
Abstract
Introduction:
Disease trajectories are often uncertain among individuals living with mucopolysaccharidoses (MPS) due to the progressive nature of the illness and the goal of care. This study investigated the impact on caregivers and care providers of children and adults living with MPS.
Methods:
The study used a cross-sectional design and a convenience sampling strategy which involved two sequential study components. The stage 1 quantitative component included three validated scales: the abbreviated World Health Organization Quality of Life (WHOQOL-BREF), the Paediatric Inventory for Parents (PIP) and the 14-item Resilience Scale (RS-14). The stage 2 qualitative component consisted of two focus groups with healthcare professionals (HCPs) (n = 9) working with children and adults living with MPS across three clinical sites in Ireland. Data were collected between November 2017 and July 2019.
Results:
A total of 31 parents identified as caregivers participated in this study. The mean quality of life (QoL) score was 93.81, indicating a significantly high QoL. The PIP frequency total mean was 102.74 and difficulty mean 104.94. The mean score for the RS-14 was notably high, 81.42 out of a maximum of 98. The majority of the results showed high levels of concern for the future, with just under 50% finding themselves very often feeling scared that their child’s condition will deteriorate or that their child will die and finding these thoughts very difficult. The healthcare professionals’ (HCPs) perceptions were focused on the complexity of MPS, coping strategies, managing expectations and support services.
Conclusion:
The overall findings of the study reinforced the need for sustained and enhanced psychological support to ensure both families of children and adults living with MPS and the HCPs are supported in the continued delivery of quality patient care and outcomes. Subjective and objective measures from family caregivers and HCPs yield results that can decrease stress and improve psychological support.
Plain language summary
Mucopolysaccharidoses (MPS) is a group of one of the many rare inherited metabolic disorders that come under category three of life-limiting conditions. Children born with this genetic condition show no change at birth, but effects start to show in subsequent years as it is a progressive disease. The severity of the condition varies according to the specific type, ranging from very mild symptoms to, in most cases, multisystemic, restricted growth or mental and physical disabilities. Recent developments in treatments for some forms of MPS have dramatically changed the quality of life (QoL) for patients. Other forms of treatment are currently under investigation and development. This study aimed to provide a detailed and reliable evidence base on the impact of caregiving for patients living with MPS on family caregivers and healthcare providers. Paper questionnaires were completed by the family caregivers of children and adults living with MPS. These three questionnaires focused on measuring QoL, parental stress and anxiety, and resilience among these families. Two focus group interviews were carried out with healthcare professionals working with children and adults living with MPS across three clinical sites in Ireland.
A total of 31 parents completed the questionnaires in this study, indicating a significantly high QoL and notably high resilience. The majority of the parental stress results were related to concern for the future, with just half of the families finding themselves very often scared that their child’s condition will deteriorate or that their child will die and find these thoughts very difficult. The healthcare providers also spoke about the complexity of MPS, coping strategies, managing expectations and support services for the families of children and adults living with MPS. This study provided evidence for clinicians and policymakers to improve the availability of appropriate healthcare provisions for people living with MPS and their families.
Keywords
Introduction
The mucopolysaccharidoses (MPS) are a group of rare inherited lysosomal storage disorders, which are multisystemic progressive disorders.1–4 All of these MPS disorders are caused by the deficiency of one of the lysosomal enzymes involved in the degradation of glycosaminoglycans or impairments in the lysosomal transport system.1–6 The management of patients with MPS is primarily supportive, with treatment focused on signs and symptoms rather than addressing the underlying enzyme deficiency. 5 Haematopoietic stem cell transplantation (HSCT) is the standard of care for infantile Hurler syndrome [mucopolysaccharidosis type 1 (MPSI)], although associated with significant procedural risks. Enzyme replacement therapy has become available for a subset (MPSI, II, IV, VI and VII) with resultant improvement in some but not all aspects of the disease.1–4
Early access and significant input from a multidisciplinary team of specialised professionals are recommended for diagnosing, treating and managing patients with MPS, as these diseases are rare and progressive.1,2 These conditions fall under category three of life-limiting disorders in which there is a lack of curative treatment options. 7 The progressive nature of symptoms implies that many patients living with these rare diseases will require recurrent hospitalisations. The signs and symptoms associated with MPS may vary among different types of MPS disorder; 8 however, symptoms can also be similar to physical, psychosocial, emotional and spiritual symptoms, in keeping with other forms of life-limiting illness.9,10
Technological and treatment advancement has enabled many children diagnosed with MPS or other rare complex conditions that were once considered life-limiting, such as Hunter syndrome (MPSII) and Hurler syndrome, to live into adulthood.11,12 The family plays a central role in caring for their child living with MPS,9,10 regardless of age. There are a limited number of studies that have investigated the impact of parenting a child with MPS. These studies reported parents’ experience as devastating, with a heavy burden being placed on parents due to the child’s challenging behavioural and physical symptoms and the progressive nature of the condition itself.9,10,13,14 However, very little is known about the caregiving impact of the family caregivers of individuals living with MPS.
