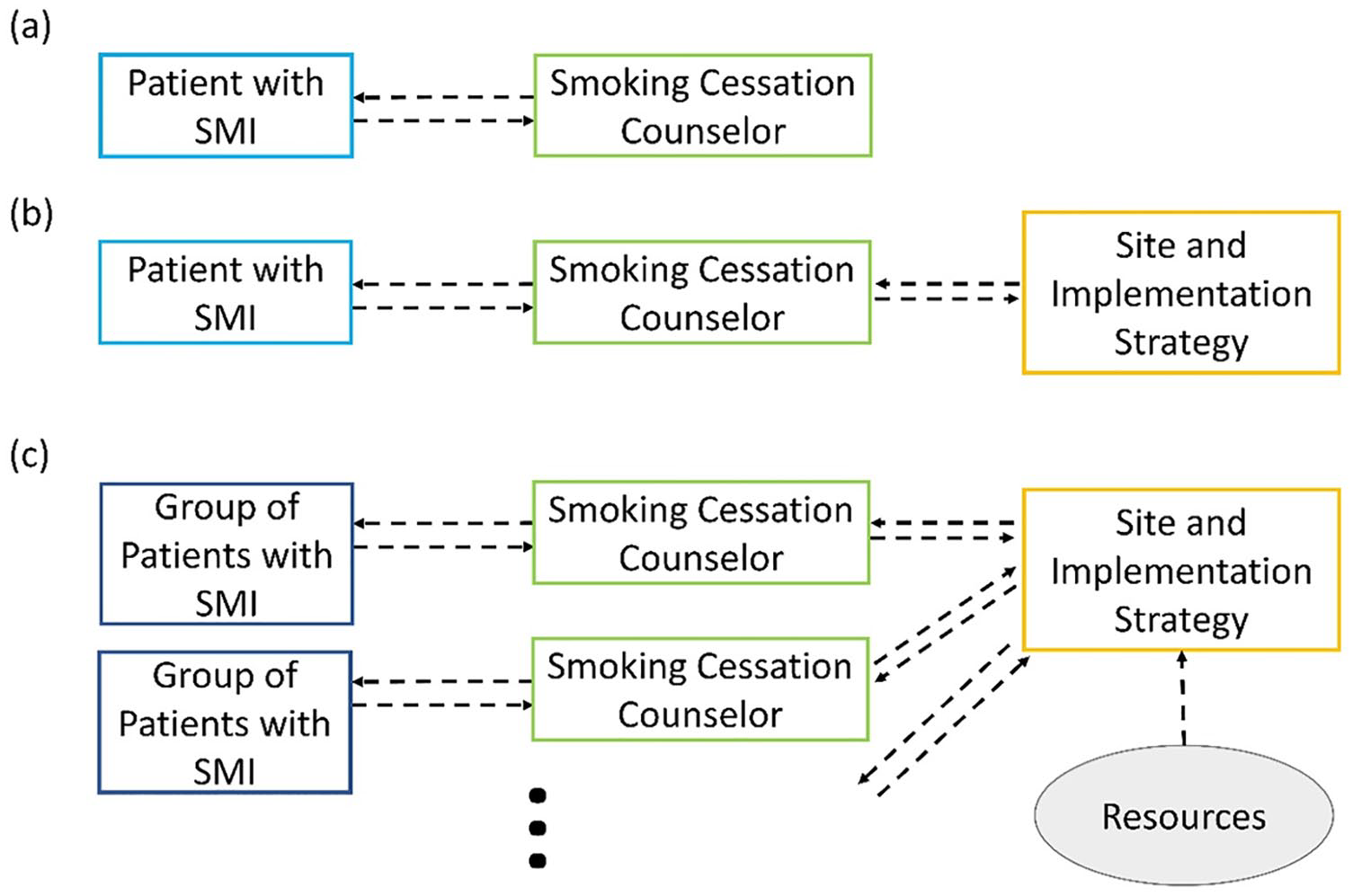
Series of increasingly complex systems science models for the smoking cessation program example: (a) ABM with basic patient–counselor interaction, (b) ABM with basic organizational network, and (c) ABM with multi-site organization and resource allocation analysis.
A model with an additional level of complexity includes the clinic management, who oversee the ultimate, real-world implementation of the smoking cessation program. (For technical details, see Supplementary Material 2 in the section, Simulated Site-Level Processes Section.) This model will include a hierarchical network that is used to represent the flow of information and interactions between clinic management, smoking cessation counselors, and patients, as indicated in Figure 2(b). The final model will also include multiple sites that are networked through association with the implementation intervention team, which oversees the entire implementation process, as shown in Figure 2(c). (For details, see Supplementary Material 2 in the section, Multi-Site Organization Section.) The systems science modeling methods that underlie the diagrams in Figure 2 include state variables, which quantify the level of fidelity of the smoking cessation counselors and the willingness to quit of the persons with SMI, utility functions, and networks, Markov analysis in terms of these state variables and utility functions, and a function for smoking cessation intervention effectiveness that depends on site characteristics, such as staffing levels and patient population. Details of the model formulation are provided in Supplementary Material 2.
