
Abstract
Objectives
The treatments of limbic and other autoimmune encephalitis include immunosuppression, symptomatic treatment, and in the case of paraneoplastic syndromes, appropriate therapy for underlying neoplasms. When immunotherapy is considered, intravenous immunoglobulin is one option for treatment, either alone or in combination with corticosteroids. To date, however, evidence for the use of intravenous immunoglobulin in this context comes from case series/expert reviews as no controlled trials have been performed. We aimed to analyse the NHS England Database of intravenous immunoglobulin usage, which was designed to log use and guide procurement, to explore usage and therapeutic effect of intravenous immunoglobulin in autoimmune encephalitis in England.
Design
We conducted a retrospective audit and review of the NHS England Database on intravenous immunoglobulin use.
Setting
NHS England Database of intravenous immunoglobulin use which covers secondary and tertiary care prescribing and use of intravenous immunoglobulin for all patients in hospitals in England.
Participants
Hospital in-patients with confirmed or suspected autoimmune/limbic encephalitis between September 2010 and January 2017.
Results
A total of 625 patients who were 18 years of age or older were treated with intravenous immunoglobulin for autoimmune encephalitis, of whom 398 were determined as having 'highly likely' or 'definite' autoimmune/limbic encephalitis. Ninety-six percent were treated with a single course of intravenous immunoglobulin. The availability and accuracy of reporting of outcomes was very poor, with complete data only available in 27% of all cases.
Conclusions
This is the first review of data from this unique national database. Whilst there was evidence for clinical improvement in many cases of patients treated with intravenous immunoglobulin, the quality of outcome data was generally inadequate. Methods to improve quality, accuracy and completeness of reporting are crucial to maximise the potential value of this resource as an auditing tool.
Introduction
Autoimmune encephalitis is a neuropsychiatric condition usually involving subacute onset of amnesia, behavioural change and seizures. Some cases are paraneoplastic, secondary to an immune reaction to a remote tumour, and some have no identifiable tumour. Many cases are likely antibody-mediated. The majority of antibodies are directed against neuronal cell surface proteins and are likely causative. 1 The commonest neuronal cell surface proteins include the N-methyl, D-aspartate receptor (NMDAR), LGI1 and the GABAB-receptor. First line immunotherapies for these conditions include corticosteroids, intravenous immunoglobulin or both. These are usually more effective in autoimmune encephalitis associated with neuronal cell surface proteins.1–6 Plasma exchange or immunoadsorption may be useful treatments, but in many centres their use is restricted as a second-line agent. 7 In the absence of randomised controlled trials – which are logistically difficult to carry out in these recently defined conditions – recommendations for treatment come from observational studies and expert consensus.
Neurological indications account for over 40% of the total usage of intravenous immunoglobulin. 8 In 2015, approximately 4.2 million grams of intravenous immunoglobulin was used to treat various medical conditions approved in the Department of Health Guidelines. Less than 5% of this was used to treat autoimmune encephalitis, classified as a ‘grey’ indication. 9 The NHS England Database of intravenous immunoglobulin usage provides a unique resource to investigate the use of intravenous immunoglobulin across the UK. Considering intravenous immunoglobulin has relatively limited availability depending on indication, and it costs approximately £5040 for a five-day course in a 70 kg patient, the database was established to attempt to track intravenous immunoglobulin use for various conditions across the NHS for contracting and procurement purposes. It was later modified to include ‘Outcome’ data to monitor appropriate use and potentially serious side effects including thromboembolism and haemolytic anaemia. However, this was not its initial purpose or design.
Using this database, we aimed to assess outcomes in cases of autoimmune encephalitis and the proportion of patients who demonstrated favourable outcomes. We also aimed to assess completeness and accuracy of data entry by the medical teams on application for approval of use of intravenous immunoglobulin in these cases in terms of diagnosis and longitudinal outcome measures.
Methods
Retrospective, observational, pseudo-anonymised data were extrapolated from the NHS National Immunoglobulin Database. 8 This database contains, amongst others, the following relevant fields which we extracted: ‘Diagnosis Confidence’; ‘plasma exchange’; ‘Outcome’; ‘Outcome Result’; ‘Condition Improved’; ‘Comments’. We applied the search terms ‘encephalitis’; ‘autoimmune encephalitis’; ‘limbic encephalitis’; ‘antibody-mediated encephalitis’; ‘encephalopathy’. We also searched for cases classified as ‘other’ because some cases of defined antibody-mediated encephalitis or encephalopathy were misclassified by ‘freetext’ within this category. We extracted the data and performed both qualitative and, where possible, quantitative analyses.