However, despite the phenotype of MPS, the families of children and adults living with MPS and related rare conditions often adapt well to medical diagnosis and ongoing care needs.9,10 The need to provide ongoing care and support for their child and the fact that this care will extend into adulthood 15 and the parents’ own later life can have a significant impact on their quality of life (QoL), resilience, employment, income and family finances, and mental and physical health.13–18 This may also lead parents to increased risk of family dysfunction, marital disruption, physical and psychological dysfunctions, and mental health conditions. 19 Numerous studies have reported that caring for an individual living with MPS can impact every dimension of the family’s life. Families gradually develop ways to incorporate MPS into their day-to-day life.9,10,13,14 However, some family caregivers cope more effectively in their new role as caregivers than others, being more resilient and better able to bounce back from adversity.11,12,20 The parental ability to maintain a positive attitude and remain proactive appeared central to the coping strategies adopted by parents of children with MPS in a reported study from the same context. 9 Resilience plays a pivotal role in addressing and overcoming the disease’s challenges and caregiving roles and responsibilities. A wide range of studies have determined how psychosocial support and continuing care services9,10 and respite care21,22 are integral to, and either directly or indirectly impact the well-being and QoL of caregivers of children or adults with complex needs. A recent study reported that caregivers, mainly mothers of patients with MPS, experience low QoL, with caregivers of patients with MPSII experiencing significantly low QoL. 14
Healthcare systems across the world have adopted the concept of family-centred and family-oriented care to maximise the well-being of patients and their families. 23 Clinical practice and the experience of parents can sometimes fall short of this theoretical ideal. There is evidence that healthcare professionals (HCPs) do not appear to pay sufficient attention to supporting the caregivers’ health and well-being, despite the vital role played by the family caregiver. 24
Since MPS is a chronic progressive condition, HCPs who witness patients’ pain and suffering and their family members may also experience pain and suffering themselves. 25 Healthcare providers caring for children or adults with complex or palliative conditions experience moral and ethical distress, leading to feelings of helplessness and anger. 25 When HCPs feel they can no longer help the terminally ill recover, they begin to experience a deep sense of sadness, ambivalence and helplessness.24–26 These feelings may quickly lead to burnout and increase turnover rates in hospital settings. 25 Many HCPs express discomfort at introducing the topic of prognosis, including limited life expectancy, and may withhold information or not disclose prognosis as a result.24,27,28 To date, HCPs caring for children and adults with MPS have not been allowed to describe their caring experience. To address the lack of formal research into the HCPs’ understanding of caring for these children with MPS, our study also investigated the impact of the HCPs’ perspective. Given the lack of current evidence, there is a need to make a specific plan in developing and promoting best practice in the care provision for both caregivers and care providers. Measures of resilience, QoL and parental stress and their perceptions of the caregiving demands are examined to capture a comprehensive picture of the caregiver experience. This multiple-method study investigated the impact of caring for children and adult with MPS from the perspectives of both caregivers and HCPs.
Aim and research objectives
The aim and objectives of the stage 1 quantitative phase were to investigate the impact of caring for children and adults living with MPS from parents’ and caregiver’s perspectives by addressing the following research objectives: (a) to evaluate the QoL of caregivers of patients with MPS; (b) to examine caregivers stress related to caring for a child or adult with MPS; (c) to identify the degree of individual resilience.
The stage 2 qualitative phase focused on the perspectives of those providing health services to children and adults with MPS and their families to address the following research objectives: (a) to explore healthcare providers’ perceptions of the services currently available to children and adults living with MPS and their families; (b) to explore the experience of HCPs caring for a child or adult living with MPS.
Ethics
Approval to conduct the study was obtained from the ethical committees of three hospitals in Ireland: Children’s University Hospital (17.007); Our Lady’s Children’s Hospital (GEN/547/17); Mater Misericordiae University Hospital (1/378/1923) and University College Dublin (LS-E-17-156-Somanadhan). Written informed consent was obtained from each of the participants prior to the conduct of the study.
Participants’ rights of anonymity and confidentiality were supported throughout this study by the use of anonymous surveys. These special cohort patient groups can be easily identifiable due to their rare medical condition. This created a unique challenge for the researcher regarding protection of the study participants’ internal confidentiality or deductive disclosure. 29 Therefore, the researcher was conscious to avoid identifying the participant information by carefully selecting anecdotal and specific alterations. For example, disclosing particular phenotypes of their child’s MPS condition and related information were omitted, and no identifying information about patients was collected via medical records.
Methods
The cross-sectional study employed a purposeful sampling strategy that involved two sequential study components. The quantitative study component included three validated scales that were entirely close-ended,25,30,31 described below, and the response categories developed following statistical data analysis. The qualitative study component consisted of two focus groups with HCPs working with children and adults living with metabolic disorders. This approach permits each strategy’s strengths to be combined in a complementary manner with each other’s strength. 26
Recruitment
A purposeful criterion-based sampling strategy was used to recruit eligible HCPs and families of children and adults living with MPS from the National Centre for Inherited Metabolic Disorders. Inclusion and exclusion criteria are highlighted in Figure 1.

Inclusion and exclusion criteria.
Data collection measures
Stage 1: quantitative method
The three questionnaires were distributed to parents or caregivers during three outpatient clinic visits at the country’s metabolic service. Although these measures are self-rating questionnaires that the individual can complete, a member of the research team was available to provide assistance where required. All the participants were informed that their responses would remain confidential. Cronbach’s coefficient alpha was used to calculate the items’ internal consistency coefficients included in the questionnaires.
The abbreviated World Health Organization Quality of Life (WHOQOL-BREF) 32 instrument comprises 26 items designed to measure participants’ QoL by investigating the perception of their physical health, psychological health, social relationships and environmental health. 31 This survey was developed from the WHOQOL 100 survey to be a more manageable, shorter evaluation of QoL. It is considered a reliable alternative to the WHOQOL 100; however, the social aspect of the questionnaire is considered to be less accurate. 28 This survey includes questions about the participants’ issues, any medical or mental health problems. The closer the total score is to 100 points, the better the QoL, lower scores denoting lower QoL. The WHOQOL-BREF 31 questionnaire, contains 2 items from the overall QOL and general health sections and 24 items of satisfaction divided into 4 domains: physical health with 7 items (DOM1), psychological health with 6 items (DOM2), social relationships with 3 items (DOM3) and environmental health with 8 items (DOM4) (Table 1). Four domains of the WHOQOL-BREF questionnaire were considered as dependent variables. The other data collected included sex, age, education years, marital status, employment type, income level (per month), job background, chronic disease existence and local residence as independent variables. 31 In this study, Cronbach’s coefficient alpha was applied to examine the internal consistency of the WHOQOL-BREF scale (26 items) and the 4 domains in it. Cronbach’s coefficient alpha of the WHOQOL-BREF survey ranged from 0.704 to 0.868 for all 26 questions. The values were physical health domain (0.835), psychological health domain (0.790), social relationship domain (0.868) and environmental health domain (0.704).
