
Abstract
Background
Psychological distress, maladaptive illness perceptions, and reduced quality of life are common following acute myocardial infarction (AMI) and may negatively influence recovery and treatment adherence. Mindfulness-based cognitive therapy (MBCT) has demonstrated benefits for emotional regulation; however, evidence for internet-based brief MBCT (B-MBCT) interventions in post-AMI populations remains limited. The present study examined the preliminary effectiveness and feasibility of an internet-based B-MBCT intervention in improving psychological outcomes following AMI.
Methods
This pilot randomized controlled trial included 18 medically stable post-AMI participants with mild to moderate depressive symptoms. Participants were randomly allocated to an internet-based B-MBCT plus treatment-as-usual (TAU) group or a TAU-only group. The intervention consisted of 8 weekly online sessions. Outcomes were assessed at baseline and post-intervention using the Depression Anxiety Stress Scale-21 (DASS-21), Brief Illness Perception Questionnaire, Five Facet Mindfulness Questionnaire-15, and MacNew Quality of Life Questionnaire.
Results
Compared with TAU, the intervention group demonstrated significantly greater reductions in depression, anxiety, stress, and illness perception, along with significant improvements in mindfulness skills and quality of life (P < .05). Effect sizes were large across outcomes (η² = 0.59-0.94).
Conclusion
Internet-based B-MBCT appears feasible and shows promising preliminary effectiveness for improving psychological outcomes following AMI. Larger randomized trials are required to confirm these findings.
Introduction
Acute myocardial infarction (AMI) is a major public health concern 1 and is frequently accompanied by significant psychological morbidity, including depression, anxiety, maladaptive illness perceptions, and a reduced quality of life (QOL). 2 Psychological distress followed by an AMI has been shown to negatively affect recovery, treatment adherence, functional outcomes, and long-term prognosis. Despite these issues, psychological care remains ignored in routine cardiac rehabilitation, especially in low- and middle-income countries such as India. 3
Depression is one of the most common psychological issues observed following AMI, with prevalence rates also higher compared to the general population. 4 Post-AMI depression has been associated with poorer health behaviors, reduced engagement with rehabilitation process, and increased healthcare burden. 5 In addition to depressive symptoms, patients often develop maladaptive illness perceptions characterized by heightened emotional distress, catastrophic interpretations, and reduced perceived control over their illness, which further influence recovery and QOL.6, 7
Psychological interventions, particularly cognitive-behavioral approaches, have shown effectiveness in reducing emotional distress and improving QOL in people with cardiac illness. 8 Mindfulness-based cognitive therapy (MBCT) integrates mindfulness practices with cognitive strategies to improve awareness of maladaptive thought patterns and emotional responses to them. Emerging evidence suggests that mindfulness-based interventions may be helpful in reducing depressive symptoms and more adaptive illness-related beliefs in individuals with cardiovascular disease.9, 10
However, a structured psychological intervention remains limited due to resource constraints, a shortage of trained professionals, and logistical barriers. Internet-based psychological interventions offer a useful approach to address these gaps by improving accessibility and continuity of care.11, 12 Brief and internet-delivered interventions may be particularly suitable for post-AMI patients who often face physical limitations and time constraints during recovery.
While previous studies have examined mindfulness-based interventions in cardiac populations, evidence for brief, internet-delivered MBCT interventions in post-AMI patients, especially within the Indian context, remain unexplored. 13 Moreover, fewer studies have simultaneously studied depressive symptoms, illness perception, mindfulness skills, and QOL as integrated outcomes of intervention.
Therefore, the present study aimed to examine the preliminary effectiveness of an internet-based brief mindfulness-based cognitive therapy (B-MBCT) intervention, delivered along with treatment-as-usual (TAU), in reducing depressive symptoms and improving illness perception, mindfulness, and health-related QOL in patients recovering from AMI.
To our knowledge, few studies have examined internet-delivered MBCT specifically in post-AMI populations within low- and middle-income countries.
