
Abstract
Background:
Kawasaki disease (KD) is a rare medium-sized vessel vasculitis that is the leading cause of acquired heart disease in children. However, most studies on KD focused on its occurrence in infants aged <6 months.
Objectives:
To evaluate the clinical characteristics, treatments, and complications of KD in Peruvian children.
Design:
Retrospective observational study.
Methods:
We collected data from patients aged <18 years who were diagnosed with KD and hospitalized at four healthcare institutions in Lima, Peru, between 2010 and 2022. Clinical characteristics, treatments, and complications were described overall and by age (groups A: <6 months, B: 6 to <12 months, C: 1 to <5 years, and D: ⩾5 years).
Results:
The median age was 2.3 years (interquartile range: 1.4–4, range: 1 month–13.2 years), and 68% were male. Group A had fewer oral mucocutaneous symptoms, whereas groups C and D had higher frequencies of cervical lymphadenopathy than the other groups. Gastrointestinal symptoms and incomplete KD presentation were common in groups A and D. Elevated white blood cell counts, platelet counts, erythrocyte sedimentation rates, and C-reactive protein levels were observed, particularly in patients with an illness duration of >10 days. A second dose of immunoglobulin was administered to 32 patients, and corticosteroids were administered to 48 patients (21.3%). Immunoglobulin resistance occurred in 14.8% of the patients, predominantly in group D. Coronary aneurysms were observed in 25 patients (12.1%), predominantly in group A. Two patients required intensive care unit admission, and no deaths occurred during hospitalization.
Conclusion:
Mucocutaneous manifestations of KD in Peruvian children are consistent with those reported in other populations. The frequency of aneurysms and immunoglobulin resistance differed according to age. We emphasize the importance of understanding the clinical presentation of KD, both overall and stratified by age, to prevent late diagnosis and ensure timely treatment.
Plain language summary
Kawasaki disease (KD) is rare in children. KD was initially described in Asian children and later reported in other countries. Its most common complication is coronary artery damage. Treatment consists of administering high-cost medications (immunoglobulins) that are not always available in healthcare institutions in low- and middle-income countries.
The study aimed to evaluate the clinical characteristics, treatments, and complications of KD in Peruvian children.
In our study on Peruvian children with KD, we found that the clinical characteristics were similar to those reported in studies from other countries. The frequencies of coronary aneurysms and immunoglobulin resistance varied with age. A group of children were diagnosed late (>10 days) because the healthcare workers misdiagnosed them with other childhood infectious diseases. The treatment was consistent with the recommendations of international institutions. Immunoglobulins and aspirin were the most commonly used drugs.
The results of this study provide information on KD stratified by age group and include the most significant number of children with this rare disease in Peru, utilizing data from hospitals that are representative of the Peruvian healthcare system.
Introduction
Kawasaki disease (KD) is a medium-sized vessel vasculitis that typically presents as an acute febrile illness in children under 5 years of age. 1 Since its first description in Japan in 1967, 2 KD has gained global attention because of the associated cardiac complications such as coronary artery aneurysms. 1
The incidence of this condition is higher in Asian countries than that in Europe and North America, 3 likely because of a genetic predisposition. 1 The etiology remains unknown; however, the proposed triggers, such as infectious agents and environmental particles, may be associated with genetically predisposed children. 4
In Latin America, efforts have been made to characterize KD 5 more comprehensively, although most studies have focused on its occurrence in infants age <6 months.5–7 Diagnosis is particularly challenging at extreme ages (<1 and >5 years), often leading to delays and an increased risk of coronary involvement if treatment is not promptly initiated.7–9
Differences in the clinical characteristics and complications have been associated with patient subgroups affected by this disease. 10 Given the heterogeneity of healthcare resources and systems across countries, we aimed to describe Peruvian experience regarding KD diagnosis and management.
This study aimed to describe the clinical characteristics, treatments, and complications of KD in Peruvian children, both overall and by age.