WHOQOL-BREF domains. 31
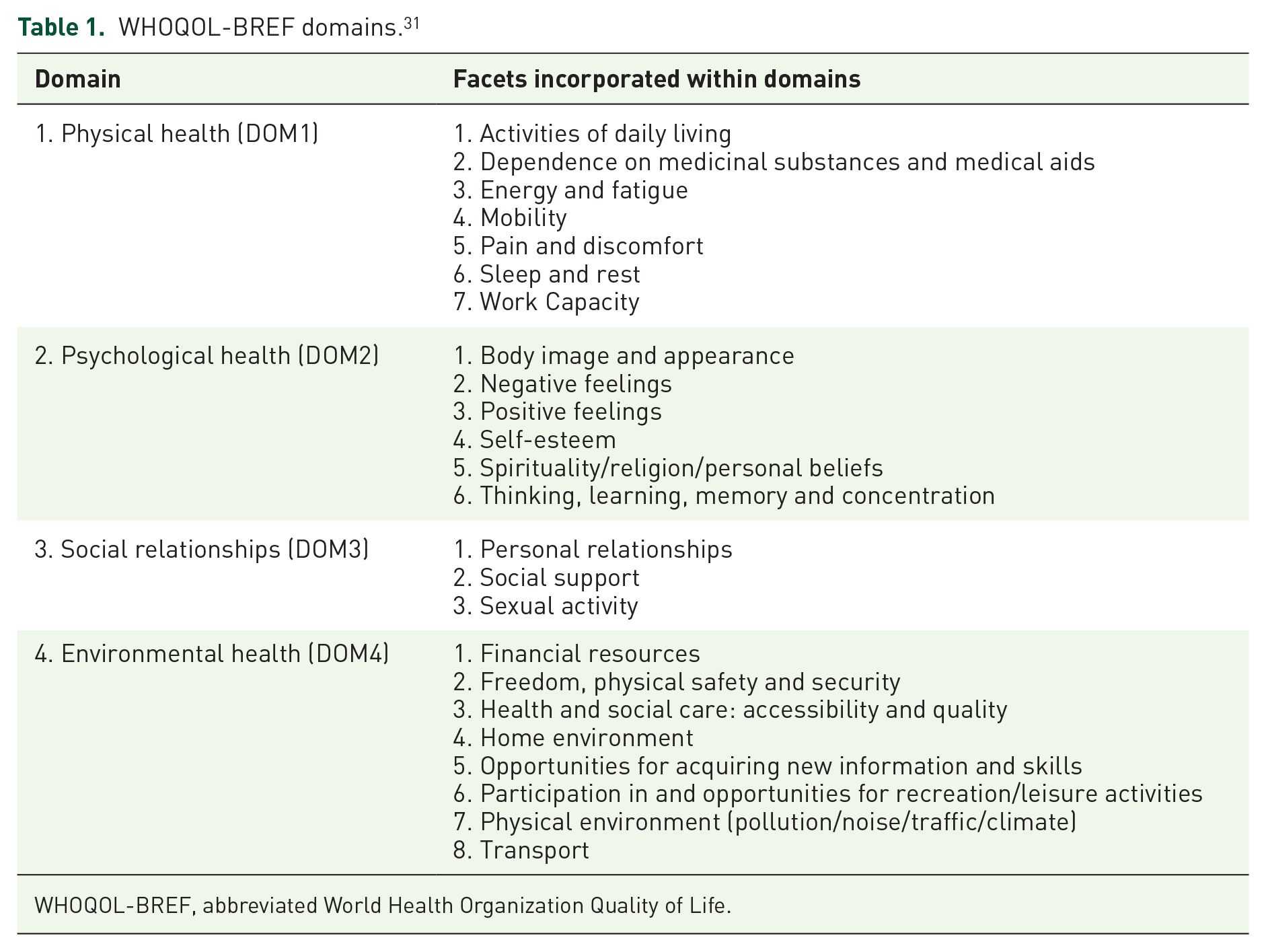
WHOQOL-BREF, abbreviated World Health Organization Quality of Life.
The Paediatric Inventory for Parents (PIP) 25 was designed to measure stress levels, specifically of parents of children with chronic illnesses or children requiring long-term care. 33 PIP was intended for a generic paediatric population but not limited to a specific diagnosis. 25 The instrument consists of 42 items split into four subscales: communication, emotional distress, medical care and role function. It takes two criteria into account, that is, frequency and difficulty. The response options consist of a 5-point scale ranging from ‘never’ (scores 1) to ‘very often’ (5) for frequency and from ‘not at all’ (1) to ‘extremely’ (5) for difficulty. Higher scorings indicate higher levels of distress.
The Resilience Scale 30 short form made up of 14-items (RS-14) 34 was used to identify the degree of individual resilience (personal competence and acceptance of self and life); a positive personality characteristic that enhances individual adaptation. The definition of resilience used for this survey is to sustain mental health/well-being in situations where an individual is faced with significant adversity or risk. 35 RS-14 is a self-completed questionnaire in which respondents were asked to state the degree to which they agree or disagree with each item on a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree).30,34 All the items are positively scored, and the minimum score on the 14-item scale is 14 while the maximum rating is 98.30,34
Stage 2: qualitative method
The purpose of this qualitative phase (stage 2) in this multiple-methods study was to explore and understand the HCPs experience of caring and the availability of appropriate healthcare provisions for patients and their families. Focus group interviews were used as the data collection method. This data collection mode offered respondents the opportunity to answer the questions posed by the researcher and discuss issues raised by their fellow participants. 36 Data were collected over 4 weeks between June 2019 and August 219 and transcribed verbatim. A semi-structured topic guide was developed from the findings explained from the stage 1 survey results.
Data analysis
Stage 1 quantitative survey data were analysed with the use of SPSS16 software. Descriptive analyses were conducted. The reliability of the WHOQOL-BREF domains, 31 PIP 25 and RS-14 was assessed using Cronbach’s coefficient alpha. A critical value of alpha of 0.70 and above was considered to be satisfactory evidence of the reliability/internal consistency of each of these instruments, with no further scale development needed. 37
Stage 2 qualitative focus group interviews were guided by the Lincoln and Guba 38 (pp. 294–301) framework for evaluating rigour and credibility as appropriate to this study. The study reflexivity was achieved by writing, analysing and reflecting, and keeping a reflective journal throughout the study.39,40 The qualitative thematic analysis checklist facilitated by Harvey and Land 36 (p. 286) was used to guide the data analysis process in the second phase of the study. The thematic analysis provided a flexible and valuable research tool to identify themes across a qualitative dataset,36,41 and the software NVivo12 assisted this analysis. A total of 4 themes and 16 corresponding subthemes emerged during thematic data analysis.