This was considered an audit of use with pseudo-anonymised data not specifically requiring research ethics committee approval prior to commencement.
Results
Between September 2010 and January 2017, a total of 625 patients (328 female) aged between 18 and 102 were identified as fulfilling our search criteria and having been treated with intravenous immunoglobulin. Diagnoses identified using our search terms included: ‘likely encephalitis’; ‘limbic encephalitis’; ‘autoimmune encephalitis’; ‘autoimmune limbic encephalitis’; ‘anti-NMDA encephalitis’; ‘anti-GAD encephalitis’; ‘anti-VGKC encephalitis’; ‘encephalopathy’. Considering a likely autoimmune aetiology, 193 cases were classified in the ‘Diagnostic Confidence’ category as ‘Definite’, 205 were classified as ‘Highly likely’, 77 as ‘possible’ and 150 did not have information available (field left blank). The data recorded in this field were assumed to be the degree of diagnostic certainty of the treating clinicians. However, no actual definitions of definite, probable or possible disease were provided in the database for these terms.
Plasma exchange use in patient cohort.

Examples of outcome measures used in database.

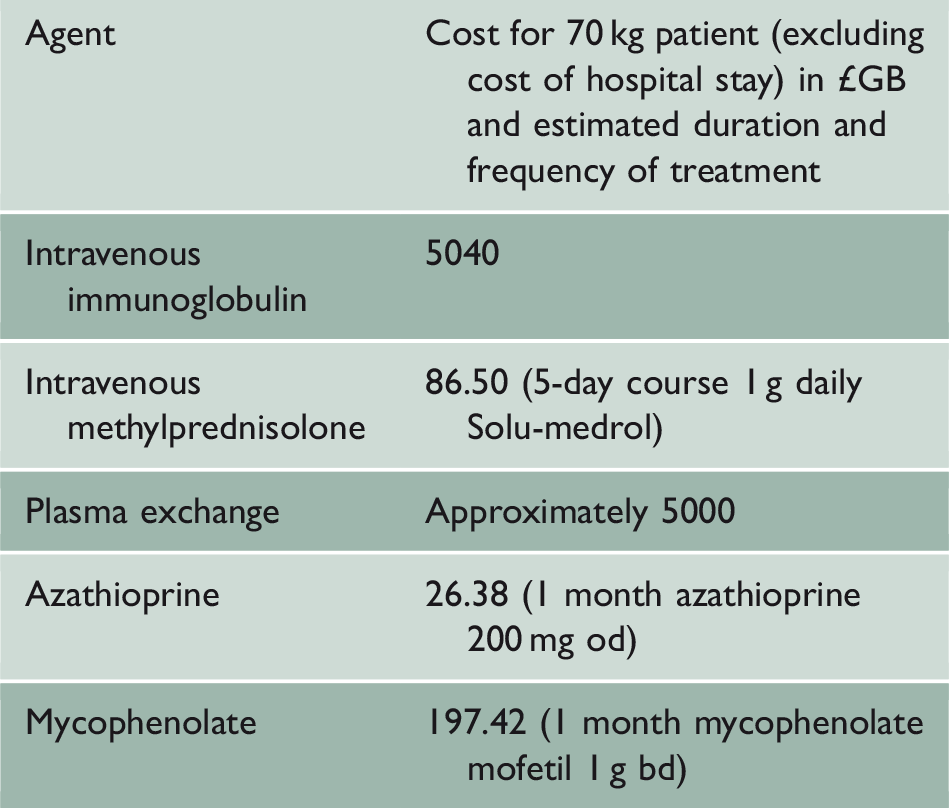
Illustration of comparative cost of a course of treatment in acute AE.
Forty-three patients had assessments at one time-point only. The remainder had > 1 assessment documented, but at different time-points and in many cases the time-points were not clear. Three patients simply had a drug dosage inserted as an outcome measure. Three patients had ‘imaging’ inserted as outcome data, although only one imaging report was quoted. Twenty-nine patients had ‘seizures’ recorded as an outcome, but with incomplete reporting on the outcome result. Twenty-eight had either no improvement or worsening of their outcome result entered. However, 58 had documented improvement in symptoms, including measures of improvement in mental status or reduction/control of seizures or reduction in antibody titres. The remainder had blank fields, incomplete, unclear or uninterpretable data entries.