Methods
Design and population
This was a retrospective, observational study. This study was conducted in accordance with the Strengthening the Reporting of Observational studies in Epidemiology guidelines (Supplemental Material 1). 11
Data were obtained from the physical and electronic medical records of children diagnosed with KD who were hospitalized in four hospitals in Lima, Peru: the Instituto Nacional de Salud del Niño-Breña (INSN-Breña) (2010–2022), Hospital Nacional Edgardo Rebagliati Martins (2010–2022), Hospital Nacional Arzobispo Loayza (2019–2022), and Hospital de Emergencias Villa El Salvador (2019–2022). These institutions have experience with KD diagnosis and access to standard treatment.12,13 Additionally, they have specialties related to the disease that can aid in the timely diagnosis of cardiac complications.
Selection of participants
The KD diagnosis was based on the 2004 and 2017 American Heart Association (AHA) criteria14,15 (Supplemental Material 2). All patients were evaluated by an infectious disease specialist or cardiologist for diagnosis.
We included 225 patients diagnosed with KD based on the AHA criteria in the emergency room, consulting room, or upon hospitalization. Patients with diseases simulating KD (82 patients with multisystem inflammatory syndrome and one patient each with abscessed adenitis, dengue, thrombotic thrombocytopenic purpura, sepsis, scarlet fever, systemic lupus erythematosus, and urinary tract infection), those whose medical record were not accessible (117 patients), and those who were referred to other institutions (one patient) were excluded. The participant selection is shown in Supplemental Material 3.
The sample size was not estimated because of the limited number of cases, as KD is a rare disease. Data collection was performed by five investigators and, in the event of discrepancies, a sixth investigator performed the review.
Study variables
One of the study variables was age, which was subdivided into four groups: Groups A (<6 months), B (6 to <12 months), C (1 to <5 years), and D (⩾ 5 years). The patients were subdivided into these groups according to previous reports7,9,16 and their findings suggesting that age may help identify clinical subgroups within KD. 10 Additional variables included sex, comorbidities, origin, month of diagnosis, time of hospitalization, symptomatology (mucocutaneous, respiratory, neurological, or gastrointestinal), and form of presentation according to the AHA definitions (complete, incomplete, or atypical)14,15 (Supplemental Material 2).
Laboratory parameters, treatment characteristics (immunoglobulin, corticosteroid, acetylsalicylic acid, anticoagulation, and antibiotics), complications such as echocardiographic alterations (coronary aneurysms), admission to the intensive care unit (ICU), and immunoglobulin resistance were also recorded.
All variables were described overall and stratified according to age. Laboratory findings were described both in general and by time of disease: ⩽10 (acute phase) vs. >10 (subacute phase) days. 17
Statistical analysis
Data were entered into a database in Microsoft Excel ® (Windows 10 version) and analyzed using STATA v.17 software (StataCorp LP, College Station, TX, USA). Because the objective of the study was to describe the characteristics of all cases of Kawasaki disease, we did not perform hypothesis testing. Categorical variables are reported as absolute and relative frequencies, and quantitative variables as median and interquartile range (IQR) based on their distribution, as assessed by histogram analysis.
Ethical aspects
This study was approved by the Research Ethics Committees of INSN-Breña (No 128-2023-CIEI-INSN), Hospital Nacional Edgardo Rebagliati Martins (No 637-GRPR-ESSALUD-2023), Hospital Nacional Arzobispo Loayza (No 18-2023-HNAL-P), and Hospital de Emergencias Villa El Salvador (No 001-2024). Informed consent was not required because the information was collected directly from medical records, and the confidentiality of the data was safeguarded using numerical identifiers.
Results
During the study period, 432 medical records containing the International Classification of Disease-10 diagnosis of KD were obtained. Records without a final diagnosis of KD (n = 90) and those unavailable for review (n = 117) were excluded (Supplemental Material 3). The final analysis included medical records of 225 patients.