Results
Stage 1 quantitative methods
A total of 31 participants, all of whom were parents currently caring for children and adults living with MPS (MPSI, MPSII and MPSIV), completed the questionnaires. Of note, the birth prevalence of MPS per 100,000 live births was almost similar in most European countries, including Northern Ireland (4.0), Czech Republic (3.72), Estonia (4.05) and Germany (3.51). 42 The reported birth incidence of MPSI in Ireland was 1 in 26,206 births with a carrier frequency of 1 in 81, however, the incidence among Irish Travellers was 1 in 371 with a carrier frequency of 1 in 10, the highest recorded incidence worldwide. 43 The characteristics of the study population are shown in Table 2. Given the small sample (~75) nature of individuals living with MPS in Ireland, a convenience sampling strategy was used to recruit parents of children or adults (n = 31) with MPS who were seen at the outpatient MPS clinic in Ireland. Due to the study’s exploratory nature, the sample size needed was very subjective, therefore, no justification of the sample size was utilised. The sample was analysed both as a whole and divided into types of MPS. This cohort included carers of patients with MPSI, MPSII and MPSIV. The majority of family caregivers was represented from the MPSI cohorts. The MPSI cohorts comprised 55% (n = 17) female caregivers, and those were reported as mothers, and 19% (n = 6) male caregivers, and those were fathers. The MPSII cohorts were mothers (n = 2) and fathers (n = 1), and the MPSIV cohorts were mothers (n = 4) and fathers (n = 1); overall, in this study 26% (n = 8) were male (father) and 74% (n = 23) were female (mother) participants. The age of participants ranged from 25 years to 61 years, with a mean age of 43.14 years. Most participants finished their education after secondary school, with 19.4% finishing education at primary level and 29% going on to the third level. The majority (71%) of parents reported their status as married, with 6.5% single, 3.2% widows and 19.4% co-habiting. A small proportion of the sample was experiencing their own health difficulties at the time of the survey. One in 10 (9.7%) reported flare-up of a chronic illness, with a similar proportion (9.6%) reporting current mental health issues, short-term illness and/or a combination of the two. Breakdown of the sample is shown in Table 2.
Socio-demographic characteristics of the participants.
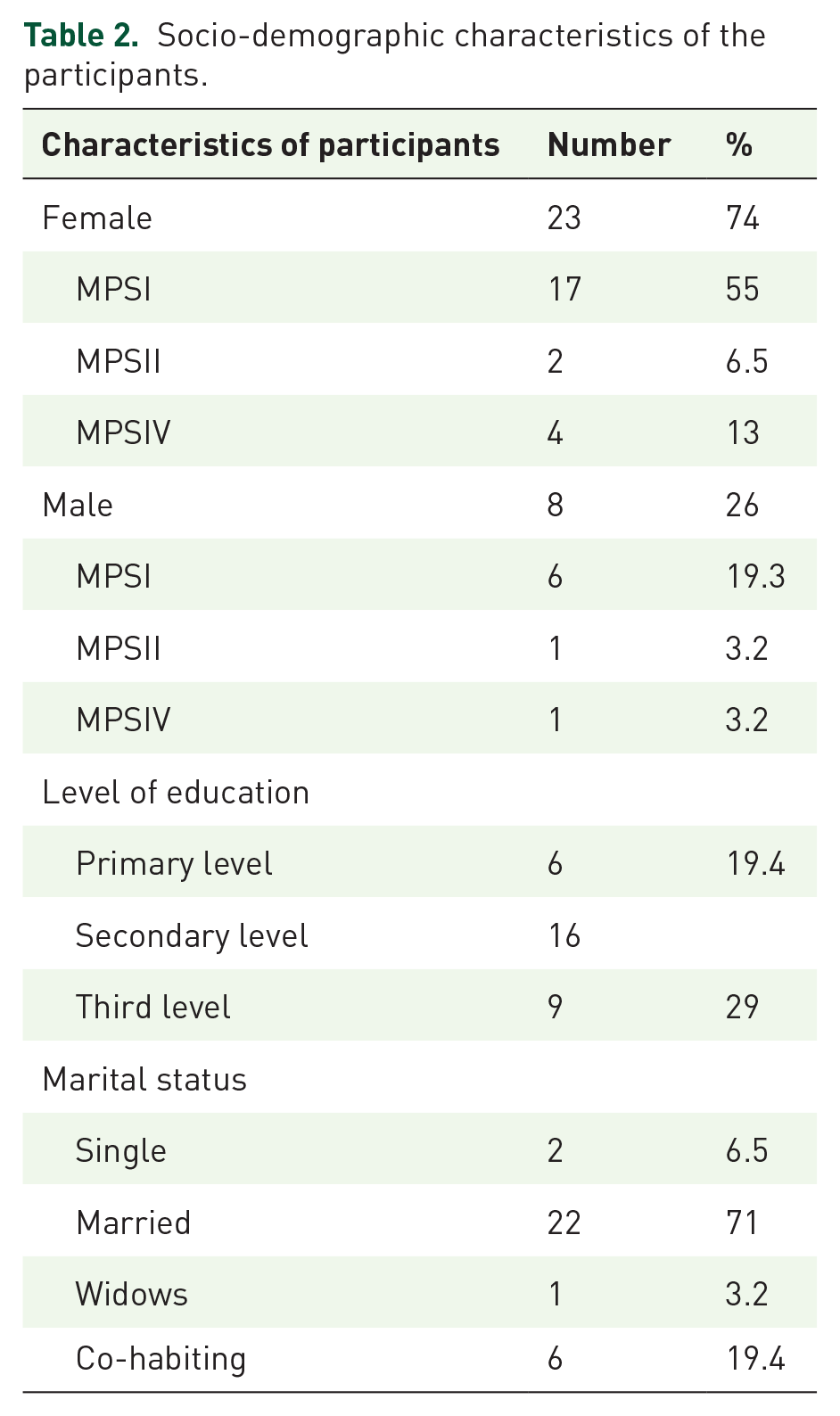
Table 3 shows the scores derived from the WHOQOL-BREF survey. In this study, among the four domains of WHOQOL-BREF, the highest mean satisfaction rating was found for DOM4 (Environmental health, mean = 30.55), implying good financial resources, freedom, living conditions place and access to health services. The second-highest score was applied to DOM1 (Physical health, mean = 28.35), implying the ability to perform good activities of daily living, less dependence on medicinal substances and medical aids, enough energy and mobility, less pain and discomfort, sufficient sleep and rest, and good work capacity. The third highest score was applied to DOM2 (Psychological health, mean = 23) and included life enjoyment, life to be meaningful, satisfaction of yourself and experience of negative feelings such as blue mood, despair, anxiety and depression. The lowest mean score was shown for DOM3 (Social relationships, mean = 11.09), indicating personal relationships, including sex life and lack of support from friends. Cronbach’s coefficient alpha for this survey ranged from 0.704 to 0.868.