Materials and Methods
Study Design and Sample
This pilot randomized controlled trial compared internet-based B-MBCT plus TAU group with the TAU group alone. Assessments were conducted at baseline and immediately after the 8-week intervention. The study was conducted at a tertiary care hospital in North India and approved by the Institutional Ethics Committee. Written informed consent was obtained from all participants.
Sample
A consecutive sampling method was used to screen participants from the Cardiology Outpatient Department. Due to unforeseen constraints (i.e., COVID-19 pandemic restrictions), a small sample size was used for this pilot study. The sample included 18 participants aged 18-60 years with a history of one AMI and who were medically stabilized as suggested by the cardiologist. Participants were allocated to a B-MBCT group using a 1:1 allocation ratio (n = 9; mean age 44.00 ± 9.08) or a TAU group (n = 9; mean age 47.44 ± 7.16).
The sample size was calculated based on detecting a difference in the mean scores of the primary outcome measure between the two groups. Assuming a power of 80% and a significance level of alpha = 0.05, the required sample size was calculated to be n = 9 in each arm, resulting in a total sample of N = 18 participants. Participants gave their informed consent, confidentiality was ensured, participation was voluntary, and no monetary incentives were offered.
Inclusion Criteria
History of AMI within the past month.
Currently medically stable and cleared for participation by the treating cardiologist.
Able to understand study assessments.
Cooperative during the interview, assessments, and intervention process.
Screened positive for a current depressive episode using the Modified Mini Screen (MMS).
Exclusion Criteria
Clinical history suggestive of any psychiatric illnesses (e.g., psychosis, bipolar disorder), excluding the target condition of major depressive episode.
Presence of severe or extremely severe levels of depression, as indicated by a Depression Anxiety Stress Scale-21 (DASS-21) depression subscale score of more than 14 (severe/extremely severe range).
Presence of neurological or serious medical conditions (other than stable coronary artery disease [CAD]).
Received psychological intervention in the last 6 months or is currently receiving any psychological treatment.
Measures
Screening Instrument
All participants were screened using the MMS, a brief screening tool derived from the Mini-International Neuropsychiatric Interview and used to exclude major psychiatric conditions such as psychosis, bipolar disorder, or active suicidality.
Depression, Anxiety, and Stress
The DASS-21 was used to assess depression, anxiety, and stress symptoms. The scale demonstrates good internal consistency, with Cronbach’s alpha values of 0.81 (depression), 0.89 (anxiety), and 0.78 (stress).
Illness Perception
Illness perceptions were assessed using the Brief Illness Perception Questionnaire (B-IPQ), a nine-item self-report measure assessing cognitive and emotional representations of illness.
Mindfulness Skills
Mindfulness skills were measured using the Five Facet Mindfulness Questionnaire-15 (FFMQ-15), which assesses observing, describing, acting with awareness, non-judging of inner experience, and non-reactivity. The scale demonstrates good internal consistency and sensitivity to change following mindfulness-based interventions.
Health-related Quality of Life
Health-related QOL was assessed using the MacNew Quality of Life after Myocardial Infarction Questionnaire (MacNew QLMI). The instrument comprises 27 items across emotional, physical, and social domains, with higher scores indicating better QOL.
Intervention
The intervention group received an adapted, online B-MBCT protocol, delivered concurrently with TAU.
The intervention was adapted from the standard 8-week MBCT protocol described by Segal et al., 14 with modifications to suit post-AMI patients and online delivery.
Key adaptations included:
Reduced duration: The standard 8-week program was maintained, but the session length was reduced from the typical 90-120 min to 45-50 min per week. This reduction was implemented to ensure better adherence and reduce the cognitive burden on participants recovering from an AMI. Delivery format: All sessions were conducted online via an audio/visual internet-based platform. This format was selected for its accessibility and safety during the COVID-19 pandemic. Activity modification: Specific MBCT meditations and cognitive exercises were adapted to be less physically taxing and more psychologically focused on the experience of living with a cardiac illness. Focus on body sensations: Exercises related to body scanning and physical sensations were carefully framed to avoid triggering health anxiety or distress related to cardiac symptoms, emphasizing a non-judgmental awareness rather than catastrophic interpretation. Cognitive modules: The cognitive component maintained its focus on recognizing links between mood and thought patterns, but examples and discussions were tailored to address common post-AMI concerns (e.g., fear of recurrence, illness perception, and limitations). Home practice: The requirement for daily home practice was maintained, with tailored, shorter guided audio files provided to match the reduced session length.