General and clinical characteristics
The general and clinical characteristics of the patients are shown in Table 1. The median age was 2.3 years (IQR: 1.4–4 years, range: 1 month 3 days–13.2 years), and there was a higher frequency of cases between 1 and 5 years. The cases were distributed across all months of the year, with the highest frequency observed from April to July (Figure 1(a)). Infants aged <1 year (groups A and B) accounted for approximately 30% of the cases in April and November, whereas group D showed higher frequencies in January, February, and August (Figure 1(b)). Seven patients had comorbidities (one patient each with atopic dermatitis, neurofibromatosis type 1, migraine, attention deficit hyperactivity disorder, epilepsy, latent tuberculosis, and partial anomalous pulmonary venous drainage). Among the mucocutaneous manifestations, oral changes were less frequent in group A, whereas lymphadenopathies were more frequent in groups C and D. Respiratory symptoms were reported in 33% of the cases and were common in group A. Neurological symptoms were reported in 5.8% of the cases and were common in group D. Gastrointestinal symptoms were common in group D, with diarrhea present in half of the patients in group A (Table 1). Four patients had atypical KD because of their initial presentation (two with aseptic meningitis and one each with staphylococcal shock syndrome and angioneurotic edema).
General and clinical features of children with Kawasaki disease.
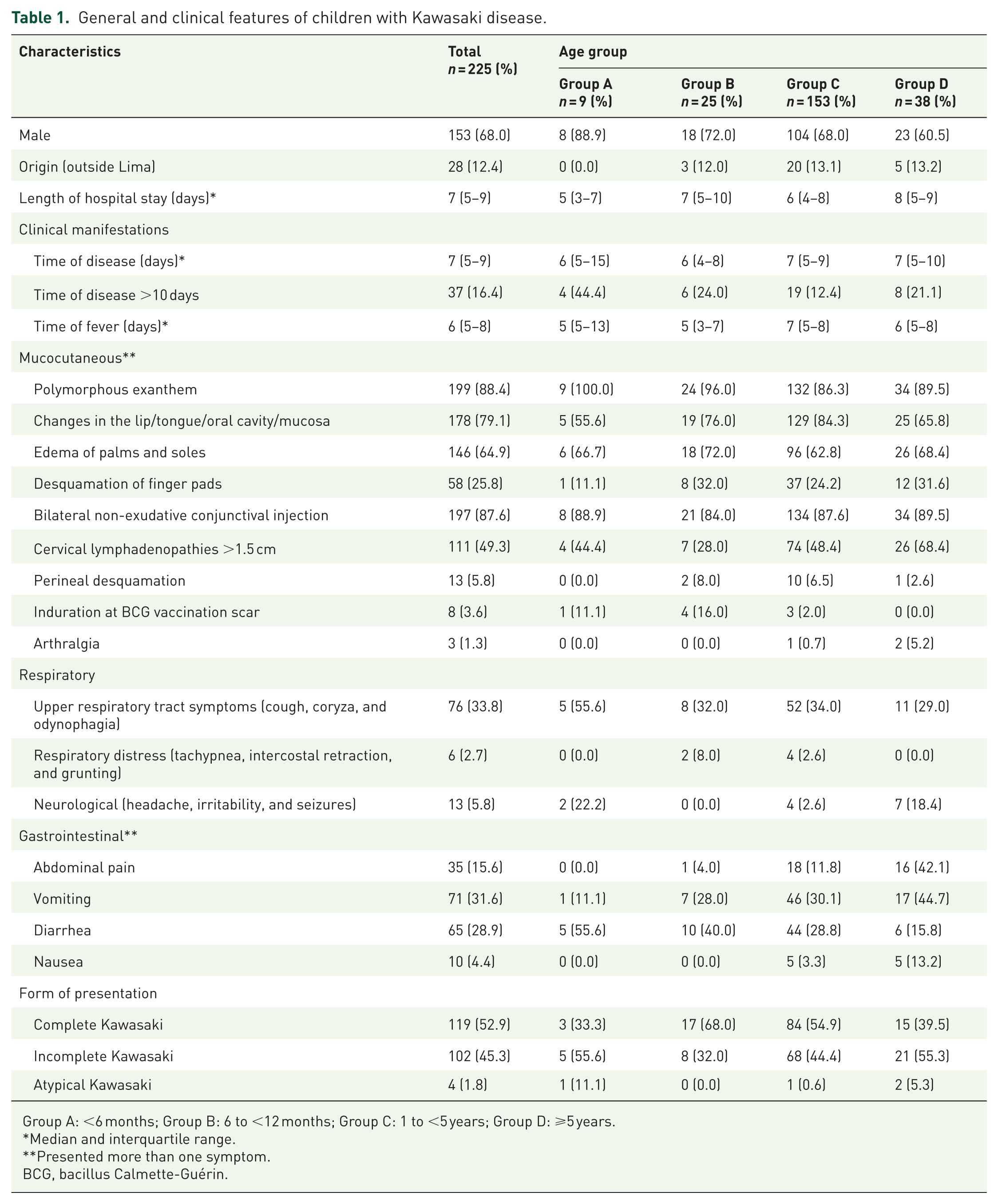
Group A: <6 months; Group B: 6 to <12 months; Group C: 1 to <5 years; Group D: ⩾5 years.
Median and interquartile range.
Presented more than one symptom.
BCG, bacillus Calmette-Guérin.