Scores derived from the WHOQOL-BREF survey.
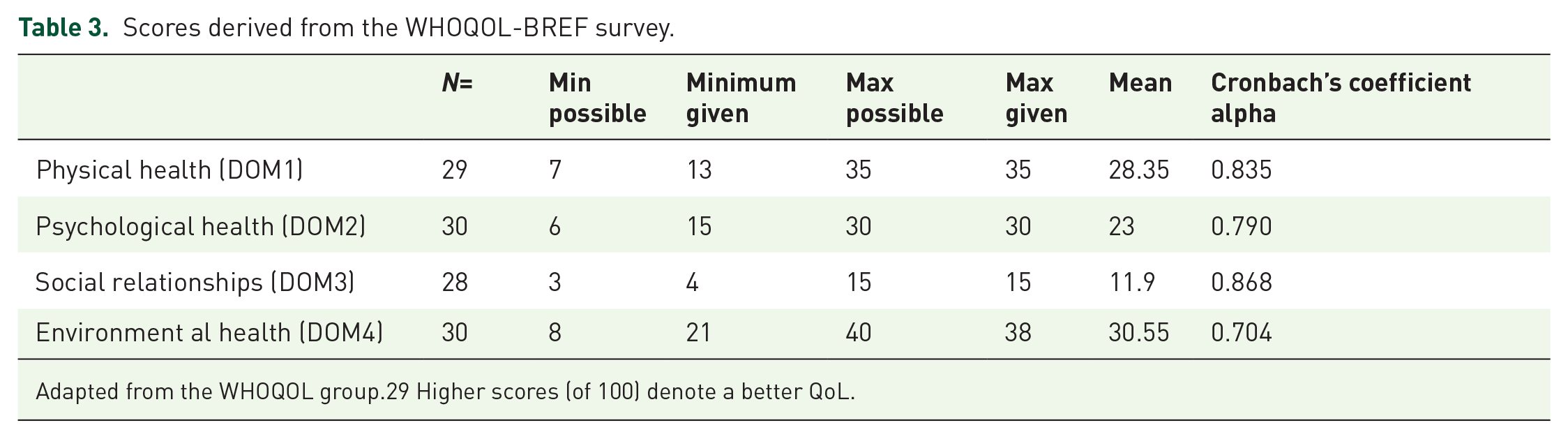
Adapted from the WHOQOL group.29 Higher scores (of 100) denote a better QoL.
The PIP 25 instrument consists of 42 items split into four subscales: communication, emotional distress, medical care and role function. Each subscale yields two scores, that is, frequency (whether the parent experiences these issues) and difficulty (how much of a problem this is for the parent). Table 4 summarises mean scores on the subscales and total scales used to assess paediatric parenting stress of the parent (n = 31), of which fathers (n = 8) and mothers (n = 23) completed this scale. The first domain, communication, scored a mean score for frequency of 19.87. However, the difficulty aspect of the domain had a mean score of 20.06. Medical care, the second domain, had a mean score of 20.81 and a difficulty mean of 18.97. The third domain regarding emotional distance gave a frequency score mean of 40.55 and a difficulty mean score of 43.29. The fourth domain related to role function and the mean score for frequency was 20.90 and 24.19 for difficulty. PIP’s internal consistency was examined by calculating Cronbach’s coefficient alpha for the total and four domain scale score for both frequency (0.69) and difficulty (0.90).
A summary of the PIP score subscale.

PIP, Paediatric Inventory for Parents.
RS-14 includes 14 statements. Participants respond to a scale ranging from 1 to 7, depending on how much they agree with the statement (1–3.5 corresponding to disagreement with the statement and 3.5–7 agreement). The minimum possible score for each question is 1, and the maximum is 7; the minimum score is 14 and the maximum is 98. The mean score overall was 81.42. An individual with a score of 82–98 was considered to have very high resilience tendencies, which applied to 51.7% of the sample. Around 32.2% of the sample scored between 64 and 81, rated as having high resilience tendencies. Less than a fifth of the sample (16.1%) was shown to have average resilience tendencies, scoring between 49 and 63. None of the participants scored below 57, indicating that there were no participants with low and very low resilience tendencies.
Cronbach’s coefficient alpha was calculated to determine the reliability of RS-14. A value of 0.913 was yielded, indicating that the RS reliability was good.
Stage 2 qualitative methods
A purposive sample of nine HCPs, working as part of the national metabolic service for paediatrics (n = 3) and the adult service (n = 6), participated in the focus group, which lasted for a minimum of 60–120 min. The focus group interviews were held at the respective clinical sites because they were proposed as convenient locations for the participants. The adult service focus group (FG1) comprised two consultants, one nurse, two specialist registrars and one junior medical officer. The paediatric service focus group (FG2) included one consultant, one nurse and one clinical psychologist. Data saturation occurred after the second focus group, therefore, further focus group discussion was not required from the research sites. The following codes are used with the data quotations: P = participants; M = letters assigned to represent male participants; W = letters assigned to represent female participants, for example, M1 = male participant 1, W1 = female participant, respectively. FG1 = focus group 1; FG2 = focus group 2. The details of the demographic characteristics of the participants are presented in Table 5.
Demographic characteristics of focus groups participants (n = 9).

The four main themes from the focus groups were: (a) multiplicity and complexity of MPS; (b) managing expectations; (c) support systems; (d) coping strategies.
Multiplicity and complexity of MPS
All the participants in FG1 and FG2 indicated the multiplicity and complexity of MPS, and how signs and symptoms associated with MPS fluctuate with typology. The quotes below suggest that participants were reflecting more on the organisational and systemic challenges of meeting the needs of patients and families, given that these needs are challenging, complex and specific to the individual patient or family.