The intervention protocol was adapted from the standard MBCT framework described by Segal et al. 14 The modifications were introduced to enhance feasibility for participants recovering from AMI and to facilitate online delivery. As the present study was designed as a pilot randomized controlled trial, the aim was to evaluate feasibility and preliminary effectiveness rather than formally validate the adapted intervention protocol. Future studies may further evaluate the psychometric and clinical validity of the adapted intervention in larger samples.
Procedure
The study design involved three distinct phases: recruitment and screening, baseline assessment and randomization, and intervention and post-intervention assessment. Eligible participants were identified through referral by their treating cardiologist. After providing informed consent, participants underwent screening using the MMS and DASS-21. Those meeting eligibility criteria completed baseline assessments, including the MacNew QLMI, B-IPQ, and FFMQ-15. Participants were then randomly assigned to either the B-MBCT group or the TAU group using a 1:1 allocation ratio. The intervention was delivered over 8 weeks. At the end of the intervention period, all participants completed post-intervention assessments using the same outcome measures to evaluate changes in depressive symptoms (primary outcome), illness perception and QOL (secondary outcomes), and mindfulness skills (process measure). All participants continued receiving standard cardiology treatment prescribed by their cardiologists and completed the intervention period and post-intervention assessment, resulting in no attrition during the study.
Statistical Analysis
The obtained data were statistically analyzed and interpreted with the help of a computer-based statistical tool IBM Statistical Package for the Social Sciences (SPSS) for Windows. The Shapiro–Wilk test was used to test whether the distribution was normal or approximately normal, and based on this, further comparative statistics were used. Due to the small sample size of the study, non-parametric statistics were used in the analysis of the data.
For age distribution, an unpaired t-test was used. To understand the distribution of discrete sociodemographic and clinical variables like sex, religion, marital status, and domicile frequency percentages, Fisher’s exact test was computed. Differences in the scores of the study scales were compared within groups using the Wilcoxon signed-rank test, and for between-group comparison of differences, the Mann–Whitney U test was calculated. Effect sizes (η²) were calculated from the Z statistics obtained from the Mann–Whitney U tests using the formula η² = Z²/N, where N represents the total sample size. Effect size values were interpreted using conventional benchmarks for small (0.01), medium (0.06), and large (0.14) effects.
Results
Statistical significance was interpreted at P < .05, with several outcomes reaching stronger levels of significance (P < .01).
Baseline Sociodemographic and Clinical Characteristics of Participants
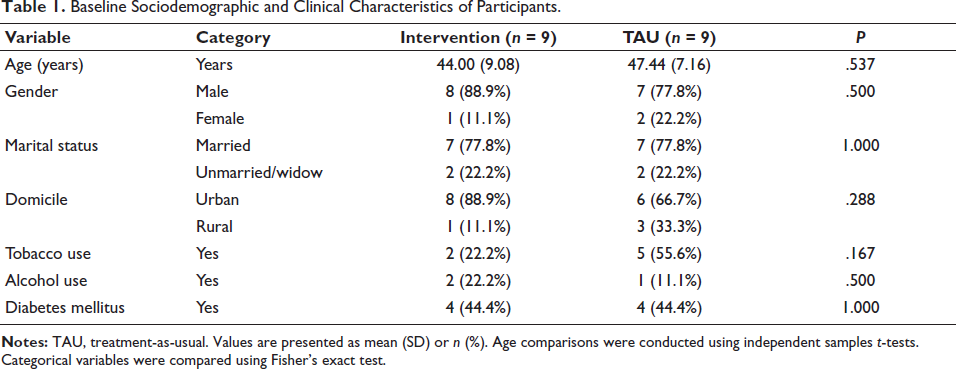
Baseline sociodemographic and clinical characteristics are presented in Table 1. No significant baseline differences were observed between groups.