(a) Number of Kawasaki disease cases per month from 2010 to 2022. (b) Percentage of Kawasaki disease cases by age group per month. A: <6 months; B: 6 to <12 months; C: 1 to <5 years; and D: ⩾ 5 years.
Laboratory findings
Blood tests showed an elevated white blood cell and neutrophil count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) level. Patients with >10 days of illness exhibited lower levels of hemoglobin, aspartate aminotransferase, alanine aminotransferase and higher leukocyte count, platelet count, and ESR (Table 2).
Laboratory findings in children with Kawasaki disease.
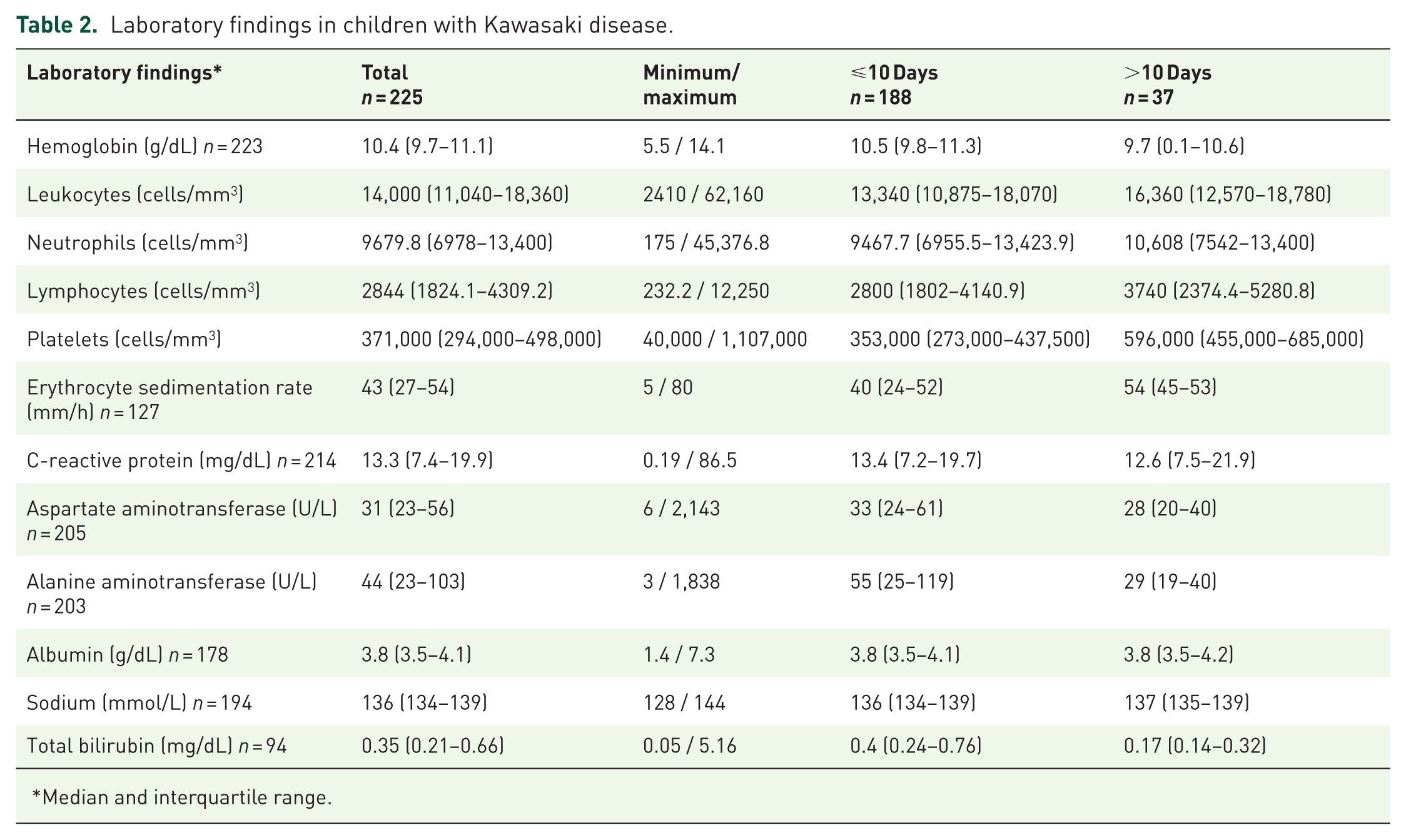
Median and interquartile range.
Treatment characteristics and complications
The treatment characteristics and complication in the affected children are shown in Table 3. Two patients (0.9%) were admitted to the ICU: one for hypotension (9 months) and one for suspected staphylococcal shock syndrome (5.1 year). None of the patients died during hospitalization.
Treatment and complications of children with Kawasaki disease.
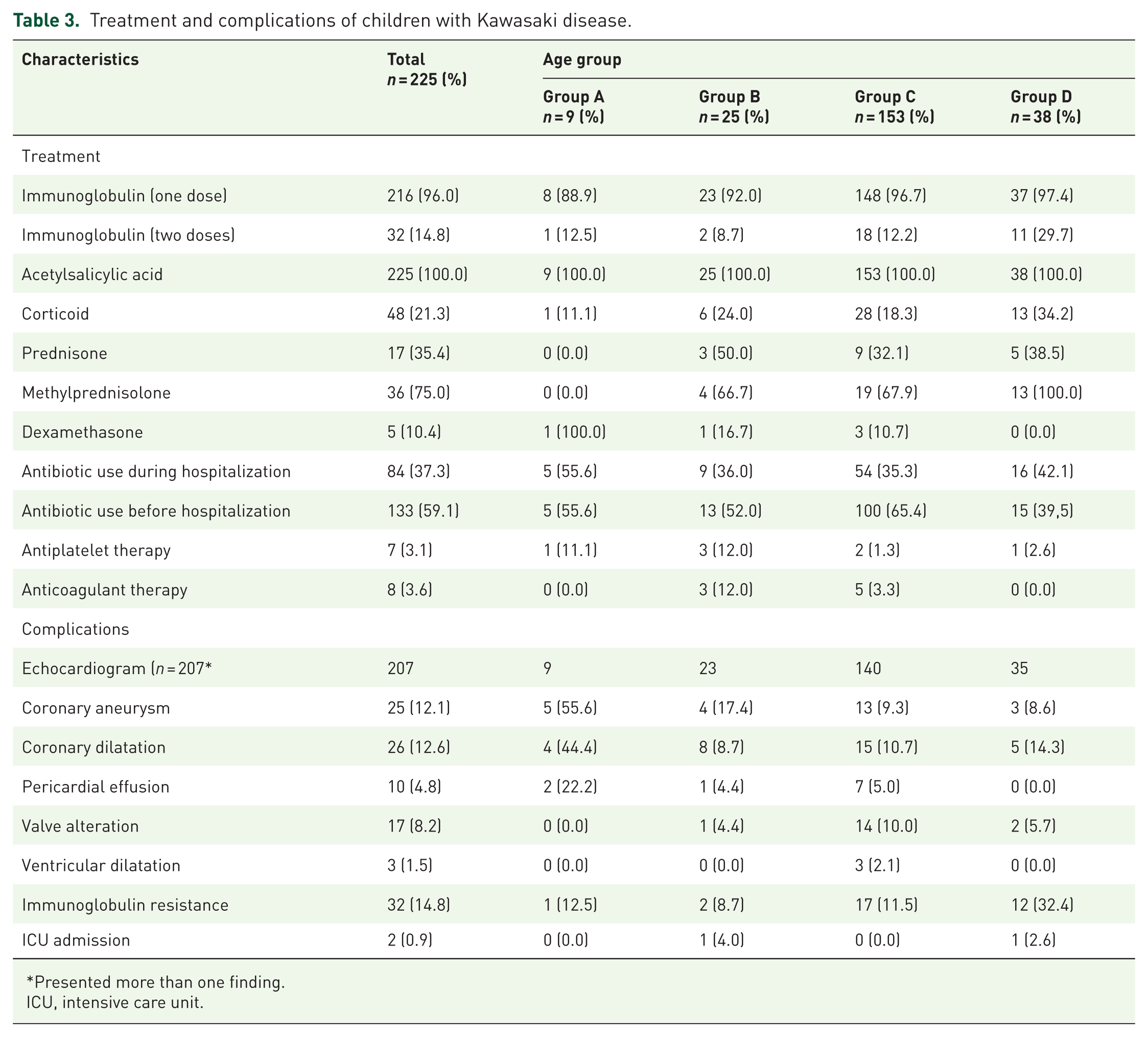
Presented more than one finding.
ICU, intensive care unit.
Discussion
In our study of Peruvian children, mucocutaneous symptoms and the use of immunoglobulins were similar to those reported in other studies with different populations.5,9,10,16 We also observed that the frequencies of coronary aneurysms and immunoglobulin resistance varied with age.
In Peru, KD is considered a rare orphan disease 18 because of its low frequency of presentation and high risk of cardiac complications if not diagnosed and treated promptly. In our study, the majority of cases occurred in children aged 1–5 years, with a median age of 2.3 years, which is comparable with reports from other Latin American centers (2.1 years), 5 Brazil (2.9 years), 16 Panama (2.4 years), 19 and Chile, where this age group represents 60% of all cases. 