“Well with this disorder . . ..your focus is all on the transplant and then they come back because they’re only seen for a year after that, and then they’re back with us. When it’s done, it’s done, but then they’re still left with a chronic illness although not fatal anymore they still have a lot of medical problems. So the complexities are probably in meeting those needs. So there are challenges around that. . .. The clinics have lots of appointments in one day, this reduces hospital visits, but they’re very difficult to arrange all the specialists on the day you need them. . . and the logistics of getting patients to everything is quite difficult.” (W1, FG2) “I guess just the complexity of the syndrome and how there are multiple aspects to consider. It’s just that when these patients come through the door, it’s not clear cut like Chronic obstructive pulmonary disease (COPD), that is sort of open and shut there is no factors or multiple systems involved. So you have to be aware of that and know who to direct their care to at relevant times”. (M3, FG1)
Managing expectations
Most of the participants expressed concerns related to managing individuals and a family’s expectations, particularly in relation to genetic services, the diagnostic process and expansion of the newborn screening programme.
“Let’s say with the Hurler case. . ., he/she receives a bone marrow transplant before the age of 2 so he never went on enzyme replacement therapy. Not all patients are lucky enough to receive that bone marrow transplant because they are diagnosed too late, and that can have a bearing on the outcome in the paediatric setting. There is a push now to expand newborn screening and to ensure MPS is included in the screening. This will definitely make a difference because if you get the diagnosis early in life and these therapies earlier on, there will be a significant–good outcome”. (M1, FG1) “The genetic system is very poorly funded, understaffed, and there’s a waiting list, but nobody has to pay unless they wanted to go privately, but they don’t have to. All families are told it’s available but a lot of them opt not to have us. The other side of it is if a mother is pregnant and wants to genetic counselling and they will give it to her first. I’m not surprised because there is a long wait. (M1, FG1)
Support systems
The majority of the respondents at the focus interviews highlighted the need for a structured support system in place for individuals living with MPS. They discussed the multisystemic nature of the illness and the need for a patient-focused approach to providing integrated care services. In Ireland the Progressing Disability Services is a national process to reorganise children’s disability services. The participant was reflecting on how these services will soon combine their staff to create new teams so that children will have equal access to support regardless of where they live or the nature of their disability.
I don’t know I think of change a lot with progressive diseases. . . somewhere like centre very well integrated in a physical disability you get all of your physical disability care needs catered for there and severe cohesive those kinds of systems but forgot to disabilities those systems, in theory, it more accessible service for more children than practice. “ think it’s all about integrated care pathways, that buzzword. The first thing is to get people aware of rare diseases and how common they can be. It’s implied by the term rare. . .. Health Service Executive (HSE) has a lot on their books and are not necessarily going to give money to rare conditions until they realise how common it is. So step one is increasing awareness and that stands for colleagues as well. Some of our colleagues are not as tuned into rare diseases as they could be. So I suppose we need to get the word out there about 1 in 10 of us could have a rare condition. (M1, FG1)
Coping strategies
Healthcare providers caring for children and adults with progressive conditions experience moral and ethical distress, and this can lead to feelings of helplessness and anger. 44 The focus group participants shared their experiences of dealing with stress in the workplace. They reported that there is no uniform structure or strategy in place to address this issue in the current educational or healthcare system.
“Traditionally medicine is terrible for this we don’t take care of each other that’s just the system. [unclear] I know sometimes have a buddy system, and that’s all well and good, but I think it’s very difficult. . . .It doesn’t really exist if you’re asking do we have a proper support structure, but maybe colleagues are nice to each other and have a chat around the coffee table”(M1, FG1) “I think it probably does a lot of informal support which works well if you’ve got a team at work together, but that is probably dependent on the team relationships so something formal alongside that might be helpful. . .” (W3, FG2) Its about recognising burnout and the old school mentality ritual humiliation has been almost knocked out. I think the support mechanism is almost a bit more established over in the UK. It’s there and the (name) here is starting to run workshops on burnout so things are on the agenda and people are starting to recognise that this is happening and the people are leaving the profession because they’re like this is too much. (M3, FG1)
In summary, the findings of the qualitative phase of the study highlighted HCPs’ perceptions of the services currently available to children and adults living with MPS and their families. They emphasised the need for an integrated health and social support system. The HCPs acknowledged that they do not seek the same expert aid as they would offer their patients. It was highlighted that there is a gap that exists in the healthcare service sector and educational settings regarding the assessment and management of stress and burnout among health and social care professionals.
Discussion
This study investigated the impact of caring for children and adults living with MPS from the perspectives of both family caregivers and HCPs. The concept of QoL has become increasingly recognised and valued over the last decade 45 and is directly linked to physical, mental, psychological and emotional well-being. The WHO defines the quality of life as a “broad-ranging concept affected in a complex way by the person’s physical health, psychological state, the level of independence, social relationships, personal beliefs and their relationship to salient features of their environment”. The overall mean QoL score of family caregivers of children and adults from the WHOQOL-BREF scale 31 was 93.81 on a 0–100 scale, where scores closer to 100 indicate better QoL. In this study, the caregivers of children and adults with MPS had significantly higher scores for all four specific domains. There was no statistical difference in the mean QoL score between family caregivers of children versus family caregivers of adults living with MPS.
A recent study based in Brazil 14 comprised 11 mothers (n = 11) of children with MPS, where few patients were attenuated and treated. The mean QoL score was 48.06, and in the specific WHOQOL-BREF domains, physical health scored a pooled mean of 56.03 points compared with a pooled mean score of 36.11 points in the social relationships domain where the lowest scores found. This study does not make it comparable with other tasks due to the patient populations’ nature and treatment.
