
Abstract
Bietti crystalline dystrophy (BCD), a rare autosomal recessive hereditary disorder, is identified by its clinical features. It is characterised by crystalline deposits and hence called crystalline retinopathy. The retinopathy progresses with age, showing a decrease in the number of crystalline deposits and increase in the area of chorioretinal degeneration, which spreads in a centrifugal pattern. Thus, BCD can be confused with other disorders with crystalline-like deposits and chorioretinal degenerations. The red-free and near-infrared reflectance allows prominent visualisation of crystalline deposits that may be missed. The non-inferiority of red-free imaging and its wider availability could allow its use as a screening tool. The enhanced depth imaging optical coherence tomography shows crystalline deposits throughout the retina and outer retinal tubulation. Thus, multimodality imaging can act as an adjunct in diagnosis, monitoring and follow up in these cases, acting not only as a teaching tool but also giving an insight into the underlying pathophysiology of the disorder.
Plain language summary
Bietti crystalline dystrophy is a rare familial disorder but is not shown in all family members and may skip generations, as it has an autosomal recessive pattern of inheritance. It shows refractile yellow-white crystalline deposits and degenerative changes in the retina. These crystalline deposits disappear with age while degenerative changes increase and spread from centre to the periphery. This may cause difficulty in early detection, and confusion with similar degenerative diseases of the retina. The use of various imaging modalities can help in diagnosis and follow up of these cases. These modalities also provide understanding of the basic disease process.
Keywords
Introduction
Bietti crystalline dystrophy (BCD), also known as crystalline retinopathy, corneo-retinal degeneration, or ‘Bietti’s tapetoretinal degeneration with marginal corneal dystrophy’, is an autosomal recessive condition involving the CYP4V2 gene.1–4 It is asymptomatic during the early stage of disease and presents around second to third decade with vision impairment, night blindness and visual field defects. Early stages can be confused with retinopathies with crystalline-like deposits, including hyperoxaluria, cystinosis, drug-related toxicity (tamoxifen, methoxyflurane and canthaxanthin), talc retinopathy, retinitis punctate albescens, fundus albipunctatus, drusens and Sjogren-Larsson syndrome, whereas advanced stages resemble severe forms of retinitis pigmentosa or other chorioretinal degenerative disorders.
Multimodality imaging techniques including fundus fluorescence angiography (FFA), fundus autofluorescence (FAF), optical coherence tomography (OCT), near-infrared reflectance (NIR) and red-free (RF) imaging have revolutionised the field of ophthalmology, thus helping better understanding and knowledge about structural changes and underlying retinal lesions. In addition, improvements in imaging modalities have allowed us wider and better visualisation.5,6 Here, we discuss BCD and the role of various imaging techniques using different platforms, with special emphasis on the NIR and RF imaging in BCD.
Case report
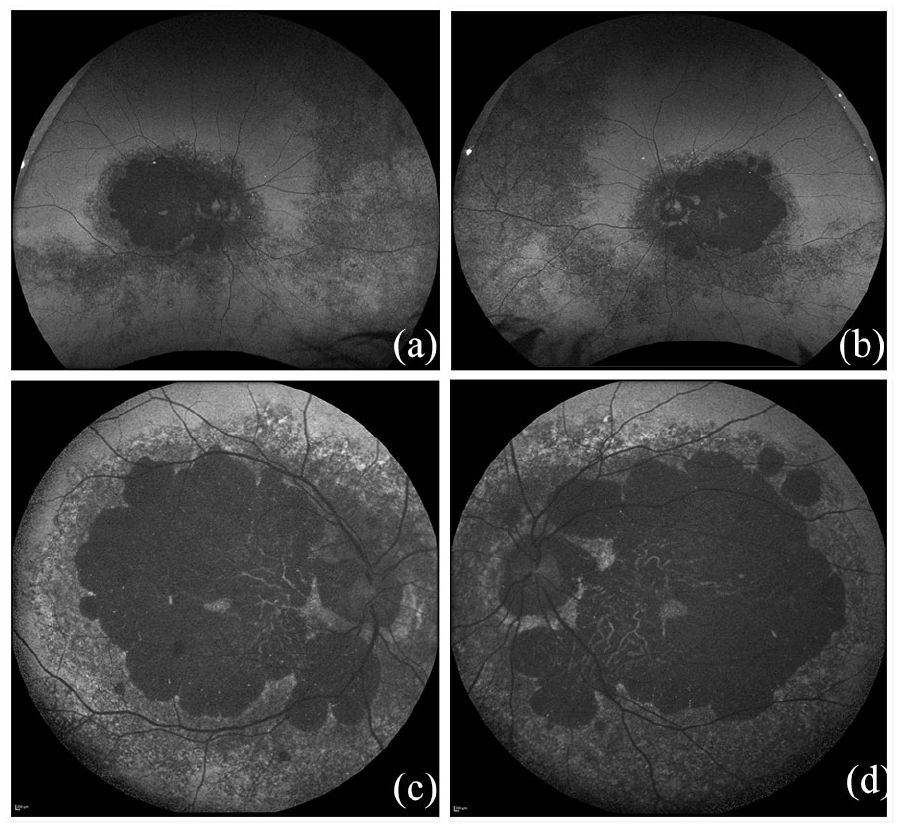
A 35-year-old Asian male, born of non-consanguineous marriage, presented with complaints of insidious onset gradually progressive diminution of vision in both eyes for the past 1 year. He also had history of night blindness for the past 3 years. The presenting visual acuity was 6/36 in right eye (RE) and 1/60 in left eye (LE). On examination, anterior segment was within normal limits and fundus showed degenerative changes, with crystalline yellow deposits prominent at the posterior pole. The choroidal vasculature was prominent in these areas (Figure 1a,b). FFA on Spectralis (Spectralis, Heidelberg Engineering, Heidelberg, Germany) showed an area of central hypofluorescence with surrounding hyperfluorescence. A peripapillary ring and small central area were seen to be preserved (Figure 1c,d). Ultra-widefield Optos (Optos California, P200 Dx, Marlborough, MA, USA) FAF showed central hypoautofluorescence with surrounding mottled autofluorescence indicating, retinal pigment epithelium (RPE) involvement in these areas along with peripheral involvement. (Figure 2a,b). But Topcon (Triton; Topcon Medical Systems, Tokyo, Japan) FAF also showed few hyper-autofluorescence (AF) areas around the margin (Figure 2c,d).