20 Therefore, the age at presentation is important for diagnostic suspicion in children with persistent febrile syndrome associated with mucocutaneous lesions.2,21
In our study, a diagnosis of KD was made every month. Seasonality has been noted in previous studies: in the Northern Hemisphere, the frequency is greater between January and March, whereas in tropical and Southern Hemisphere countries, such as Peru, the frequency is higher between May and June. 22 This timeframe was similar to that in our study, with the peak of cases beginning in April and extending through July. During this season, Peru experiences a surge in respiratory infections. This could be related to cases of KD, as evidenced in Chile. 23 However, further studies are needed to corroborate this. A recent study in France estimated that approximately 35% of KD cases can be attributed to seasonal infections, 24 suggesting that other triggers, including environmental factors, may also contribute to its presentation.4,10
Diagnosis was made after 10 days in 16% of the patients, with a higher frequency in children aged <6 months. This trend was also observed in a Latin American study with a representative sample 5 and in a study in Brazil, where the average time to immunoglobulin initiation was 10 days. 17
The delayed diagnosis of KD is explained by the fact that its symptoms vary and can initially be confused with exanthematous skin diseases and viral or bacterial infections.5,8 Therefore, strengthening knowledge about this disease is important for timely diagnosis. Currently, there is no definitive diagnostic test for KD; diagnosis relies on clinical criteria and, in some cases, supportive laboratory findings.2,21