The study by Vanz et al. 46 focused on adult caregivers (n = 24) of children and adolescents with osteogenesis imperfecta, a group of rare genetic disorders. This study also reported significantly low mean WHOQOL-BREF scores across all the specific domains, that is, 14.59 for the physical health domain, 13.80 for the psychological domain, 15.19 for the social relationships domain and 12.87 for the environmental domain. A recent qualitative study10,47 involving a similar participant cohort from Ireland noted that parents of children and young adults were living in an in-between status due to the range of uncertainties in relation to their children’s health and care. They made reference to “no man’s land” and “future is unknown”, in describing their world. Given that the present study took place in the same context, with the same socio-cultural and health service factors, the association between uncertainty/liminality and parental stress identified among this cohort was noted. 47
Paediatric parenting stress was referred to in this study as the stress experienced by parents of children with MPS by reference to (a) child health, (b) parental roles, responsibility and burden, and (c) psychological and behavioural response, and adaptation to illness. 25 The PIP questionnaire was designed to measure stress levels, specifically of parents of children with chronic diseases or children requiring long-term care. 33 It measures levels of stress through four domains; communication, medical care, emotional distance and role function. The family caregivers, (n = 31) mother, (n = 23) (father n = 8), reported the highest score on the emotional distress frequency (40.55) and emotional distress difficulty (43.29) scales. The lowest score was reported on medical care difficulty (18.97). A significant issue raised in this questionnaire were concerns related to medical decisions: 60% of caregivers rarely said or never made medical decisions, yet 40% reported not finding it difficult at all; 46.7% of caregivers stated they were not confused at all by medical information. The second-lowest reported score was on communication frequency (19.87).
The result of the PIP results revealed high levels of concern for the future, with 55% of caregivers regularly worrying about the future of their child’s condition and reported feeling helpless regarding the condition. They very often feel scared that their child’s condition will deteriorate or that their child will die and reported finding these thoughts very difficult. Around 66.7% of caregivers reported extreme levels of difficulty in dealing with this situation.
The association of female gender versus male gender paediatric parenting stress were examined in children with chronic illness.48,49,50 Studies found that mothers reported higher levels of paediatric parenting stress than fathers. Given that rationale, we examined parenting stress in relation to gender difference using normality tests, which demonstrated very little difference between the groups, and the data seem normally distributed; hence we have not carried out further inferential statistics. A recent study has also reported that the burden of care increases in fathers and decreases in mothers. 51 As the child grows, fathers assume more responsibility for the care of their child. To best support families of children with MPS and other rare and complex conditions, further research focused on comparing paediatric parenting stress in the fathers and mothers of young children with rare and complex illness to study the variation in this stress over time is warranted. More importantly, this finding suggests that PIP shows promise as a measure of disease-related parenting stress for caregivers of children and adults with MPS or rare diseases where none currently exists.
The quantitative analysis of RS-14 survey data confirmed that parents/caregivers reported high family resilience, with 57% having a score of 82–98, which is considered to represent significantly high resilience tendencies. Around 32.2% of the sample scored between 64 and 81, rated as having high resilience tendencies. Less than a fifth of the sample (16.1%) were shown to have average resilience tendencies, scoring between 49 and 63. None of the participants scored below 57, which eliminates low and very low resilience tendencies despite the time and how it differs in treated/untreated patients. These findings are consistent with a recent study, 10 which reported that parents of children and young adults with MPS maintained a positive attitude and remained proactive. These appeared to be central to the coping strategies they adopted in their day-to-day life. Families demonstrate higher resilience if they are able to maintain one or more of the four core family functions, including membership and family formation, economic support, nurturance, education and socialisation, and protection of vulnerable members. 51 The findings confirmed that resilience plays a pivotal role in addressing and overcoming disease and caregiving roles and responsibilities.
Most family caregivers represented from the MPSI cohorts from the MPSI paediatric clinic (aged from 0 to 16 years) had Hematopoietic stem cell transplantation (HSCT). The MPSI cohorts comprised 55% (n = 17) female caregivers, and those were reported as mothers, and 19% (n = 6) male caregivers, and those were fathers. MPS1 has the highest incidence among Irish Travellers, with a reported birth incidence of MPSI as 1 in 26,206 births, with a carrier frequency of 1 in 81. 52 The treatment and the positive aspects of Traveller culture such as community, family support and religiosity are reported in the All Ireland Traveller Health Study 53 and could be the reason for high resilience and reported good QoL among these cohorts. It is also important to consider the possible difficulties of participants expressing themselves and contemporary literacy and language issues, especially with the Traveller community members in this survey.
This study’s findings add to existing knowledge of supportive psychosocial needs for parents/family caregivers of children and adults living with MPS. Knowledge and educational gaps were identified between evidence and practice on how HCPs caring for children and adults are coping with stress. The majority of HCPs tend to use an informal conversation with peers as a model of coping strategy within the clinical settings. The importance of the multidisciplinary team and the professional support it offers was emphasised. The majority of HCPs emphasised a need for stress management programmes at the local hospital level and at the community level that could improve coping strategies for caregivers of children and adults with rare progressive illnesses like MPS and the care providers. With that in mind, coping strategies and stress management programmes can be considered in designing behavioural interventions for both cohorts.
Conclusion
This is the first study that examined the quality of life, parenting stress and resilience among families of children and adults living with MPS to the best of our knowledge. The study findings highlighted that in the majority of parents/family caregivers there was a significantly high QoL and resilience compared with other cohort studies. This study underlines the need to integrate both objective and subjective QoL measures to get a more realistic picture since the subjective QoL of a person is primarily invisible and, therefore, difficult to measure. 54 This study revealed that parents of children with MPS have above-average resilience. This may be accredited, in part, to the high level of social support that was reported. The major contributing factor to parenting stress identified among these family caregivers was their child’s uncertain future due to the progressive nature of the illness. While the uncertainty is primarily due to the nature of this disease, it is possible that more open discussion about long-term effects and prognoses, initiated by the healthcare team in their communication with the families, could reduce the uncertainty that these families face. The majority of the HCPs emphasised a need for stress management programmes at the local hospital level and also at the community level that could improve coping strategies for both caregivers of children and adults with a rare progressive illness like MPS and even for the care providers. This raises concern not only for the well-being of HCPs but also for the quality of patient care delivered in these settings. While it may not be entirely possible to prevent stress, depression and anxiety among HCPs, the relevant stakeholder needs to acknowledge the rising prevalence of psychological distress among HCPs so that necessary resilience strategies can be implemented to safeguard their psychological well-being and quality patient outcomes. Further research may benefit from longitudinal study designs with a more comprehensive set of demographics and personal and work-related factors to fully determine the predictors of negative mental states in different groups of HCPs who are working with children with rare progressive illnesses.