Clinical fundus image showing pigmentary changes with crystalline yellow-white deposits prominent at the posterior pole. The choroidal vasculature was prominent seen in these areas. (a, b) FFA on Spectralis shows area of central hypofluorescence with surrounding hyperfluorescence. (c, d) A peripapillary ring and small central area was seen to be preserved. The enhanced depth imaging – optical coherence tomography showed disorganisation of the RPE, photoreceptors and choriocapillaris at macula except a small central island. (e, f) Retinal and choroidal thinning was prominent with intra-retinal hyper-reflective dots corresponding to deposits. The ORT was also seen suggestive of degenerating RPE cells.
Optos ultra-widefield FAF showed central hypoautofluorescence with surrounding mottled autofluorescence indicating RPE involvement in these areas along with peripheral involvement. (a, b) Topcon FAF showed a few hyperautofluorescence areas around the margin. (c, d) A peripapillary ring and small central area was seen to be preserved.
The Optos ultra-widefield green reflectance (Figure 3a, b) showed central macular changes with few dispersed hyper-reflective spots, whereas the red reflectance (Figure 3c, d) showed prominent choroidal vasculature with no hyper-reflective spots. However, the deposits were seen more prominently on the RF imaging on Topcon and NIR on Spectralis. (Figure 4a–d) The Enhanced depth imaging – OCT (EDI-OCT) (Spectralis, Heidelberg Engineering, Heidelberg, Germany) showed disorganisation of the RPE, photoreceptors and choriocapillaris at macula with exception of a small central island (Figure 1e, f). Retinal and choroidal thinning was prominent, with intra-retinal hyper-reflective dots corresponding to deposits. Outer retinal tubulation (ORT) suggestive of degenerating RPE cells was also seen in both eyes. The patient was diagnosed as BCD, his visual prognosis was explained and he was advised low vision aid trial and regular follow up. The parents were not available for examination and siblings did not show any fundus findings. Genetic screening could not be done as this was unaffordable for the patient. As no intervention was done and only imaging was performed, institutional ethics committee approval was not needed. Written informed consent was obtained from the patient for imaging and publication of the manuscript.

The Optos imaging using green reflectance (a, b) showed central macular changes with few dispersed hyper-reflective spots while the red reflectance (c, d) showed prominent choroidal vasculature.

RF image on Topcon (a, b) and near infra-red imaging on spectralis (c, d) showing central macular changes with dispersed hyper-reflective spots and choroidal vasculature. Deposits can be seen distinctly on RF imaging.
Discussion
BCD is a rare autosomal recessive corneoretinal crystalline dystrophy involving the CYP4V2 gene. Corneal involvement is seen in 50–66% cases and is not an essential criteria for diagnosis as the CYP4V2 protein is expressed mainly in the retina.7–9 The fundus shows intraretinal crystalline deposits, distributed in different retinal layers from the nerve fibre layer to the photoreceptors. These crystals are larger, up to 50 microns in size, and distributed along the peripheral margin. Further, the distribution of crystals varies with the stage of disease. 10 As the disease progresses, crystals decrease in number and become concentrated near the RPE. Thereafter, loss of RPE and sclerosis of choriocapillaris ensues, resulting in chorioretinal atrophy. The macular island and peripapillary ring are partially spared until the advanced stages of the disease, as was seen in our case (Figure 1a–d). 4 Such advanced stages may be confused with other chorioretinal degenerations, leading to missed diagnosis. Thus, multimodality imaging including FFA, FAF, retinal reflectance, RF and OCT helps in early diagnosis and in differentiation from other simulating conditions.