Baseline Sociodemographic and Clinical Characteristics of Participants.
Psychological Outcomes
Depression, Anxiety, and Stress
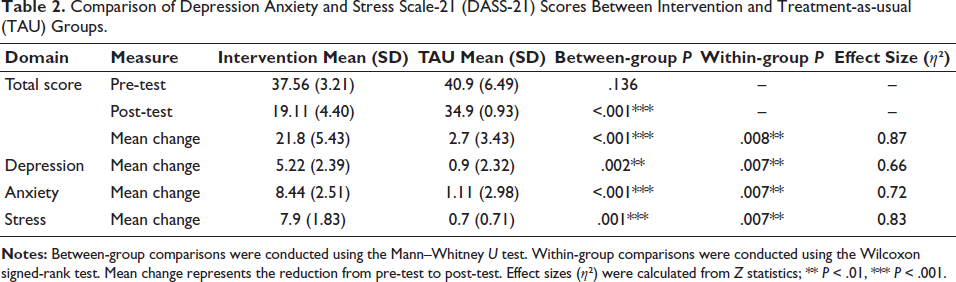
Between-group comparisons of DASS-21 scores are presented in Table 2. No significant differences were observed between groups at baseline. At post-intervention, the intervention group demonstrated significantly lower DASS total and subscale scores compared to the TAU group. Descriptive analysis of mean change scores indicated greater reductions across depression, anxiety, and stress domains in the intervention group compared with TAU, while statistical comparisons were conducted using non-parametric tests. Within-group analyses showed significant reductions across all domains in the intervention group, whereas the TAU group demonstrated a significant reduction only in stress.
Comparison of Depression Anxiety and Stress Scale-21 (DASS-21) Scores Between Intervention and Treatment-as-usual (TAU) Groups.
Mindfulness Skills
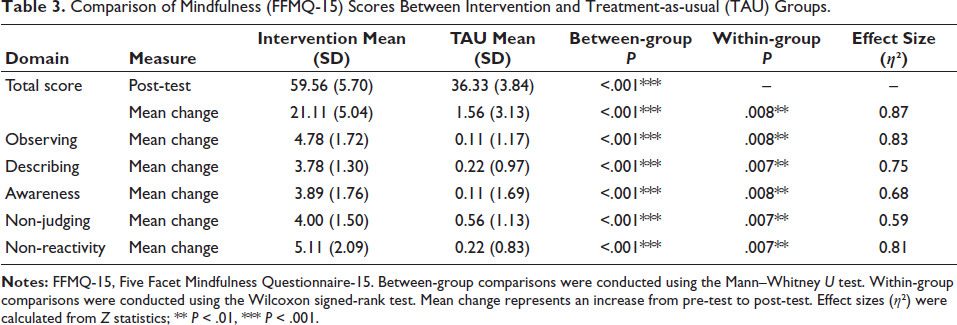
Results for mindfulness outcomes are presented in Table 3. At post-intervention, the intervention group demonstrated significantly higher total mindfulness scores compared to the TAU group. Mean change analysis revealed significantly greater increases in overall mindfulness and across all five mindfulness facets in the intervention group. No significant changes were observed within the TAU group for total or domain-specific mindfulness scores.
Comparison of Mindfulness (FFMQ-15) Scores Between Intervention and Treatment-as-usual (TAU) Groups.
Illness Perception and Quality of Life
Between-group comparisons of illness perception outcomes are presented in Table 4. At post-intervention, the intervention group demonstrated significantly lower total illness perception scores compared to the TAU group, reflecting lower illness perception scores.
Comparison of Illness Perception Scores Between Intervention and Treatment-as-usual (TAU) Groups.