Limitations of the study
While this study represents an important finding in understanding the experiences of family caregivers and HCPs, several limitations must be considered when concluding the findings. The results and the associated conclusions are limited by the small sample of 31 family caregivers due to the rarity of this illness, and limited regarding ethnicity and socioeconomic status, even though the sample was drawn from the national metabolic centre. Beyond these limitations, this study’s findings indicated that there is merit in understanding and addressing how MPS as a rare disease influences parenting stress, anxiety, QoL and family functioning across the lifespan. A convenience sampling strategy was employed for the survey due to the rarity of this illness and the patient attenuated forms. The results of the study, therefore, cannot be generalised to the entire population. The analyses that provided descriptives for each type of MPS were not included as the numbers in MPSII and MPSIV were too small. We agreed that scores for the total sample should suffice. A larger sample and more appropriate study designs are required to identify the factors involved in disease severity and reported patient outcomes measures pretreatment and post-treatment to have an impact on QoL, stress level and resilience. Normality tests and graphs demonstrated little difference between total scores on the three psychosocial measures in terms of gender differences, differences based on three categories of education such as primary, secondary and third level, and marital status, and the data seemed normally distributed, hence we have not carried out further inferential statistics. A larger sample of HCPs who care for patients with MPS is required to measure HCP stress in the management of these patients using quantitative scales to understand the most stresses among these cohorts of HCPs. Thus, future investigations require a joint effort from all researchers in this field to enable a more reliable analysis of the cornerstones of caregivers’ and care providers’ QoL, resilience and stress and study variation over time.
Implications for policy and practice
This study’s findings highlight the need for more significant and diverse initiatives that could serve as indicators for the future understanding and development of policy and practice related to rare progressive illness like MPS. Improved communication training is necessary for professional staff, including how to communicate sensitive information and support parents’ needs at the time of diagnosis of MPS and other rare diseases. Education and training for HCPs will support their personal and professional development and help reduce vulnerability and stress in the workplace.
Implications for further research
Very little is known about families’ experience of living with and caring for children with rare, nonmalignant, genetic, life-limiting conditions, mostly inherited metabolic disorders. Further qualitative research into the rare, paediatric, life-limiting illness population that will guide suitable interventions to support the family and HCPs is important and topical. Further research is also recommended to explore the level of support each separate family member requires, including healthy siblings and grandparents, as well as investigating the needs of families for the long-term care of their child through adolescence to adulthood and the specific services required at these times. The findings confirmed that resilience plays a pivotal role in addressing and overcoming disease and caregiving roles and responsibilities. Further research is needed with family-focused resilience interventions to improve the mental health and well-being of families living with children and adults with MPS and other forms of rare diseases. These studies will offer evidence to enhance positive family functioning, supporting parental well-being and family functioning, and positive coping skills. This study also recommends investigating the use, challenges and opportunities for using patient-reported outcome measures specific to lysosomal storage disorders so that they can be incorporated into clinical practice.
Supplemental Material
sj-jpg-1-trd-10.1177_1049732320931430 – Supplemental material for IMPCAT study: measuring the impact of caregiving on families and healthcare professionals of children and adults living with mucopolysaccharidoses in Ireland
Supplemental material, sj-jpg-1-trd-10.1177_1049732320931430 for IMPCAT study: measuring the impact of caregiving on families and healthcare professionals of children and adults living with mucopolysaccharidoses in Ireland by Suja Somanadhan, Hannah Bristow, Ellen Crushell, Gregory Pastores, Emma Nicholson, Thilo Kroll, Philip J. Larkin and Aoife Brinkley in Therapeutic Advances in Rare Disease
Supplemental Material
sj-pdf-2-trd-10.1177_1049732320931430 – Supplemental material for IMPCAT study: measuring the impact of caregiving on families and healthcare professionals of children and adults living with mucopolysaccharidoses in Ireland
Supplemental material, sj-pdf-2-trd-10.1177_1049732320931430 for IMPCAT study: measuring the impact of caregiving on families and healthcare professionals of children and adults living with mucopolysaccharidoses in Ireland by Suja Somanadhan, Hannah Bristow, Ellen Crushell, Gregory Pastores, Emma Nicholson, Thilo Kroll, Philip J. Larkin and Aoife Brinkley in Therapeutic Advances in Rare Disease
Supplemental Material
sj-pdf-3-trd-10.1177_1049732320931430 – Supplemental material for IMPCAT study: measuring the impact of caregiving on families and healthcare professionals of children and adults living with mucopolysaccharidoses in Ireland
Supplemental material, sj-pdf-3-trd-10.1177_1049732320931430 for IMPCAT study: measuring the impact of caregiving on families and healthcare professionals of children and adults living with mucopolysaccharidoses in Ireland by Suja Somanadhan, Hannah Bristow, Ellen Crushell, Gregory Pastores, Emma Nicholson, Thilo Kroll, Philip J. Larkin and Aoife Brinkley in Therapeutic Advances in Rare Disease
Footnotes
Acknowledgements
The authors are incredibly thankful to the families and HCPs who so generously shared their stories, experiences and insights with this study; without their input this study would not have been possible.
Author contributions
Suja Somanadhan: conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; software; supervision; validation; visualisation; writing original draft.
Hannah Bristow: data curation; formal analysis; funding acquisition; software; writing, review and editing.
Ellen Crushell: conceptualization; investigation; supervision; writing, review and editing.
Gregory Pastores: conceptualization; investigation; supervision; writing, review and editing.
Emma Nicholson: formal analysis; investigation; methodology; supervision; writing, review and editing.
Thilo Kroll: investigation; methodology; supervision; writing, review and editing.
Philip J. Larkin: conceptualization; investigation; methodology; supervision; writing, review and editing.
Aoife Brinkley: conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; supervision; visualization; writing, review and editing.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Student summer scholarship of €2400.00 (R19520) was received from the Health Research Board Ireland towards supporting an undergraduate student to work on this project with the research team.
Ethics Statement
Approval to conduct the study was obtained from the ethical committees of three hospitals in Ireland and University College Dublin:
Children’s University Hospital, Temple Street, Dublin: Ref: 17.007
Our Lady’s Children’s Hospital, Crumlin, Dublin: GEN/547/17
Mater Misericordiae University Hospital, Dublin; Ref: 1/378/1923
University College Dublin: LS-E-17-156-Somanadhan.
Written informed consent was obtained from each of the participants prior to the conduct of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.