Discussion
intravenous immunoglobulin is a relatively scarce and certainly expensive resource, accounting for approximately 0.15% of the whole NHS budget, and it is vital that it is used appropriately. Compared to other immunosuppressive therapies intravenous immunoglobulin is expensive (Table 3), but in combination with steroids can be rapidly effective and curative, returning patients to normal functions. The drug cost takes no account of rapid discharge and return to society contributions which intravenous immunoglobulin can facilitate. The UK centralised database is an essential and complete record of intravenous immunoglobulin prescribing throughout the NHS, providing commissioners, contracting agencies, regulatory bodies and researchers data on national and regional usage, and a breakdown of its use by condition and subspecialty. 8 The database is mature, having been in use for over six years. The database should provide a means of estimating benefit to patients through the measurement of longitudinal outcome measures. However, as this review demonstrates, the quality of data – and information about outcomes in particular – is inconsistently collected at best, and for the most part extremely poor.
The aim of this audit was to assess retrospectively the NHS England data collected for one intravenous immunoglobulin-indication. The objectives were many, including: assessing the frequency of autoimmune encephalitis treated with intravenous immunoglobulin, the treatment patterns and parallel therapies used, the outcomes of treatment (both absolute outcomes and the range of measures used) and the presentation of data to NHS England Commissioners to indicate the frequency of disease and intravenous immunoglobulin response.
The field of neuronal cell surface proteins has moved on in recent times, and rationalisation of tests – for example using CSF NMDAR-antibody levels, or LGI1 and CASPR2 testing in preference to the much less specific VGKC-complex assay1–4 – will help more accurately guide intravenous immunoglobulin usage. However, abolition of an antibody titre seldom occurs even though the patient recovers and so this is not an absolute outcome to measure.
In many respects, our audit produced useful outcomes. We were able to extrapolate an approximate incidence of autoimmune encephalitis of 1/million per antibody, which compares with previous estimates of 1.7/million. 10 In cases where outcome data were available (27%), intravenous immunoglobulin was shown to be effective in 39%. Very few patients are registered on the database as deceased and this probably reflects better treatment in recent years compared to before they were widely recognised, with a higher mortality among untreated patients. 11 Another explanation is that patients who died may not have been recorded in the database at all.
However, a striking feature was the frequency of poor and incomplete data entry into the database across all measures. There are several potential reasons for this. Firstly, the database was established principally to determine usage (both volume and by institution) to pre-empt and avoid shortages and potential patient harm, rather than to collect outcome data properly. The clinical utility of this database is determined by the quality of the data entered, which requires the treating physicians to provide data prospectively and after treatment for outcomes. There is little or no incentive to enter outcome data when usage is not repeated, i.e. once patients have recovered, died or moved on to other treatment. Often multiple treatments are used in parallel or serially and assessing the effect of intravenous immunoglobulin alone is difficult, not least if these co-treatments are not recorded.
The data are then added by pharmacists who have little medical or interpretative knowledge of a complex subject. No specific funds have been provided to enter the data at a pharmacy level although a small financial pharmacy cost is theoretically built into service level agreements. Data are entered by pharmacists. No medical portal is provided. And although free text entry is discouraged with drop down pre-filled options, the ‘other’ category was frequently used. Data entry is generally non-standardised with variable requirements and acceptability in terms of forms being granted positive review for processing. There were a very wide variety of outcome measures used, making results, even when recorded, not always comparable.
There are additional limitations to the study. As a retrospective audit, we were restricted to use pseudo-anonymised data from the database without access to patient level information or any ability to interrogate notes for outcomes other than in our own centre. The nature of autoimmune encephalitis means that intravenous immunoglobulin is often prescribed in one setting, with ongoing management provided elsewhere. And the limitations of the database when recording outcomes for autoimmune encephalitis do not necessarily reflect those in other conditions, where more standardised pathways to prescription and monitoring may be available.
The government are very keen on amassing statistics. They collect them, add them, raise them to the nth power, take the cube root and prepare wonderful diagrams. But you must never forget that every one of these figures comes in the first instance from the village watchman, who just puts down what he damn pleases.
Examples of suggested clinical outcomes and measures collected depending on the underlying phenotype.
Footnotes
Declarations
Funding
None declared.
Ethics approval
This was considered an audit of use with pseudo-anonymised data not specifically requiring research ethics committee approval prior to commencement.
Guarantor
MPL
Contributorship
All named collaborators qualify for authorship based on study design; collection, analysis and interpretation of data; manuscript writing and critical revision of the manuscript for important intellectual content.
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Heather Angus-Leppan.