Consistent with other studies, mucocutaneous manifestations were the most common clinical findings in our study,5,7 but the frequency of cervical lymphadenopathy (CL) increased with advancing age. One study noted that CL presents at the age of 3–6.6 years as an initial manifestation of KD. 25 In another study, CL predominated in children of intermediate age (median 3.3 years), and elevated inflammatory markers and unique differentially abundant proteins may define the KD subgroup. 10
The pathophysiological mechanism underlying this finding remains unclear, and further studies are required to analyze this in depth. Studies should also assess whether age influences the onset of CL in KD or whether CL is detected because it is more noticeable during clinical examination, as in children aged >2 years, the frequency of palpable CL is approximately 80%. 26
Respiratory symptoms were reported in one-third of the patients. A study of North American children with KD reported 50% of respiratory symptoms at diagnosis, with the most frequently identified respiratory viruses being rhinovirus/enterovirus, human metapneumovirus, respiratory syncytial virus, and adenovirus. 27 Despite their high frequency, viral infections do not appear to influence complications such as admission to the pediatric ICU, immunoglobulin resistance, or coronary aneurysms. 27
Similar to previous studies, approximately 30% of the patients presented with gastrointestinal symptoms.9,27 This feature was helpful for the clinical differentiation of patients with multisystem inflammatory syndromes during the pandemic.28,29 Although induration of the BCG vaccination scar has been observed less frequently, some reports suggest that this sign supports the diagnosis.15,16