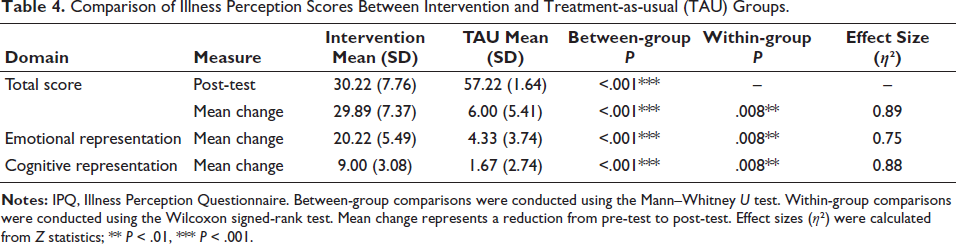
Mean change analysis showed significantly greater improvements in total illness perception, emotional representation, and cognitive representation domains in the intervention. The TAU group demonstrated significant improvement only in emotional representation, with no significant change observed in cognitive representation.
Quality of Life
Quality of life outcomes are presented in Table 5. At post-intervention, the intervention group reported significantly higher overall QOL scores compared to the TAU group.
Comparison of Quality-of-life Scores Between Intervention and Treatment-as-usual (TAU) Groups.
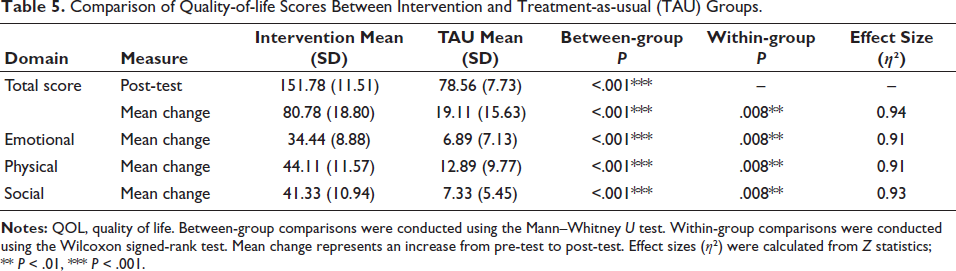
Mean change analyses demonstrated significantly greater improvements in total QOL and across emotional, physical, and social domains in the intervention group. Although the TAU group also showed statistically significant improvements across domains, the magnitude of change was smaller compared to the intervention group.
Discussion
Acute myocardial infarction is associated with significant psychological distress that may affect recovery and QOL. This study provides preliminary evidence supporting the potential effectiveness of an internet-based B-MBCT program as an adjunct to standard care following AMI.
Psychological Distress: Depression and Anxiety
The significant reduction in depression and anxiety symptoms observed in the Intervention group supports the potential usefulness of the intervention in addressing the psychological manifestations that might be due to AMI. The beneficial effects of B-MBCT on anxiety and depressive symptoms are consistent with the previous research studies that show the benefits of mindfulness-based intervention for depression and anxiety15-17 and also that such interventions can enhance positive emotion regulation strategies and self-compassion, while decreasing rumination and experiential avoidance.18, 19
Stress Response and Resilience
There has been a significant improvement in the stress level in both the intervention and TAU groups at the post-assessment level. However, the improvement was statistically significantly higher in the intervention group. This finding may reflect natural psychological recovery over time, as participants were recruited at least 1 month after the myocardial infarction event.20, 21
This has also been reported in the previous studies that overall, participants’ perceptions of stress decreased over time, particularly during the first month following AMI, and also that men have a lower level of perceived stress as compared to women. 22 Another reason for stress reduction in the TAU group can be that most of the participants were married men, and men tend to get more social support and care as compared to women.23, 24
Increased Mindfulness and Quality of Life
The study’s strength lies in demonstrating that the internet-based B-MBCT successfully enhanced the participants’ mindfulness skills. The significant increase observed in the Five Facet mindfulness in the B-MBCT group confirms the positive effect of the protocol in enhancing mindfulness skills. 25 Improvements in mindfulness facets such as non-judging and non-reactivity may help patients observe illness-related thoughts and bodily sensations with greater acceptance, thereby reducing psychological distress.26-28 Another significant finding was the significant increase in overall QOL in the B-MBCT group compared to TAU. 29 While the TAU group also experienced improved QOL due to natural physical healing and the resumption of activities post-AMI or just passing of time, 30 the substantial difference observed in the intervention group suggests that B-MBCT provides important additive psychosocial benefit.