In our case, the crystalline deposits were visible clinically on fundus examination along with the pigmentary changes. FFA in BCD has been considered as a standard tool for evaluating the extent of involvement and progression.2,4,9 On FFA, BCD shows hypofluorescent area with surrounding hyperfluorescent border but the crystalline deposits are not observed (Figure 1c, d). FAF is an imaging technology giving information about the status of the RPE, and the deposits are seen as hypo and hyper depending on its composition. The blue-AF or short-wavelength (SW) AF, has the exciting and emission filters at 488 nm and 500–700 nm, respectively, while the medium wavelength (MW)/long-wavelength (LW) AF uses longer exciting wavelength of 532 nm and has emission above 540–800 nm. The AF signal is derived mainly from lipofuschin of RPE with either wavelength, except that MW/LW-AF also gives better assessment of the fovea. 11 In BCD, FAF helps in assessing damage occurred and speculating about the course of disease but does not show the crystalline deposits. The Optos ultra-widefield (MW/LW) FAF, showed the mid-peripheral and peripheral involvement in addition to the posterior pole abnormalities, giving a more comprehensive assessment in these cases (Figure 2a, b). The peripheral pigmentary changes explains the progressive loss of visual fields seen in BCD. Comparatively, the Topcon FAF, which is again MW/LW, showed some hyper-reflective areas around the peripheral margin (Figure 2c, d). The crystalline deposits in BCD are known to be a collection of cholesterol esters because of abnormal lipid metabolism.2,3,5,12 But this is not supported by biochemical study. 13 The lack of AF with crystals suggests that they are not composed of any fluorophores.
Infrared (IR) light has wavelength longer than the visible spectrum. It is divided into near-infrared (0.7–1.4 microns), mid-infrared (1.4–15 microns) and far-infrared (15–1000microns). The IR wavelengths used for retinal reflectance imaging in Spectralis are beyond 780 nm, and thus fall within the NIR spectrum. Likewise in Optos California, green reflectance (532 nm) is light reflected from structures above the RPE while red reflectance (640 nm) shows more prominent choroidal vessels as it penetrates deeper. In our case, the intra-retinal crystalline deposits were prominently hyper-reflective on NIR reflectance when compared with green and red reflectance images taken using Optos (Figures 3, 4). This may be due to the longer wavelength of NIR allowing deeper penetration with better visualisation of subretinal structures. 14 Interestingly, on RF (green light) imaging on Topcon, crystalline deposits were noted equivocally to NIR reflectance, showing the utility of same. RF imaging is a type of monochromatic photography with a green filter, which is a broadband absorption filter with maximum transmission at 540 nm. It has less scatter and excellent contrast. Although one would expect green reflectance (optos) to yield similar results to RF imaging (topcon), its narrower bandwidth of absorption might limit its utility. Previous studies have shown that crystalline deposits in BCD are better visualized on the NIR imaging when compared with other modalities.6,15–17 However, in view of non-inferiority of RF imaging in delineating these deposits and its wider availability, it might be prudent to consider it as a primary screening tool before NIR reflectance.
Image resolution is important to detect subtle fundus changes and can affect interpretation of data. It depends upon the camera, degree of image captured, and image size. 18 The axial resolution of Optos, Topcon and Spectralis is 6, 2.6 and 3.9 µm, respectively, while the transverse resolution is 20, 20 and 14 µm, respectively, but studies have demonstrated good agreement between conventional and wide field imaging. 19 EDI-OCT of both eyes, in this case, showed ORT, disruption of ellipsoid zone with faintly visible crystalline deposition in outer retinal layers and preserved foveal contour. The hyper-reflective intraretinal deposits have been shown to correspond to crystalline deposits, inflammatory cells, protein deposits or the glial response to retinal degeneration.20–22 These hyper-reflective deposits have also been seen in the choroid layer. 23 OCT can also help in visualisation of the progression of the disease and can also be used for follow up of these disorders as these cases can develop neurosensory detachment, subretinal neovascularisation, a macular hole or cystoid macular oedema (CME). 7 ORT has been reported with a spectrum of pathologies, including Bietti dystrophy.7,24,25 The ORTs are spherical hyporeflective areas surrounded by a hyperreflective area found mainly in the outer nuclear layer frequently in advanced stages. It is a protective mechanism, whereby the damaged photoreceptor layer that has some function undergoes rearrangement and invagination.26,27
Multimodality imaging in rare diseases not only helps as a teaching tool but also gives an insight into pathophysiology. It can help in diagnosis, progression and follow up. To best of our knowledge, this is the first report comparing different FAF and retinal reflectance imaging platforms in the same patient. It emphasises the use of IR reflectance and RF imaging compared with colour fundus photography, FAF and retinal (green/red) reflectance in demonstrating retinal crystals in BCD, facilitating early diagnosis in suspected cases. Also, being non-inferior to IR, RF imaging can be used as a primary screening tool for detection of crystalline deposits and their distribution.
Footnotes
Authour Contributions
Conflict of interest
The authors declare that there is no conflict of interest.
Ethics statement
Manuscript prepared according to the World Medical Association Declaration of Helsinki. As no intervention done, ethics committee approval was not required. Written informed consent for publication was obtained from the patient. The manuscript is not presented anywhere and not being considered for publication elsewhere. The manuscript has been reviewed and approved by all named authors. The criteria for authorship have been met and each author believes that the manuscript represents honest work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.