KD is characterized by an elevation in inflammatory markers2,5,21; however, during progression, some differences may emerge. During the acute phase, increased leukocyte and neutrophil counts, elevated ESR and CRP levels, and decreased hemoglobin levels are typically observed. In the subacute phase, thrombocytosis and lymphocytosis become more prominent, 17 a pattern consistent with our findings.
First-line treatments most commonly included immunoglobulin and acetylsalicylic acid administration. In addition, patients with immunoglobulin resistance required a second dose of immunoglobulins and corticosteroids. These treatment regimens are supported by various scientific organizations studying this disease.21,30,31 Immunoglobulins decrease the incidence of coronary aneurysms, 32 whereas acetylsalicylic acid has anti-inflammatory and antiplatelet effects. 21 Corticosteroids as adjuvant therapy decrease the incidence of coronary aneurysms, and their use is suggested in individuals at a high risk of resistance or coronary aneurysms.21,33
Antibiotics were used in one-third of the population, a lower frequency than that reported in a multicenter study in Latin American centers. 5 KD is a part of the differential diagnosis of persistent febrile syndromes, and because of the risk of bacterial infection, initial antibiotic use is common. The hospitals included in this study were national/regional referral centers in Peru; thus, their health personnel were aware of KD. This could explain why antibiotics were discontinued upon the suspicion and diagnosis of the disease.