Illness Perception: Mechanisms of Change
In this study, there has been a significant improvement in the illness perception in both intervention and TAU groups. However, the improvement was statistically significantly higher in the intervention group.
The benefits of B-MBCT over TAU appear to be more in the cognitive representation of illness domain, whereas the TAU group’s improvement was more strongly associated with a reduction in emotional representation of the illness. This differential effect highlights the contribution of the cognitive restructuring element of B-MBCT, which helps participants identify and reframe maladaptive beliefs, thus enhancing their perceived control over their condition.
Several reasons can be hypothesized for the significant improvement in the TAU group. Since all the patients recruited in the study were from North India, where the joint family is the basic social unit. As a result, a strong sense of family support may alter illness perception and lead to engage positively in cardiovascular health behavior and avoid harmful health behavior.31-33 Furthermore, individuals within collectivistic cultures often demonstrate a greater propensity to adhere to medical advice and integrate lifestyle modifications, mostly driven by a desire to maintain family peace and fulfill their societal roles. 18 Another reason can be availability of good and accessible medical care facilities and patients coming in contact with their cardiologist. 34 This can come in the form of reassurance given by medical staff, and also positive test results on further assessment.
Limitations
The study has several limitations. First, the relatively small sample size limits the statistical power of the study, and additionally, the sample consisted predominantly of male participants, which may limit the generalizability of the findings. As this study was designed as a pilot randomized controlled trial, the results should be interpreted as preliminary evidence. Future multicenter randomized controlled trials with larger samples are required to confirm these findings and examine long-term outcomes. The small sample size also limited the feasibility of conducting subgroup analyses comparing mild and moderate depressive symptom severity.
Second, the study did not include long-term follow-up assessments beyond the 8-week intervention period. Therefore, the sustainability of the observed psychological improvements cannot be determined. Future research should include longer follow-up periods (e.g., 6-12 months) to evaluate the sustainability of intervention effects. Also, the large effect sizes observed should be interpreted cautiously, as effect size estimates in small pilot samples may be unstable and require confirmation in larger studies. As a pilot randomized controlled trial, the study was primarily designed to examine feasibility and preliminary effectiveness rather than to provide definitive efficacy estimates.
Conclusion
The findings provide preliminary evidence supporting the feasibility and potential effectiveness of an internet-based B-MBCT intervention as an add-on to regular medical care for participants recovering from AMI. Such interventions may represent a practical and scalable approach to integrating psychological care within cardiac rehabilitation programs, particularly in resource-limited settings. These findings highlight the potential value of integrating brief digital psychological interventions within cardiac rehabilitation programs. Further research is needed to confirm these findings and explore their long-term clinical implications.
Footnotes
Acknowledgments
The authors thank the staff of the Cardiology Outpatient Department, King George’s Medical University, Lucknow, for their support in patient recruitment.
Authors’ Contributions
Clinical Trial Registration
This pilot study was not registered in a clinical trial registry. However, the study protocol was approved by the institutional ethics committee prior to participant recruitment.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request, subject to ethical approval and participant confidentiality requirements.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the Institutional Ethics Committee of King George’s Medical University, Lucknow, India (registration no.: ECR/262/Inst/UP/2013/RR-19; ref. code: 107th ECM IIB M. Phil/P2; date of approval: April 16, 2021).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written informed consent was obtained from all participants prior to enrolment in the study. Participants were informed about the nature of the study, intervention procedures, potential risks and benefits, and their right to withdraw at any time without consequences to their medical care.