Model runs
While the domain experts who have developed the implementation project have been involved in the model design as indicated above, data from the intervention are not yet available. Once data are obtained, it would be used to calibrate the model parameters and produce numerical model runs. At the onset of model development, it is generally not possible to determine a priori the number of simulation runs required for validation analysis because the output distributions are usually unknown; an iterative approach is generally required (Hamill, 2010; Lee et al., 2015). Studies that have addressed this issue include Castiglione and Winslow (2003), D. Y. Lin et al. (2008), and Camargo (2020). Given our emphasis on introducing the concepts of systems science models and their utility in guiding implementation interventions (e.g., identifying the implementation components most crucial for success), in the remainder of this example we describe a conceptual demonstration, a dashboard, that could be constructed after the needed data become available and the agent-based model is calibrated.
Dashboard
An example of a dashboard that could be developed for this example is shown in Figure 3. On the right side of the dashboard, site-level outcomes predicted by the agent-based simulations are displayed as a series of bar charts. These outcomes include site-level quit rates and levels of fidelity to the smoking cessation practices and provider self-efficacy. On the left side are three panels of sliders and switches. The top panel contains sliders that characterize the tobacco smoking cessation program at each site, including the number of persons with SMI, smoking cessation counselors, and other mental health providers participating in the program, average level of program acceptance among site staff, and level of screening for tobacco smoking. The middle panel contains controls that characterize the smoking cessation program itself, including counselor skill level, counseling frequency, and pharmacotherapy frequency. These are essentially levers of control of the implementation intervention that can be used to investigate what-if scenarios. For instance, it is possible to observe simulation results for the trade-off between the number of smoking cessation counselors and the skill level of these counselors, in response to research question (a). Variations of smoking cessation rates with respect to changes in patient characteristics can also be explored, as well as the effects of counselor training. The bottom panel contains switches for external effects. For example, when the first switch is turned on, tobacco smoking cessation programs become a state-level requirement, which triggers reimbursement changes. The outcomes displayed on the right would indicate the site-level impacts of the policy, which is of interest in research question (b).

Dashboard for Example 2: agent-based modeling of smoking cessation implementation intervention.
Discussion
We illustrate how a stepwise procedure can be used to develop systems simulation models to address research questions related to the study of implementation processes. The examples illustrate how microsimulation and agent-based models can incorporate behavioral rules at the individual level and handle multi-level interactions at the organizational level.
The microsimulation model in the first example provides, at each time step, an update of the predicted quit status at the end of the study. This feature of the model could be useful in implementation scenarios with adaptive interventions. The predicted future trajectory of the patient status could be used to inform and adjust dose and other intervention components.
Similarly, the agent-based model of the second example could be useful in implementing adaptive interventions, providing information at the site-level scale. For example, when progress in patient responses differs significantly from expectations, the model can be used to simulate and assess candidate service changes, such as increased provider training. In this manner, agent-based models could support implementation frameworks, such as the PDSA (Taylor et al., 2014), DMAIC (Shankar, 2009), and other approaches noted in the “Introduction” section.
We now describe possible further enhancements to these models. The natural extension of the microsimulation model for patient-smoking behaviors in Example 1 is to add the effects of pharmacotherapy and of smoking cessation behavioral counseling. These effects would be incorporated into the model through increases in the Markov transition probabilities to higher levels of willingness to quit. The magnitude of these effects can be in terms of the characteristics of the smoking cessation counselor, such as fidelity to the intervention protocol, self-efficacy, and the efficacy of pharmacotherapy. The model could then be used to investigate the variability between persons with SMI in smoking abstinence outcomes when exposed to the same smoking cessation treatment. When these results are aggregated at the site level, then variations between sites with different population characteristics and intervention strategies can be explored.
Example 2 could be enhanced in several ways. For instance, it is possible to model group sessions by introducing a network analysis of groups of patients interacting with each other and their smoking cessation counselor. Here, positive peer influence of persons with SMI who are abstaining from smoking and the counteracting negative peer influence of patients who continue to smoke would be added to the utility functions embedded in the agent-based model. Other relevant network analyses include the impact of follow-up phone calls from the health counselors to persons with SMI, using intervention levers for the frequency of phone calls and the degree of encouragement communicated through these calls.