Cardiac involvement remains one of the most serious complications of KD. In this study, coronary aneurysms were observed in 12% of patients. Other studies in different populations have reported frequencies >20%.5,34 In Latin American countries, the frequency of aneurysms varies: Colombia, 20% 35 ; Chile, 9.4% 36 ; and Argentina, 15.5%. 37 Another study in Brazil found that the frequency of aneurysms was higher in children under 1 year (52.2%) and over 4 years (33.7%), 16 a similar trend was observed in our study (Table 3). This complication was more common in younger patients, particularly in those aged 6 months. This was previously reported in a study on KD subgroups, and according to other studies, this age group is the most commonly characterized.9,10,16
Immunoglobulin resistance was observed in 14% of the cases, similar to a Latin American study (11%; more common in patients aged >5 years), 5 Brazil 11.4% 16 and Argentina 20.2%. 37 Resistance is common in Chinese children aged <1 year and >5 years 9 and in Brazilian children aged <11 years. 17 We also observed that children older than 5 years had greater resistance to immunoglobulin; a similar result was observed in Chile. 36 The mechanism is not yet precise, but a proteomic analysis of Kawasaki disease subgroups found that older children have a higher risk of resistance, and this could be related to liver damage. 10 Another study in Brazil found no differences in resistance comparing three age groups. 17
The mechanism underlying this resistance remains unclear. However, it is suggested that leukocyte-platelet and monocyte-platelet aggregate complexes are produced due to the multisystemic symptoms of KD, which perpetuates inflammation and endothelial damage, especially at the coronary level.38,39 This finding explains why children with resistance are at a higher risk of coronary aneurysms.2,21 Although the participating institutions had experience in diagnosing and managing KD, there were likely differences in immunoglobulin doses and timing, because this expensive drug requires authorization for use. These factors could influence resistance, in addition to the patients’ genetic characteristics, such as polymorphisms in the Fc gamma receptor. 15 We were unable to investigate these factors in this study.
Limitations
This study has several limitations. This retrospective study was susceptible to information bias, particularly regarding the clinical symptoms reported by caregivers. Nonetheless, the risk of bias was considered low, given that the participating institutions were referral centers with experienced staff and access to standard treatment protocols. Similarly, our objective was to describe the characteristics of KD in Peru and understand the diagnosis and management in the hospitals evaluated. Therefore, we did not perform any statistical tests. In addition, this study focused on in-hospital data and did not assess long-term outcomes. Future studies should evaluate patient follow-up, particularly for aneurysm regression and recurrence.
The major strength of this study was that it included the largest number of KD cases reported to date in Peru. This method incorporates data from both the Ministry of Health and the Social Security System, enhancing representativeness despite the absence of a formal sample size estimation.12,13 Unlike previous Peruvian studies,12,13 this analysis stratified the data by age, providing insights into age-related differences in clinical presentation and complications. This study has implications for national guidelines regarding the management of this orphan disease in Peru as it demonstrates how a high-cost drug (immunoglobulin) is used as a standard treatment in healthcare institutions, as recommended by international organizations that study this disease.21,30,31 In future clinical practice, our results reinforce the recent AHA recommendations to intensify anti-inflammatory treatment in younger patients because of their elevated risk of coronary aneurysms. 21 This recommendation may be useful in countries with limited access to cardiac imaging services. Our results also emphasize the importance of a thorough history and physical examination, as some patients may be diagnosed late due to a disease that mimics other infectious diseases.
Conclusion
Mucocutaneous symptoms are common in Peruvian children with KD. The distributions of coronary aneurysms and immunoglobulin resistance differ with age. Management strategies were consistent with international recommendations. Future prospective studies are recommended to assess the long-term outcomes, particularly in patients with cardiovascular complications at the time of diagnosis.
Supplemental Material
sj-docx-1-trd-10.1177_26330040251404520 – Supplemental material for Clinical characteristics, treatments, and complications of Kawasaki disease in Peruvian children: a retrospective observational study
Supplemental material, sj-docx-1-trd-10.1177_26330040251404520 for Clinical characteristics, treatments, and complications of Kawasaki disease in Peruvian children: a retrospective observational study by Noé Atamari-Anahui, Giancarlo Alvarado-Gamarra, Nadin Conto-Palomino, Stephanie Cabello-Coca, Jessica La Torre Torreblanca, Danny Asparrin Ramos, María Fernanda Rosado Rullier, Olguita del Aguila and Jorge Candela-Herrera in Therapeutic Advances in Rare Disease
Footnotes
Acknowledgements
None.
Declarations
Availability of data and materials
The data and materials used in this study were obtained from medical records. Further information regarding this research can be obtained by contacting the authors.
Supplemental material
Supplemental material for this article is available online.
*
This reference indicates in Supplementary Material 2.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.