Complex interactions based on game theory can also be introduced at multiple levels. Such complexity arises whenever the interactions between two or more agents influence their respective utility functions. For instance, at the patient–counselor level, the patient may be seeking ways to maximize the receipt of rewards and other encouragement from the counselor while the counselor is seeking ways to maximize the likelihood that the patient will abstain from smoking. Patients who are able to exhibit signs of willingness to quit without the intent of abstaining would be gaming the intervention, even if the lack of intent is not deliberate, and this type of interaction would need to be incorporated into the model so that possible adjustments to the intervention can be effectively explored.
External effects would be modeled through their influences on the agents and processes within the agent-based model. In the dashboard in Figure 3, the external effects panel has four switches corresponding to the following four external effects: changes in Medicaid reimbursement for pharmacotherapy and behavioral counseling; a state requirement to offer smoking cessation treatment to all who smoked, which might increase the providers’ acceptance of this treatment; and restrictions on workforce expansion, which may arise due to skilled medical labor shortages, resulting in constraints on smoke cessation counseling. Since the simulations in the agent-based model include detailed interactions between counselors, prescribers, and persons with SMI, the impacts of external effects can be modeled mechanistically through a chain of events. For instance, the effect of a decrease in Medicaid reimbursement of behavioral counseling would enter the agent-based model through a reduction of the number of smoking cessation counselors, which in turn would increase the patient load per counselor and decrease the frequency and duration of each counseling session, which would then result in a reduced influence on willingness to quit, which would ultimately lead to a lower quit rate.
Finally, the microsimulation model of Example 1 and the agent-based model of Example 2 can be merged into a single integrated model. Essentially, details of the patient behavioral processes that are examined in the microsimulation model can be incorporated into the simulated patients of the agent-based model. This would provide greater depth in the model that would be useful for formulating the game theory models of agent-to-agent interactions and for investigating a wider range of research questions related to the intervention and its implementation.
It is important to keep some limitations of these methods in mind. As alluded to earlier, a general limitation of agent-based approaches is the need for detailed data to calibrate the model parameters, particularly for the more complex models that extend to the right side of the conceptual map in Figure 1. One way to address this limitation is to expand the data collection effort to parameterize all of the variables described in the third column of Table 2. The second way is to use simpler agent-based models, as shown in the bottom right of Figure 1. While this will provide greater assurance of model fidelity, the resulting models would no longer have the ability to address the range of research questions noted earlier, particularly those related to complex implementation processes (Higgins et al., 2019).
Another limitation that is broadly applicable to predictive models is that they are simplified representations of real-world systems. Hence, the simulation models should not be viewed as precise predictive tools but should be used primarily to gain insights into the intervention processes that can help implementation teams to better understand barriers in their interventions and design possible improvements. The conceptual map in Figure 1 provides a modeling perspective, with various levels of desired modeling complexity shown with respect to the level of data requirements. In the future, as research in modeling approaches advances and as more data become available, then we would be able to move upward and to the right of this conceptual map, with increasing accuracy and range of applicability of systems science models.
Conclusion
In this article, we provide a description of systems science simulation methods for the study of complex interventions, using applications focused primarily on smoking cessation to maintain a unified theme in illustrating concepts. We use a stepwise approach to show how the methods could be used in practice. While expertise in modeling is required within some of these steps, the overall procedure is written in a manner that we believe could be appreciated by a wide audience. We provide two contrasting examples that illustrate simulation modeling at two levels, one at the individual level that focuses on patient behavior and the other at the multi-site level that incorporates organizational effects.
Those involved in site-level implementation planning and assessment would benefit from microsimulation and agent-based models that show the impacts of the implementation process. Policy-level stakeholders who wish to examine broader impacts would be interested in dashboards and other simulation-driven visualization tools that can provide projections at the community or wider levels. While there is ongoing research work to improve the accuracy of systems science simulation methods, there is growing recognition in public health, particularly in implementation science, in the need to expand utilization of such multi-level, complex approaches.
Supplemental Material
sj-pdf-1-irp-10.1177_26334895211010664 – Supplemental material for Agent-based modeling for implementation research: An application to tobacco smoking cessation for persons with serious mental illness
Supplemental material, sj-pdf-1-irp-10.1177_26334895211010664 for Agent-based modeling for implementation research: An application to tobacco smoking cessation for persons with serious mental illness by Wanyu Huang, Chia-Hsiu Chang, Elizabeth A Stuart, Gail L Daumit, Nae-Yuh Wang, Emma E McGinty, Faith B Dickerson and Takeru Igusa in Implementation Research and Practice
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health, P50MH115842.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.