
Abstract
Background
Balloon dilation is an established option for selected left heart obstructive lesions in infants, traditionally using low-profile, low-pressure balloons. Experience with high-pressure, rapid-exchange systems such as the Aviator Plus in this age group remains limited.
Objective
To describe feasibility, procedural performance, and early outcomes of off-label balloon dilation using the Aviator Plus platform in infants with coarctation of the aorta or valvular aortic stenosis.
Methods
A retrospective review was performed of infants undergoing Aviator Plus balloon dilation between April 2024 and July 2025. Clinical features, procedural details, and follow-up outcomes were summarized descriptively.
Results
Four infants (mean age 5.5 months; mean weight 5.87 kg) underwent intervention: three with native coarctation of the aorta and one with severe aortic stenosis. One coarctation of the aorta patient had significant left ventricular dysfunction; the aortic stenosis patient had moderate mitral regurgitation. Balloon dilation used a single 6 × 20 mm balloon in two cases and sequential 6 × 20 mm and 7 × 20 mm balloons in two. All procedures produced immediate gradient reduction. During a mean 8.5-month follow-up, one infant with aortic stenosis died from progression of mitral regurgitation and intercurrent infection, and one coarctation of the aorta patient required surgical repair for re-coarctation. The remaining infants maintained gradient relief with preserved ventricular function.
Conclusions
This early experience suggests that the Aviator Plus balloon can be a feasible off-label option for carefully selected infants with left heart obstruction, particularly where pediatric-specific balloons are limited. Larger series with extended follow-up are needed to define long-term outcomes.
Keywords
Introduction
Severe left heart obstructive lesions, such as coarctation of the aorta (CoA) and isolated valvular aortic stenosis (AS), represent critical congenital narrowing of the left ventricular (LV) outflow tract. These lesions frequently manifest in neonates and young infants with heart failure, poor systemic perfusion, or severe hypertension. While surgical repair remains the standard of care for neonates with critical CoA, balloon angioplasty has emerged as an accepted alternative in selected situations—particularly in unstable infants, those with prohibitive surgical risk, or in resource-limited settings. Similarly, balloon aortic valvotomy is well-established as first-line therapy for severe valvular AS in infancy. Beyond the neonatal period, balloon angioplasty is a reliable and widely adopted method to relieve left heart obstruction.
The Aviator Plus balloon (Cordis Corporation, FL, USA), designed primarily for peripheral interventions such as carotid and renal angioplasty, features a low-profile, high-pressure, rapid-exchange design that may offer advantages in the delicate vasculature of infants. However, its use in infantile left heart obstructive lesions has not been systematically evaluated. Here, we describe a series of four infants undergoing balloon angioplasty for native CoA using the Aviator Plus balloon in an off-label setting, with emphasis on procedural feasibility, safety, and short-term outcomes.
Materials and Methods
Study Design
A retrospective observational study was conducted at a tertiary pediatric and congenital cardiac center.
Patient Selection
All infants diagnosed with severe left heart obstructive lesions (native CoA and severe aortic valvular stenosis) who underwent balloon angioplasty using the Aviator Plus balloon between April 2024 and July 2025 were included.
Inclusion Criteria
Severe native CoA with significant pressure gradient, with diastolic tailing in the echocardiogram
Severe valvular AS
Babies with severe left heart obstructive lesions deemed high-risk for immediate surgical intervention or requiring palliation
Age <12 months
Exclusion Criteria
Any patients with left heart lesions associated with other significant congenital heart disease, such as significant shunt lesions or complex structural heart disease, were excluded.
Procedure
All interventions were performed under conscious sedation with local anesthesia through femoral arterial and venous access. Baseline hemodynamics were recorded, followed by angiography to delineate the anatomy. Balloon sizing was guided by echocardiographic measurements—using the adjacent aortic dimensions for coarctation and the aortic annulus for valvular stenosis—and corroborated with angiographic data.
A 4F Terumo radial Glide sheath (Terumo Medical Corporation, Ann Arbor, MI, USA) was employed for balloons up to 6 mm, while a 4/5F Slender Glide sheath was used for 7 mm balloons, permitting 5F catheter compatibility within a 4F profile. Lesions were crossed with a 0.014″ coronary wire, and the Aviator Plus balloon (Cordis US Corporation, Miami Lakes, FL, USA) was advanced across the target segment. Dilatation was performed with an indeflator, with rapid right ventricular pacing for aortic valvuloplasty. Pressure gradients were recorded before and after intervention. Post-dilatation angiography was used to assess procedural efficacy and to exclude complications such as dissection or aortic regurgitation. Femoral pulse loss, when observed, was managed with heparin.
The Balloon
The Cordis Aviator Plus PTA Balloon is a high-pressure device designed for peripheral endovascular interventions, including percutaneous transluminal angioplasty (PTA) of the iliac, femoral, iliofemoral, popliteal, infrapopliteal, renal, and carotid arteries, as well as for the treatment of obstructive lesions in native or synthetic arteriovenous dialysis fistulae. It is also indicated for post-dilatation of both balloon-expandable and self-expanding stents within the peripheral vasculature. In this study, the balloon was used off-label for congenital cardiac intervention in infants, reflecting the common need to adapt available hardware in pediatric practice due to limited equipment designed specifically for this age group. Unlike conventional low-pressure balloons, the Aviator Plus offers high-pressure capability, a rapid exchange platform, ultra-low profile, and enhanced pushability, facilitating safe navigation across tortuous anatomies—particularly relevant for carotid and renal interventions.1, 2
Ethics Approval and Consent
This retrospective study adhered to the approved protocol of the ethical committee. Patient confidentiality was maintained by complete anonymization of clinical and imaging data. As the study involved retrospective analysis of anonymized information, the requirement for individual research consent was waived by the committee.
All infants had undergone clinically indicated catheter-based interventions after standard parental informed consent for the procedure, including acknowledgment of balloon characteristics and off-label balloon use, where applicable. The use of the Aviator Plus balloon reflected clinician judgment in a setting where dedicated neonatal hardware is limited, consistent with established practice in pediatric and congenital cardiac catheterization.
Statistical Method
Continuous variables were expressed as mean ± standard deviation (SD). Categorical variables were presented as frequencies and percentages. Statistical significance was set at a P value less than .05 for all analyses.
Results
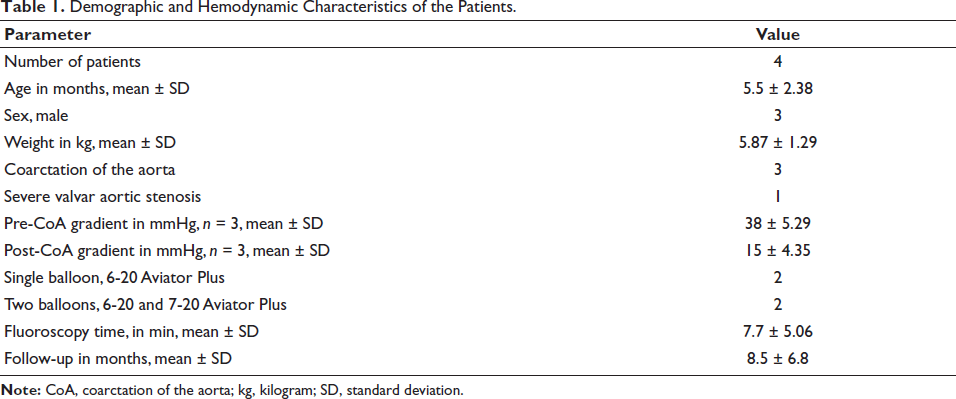
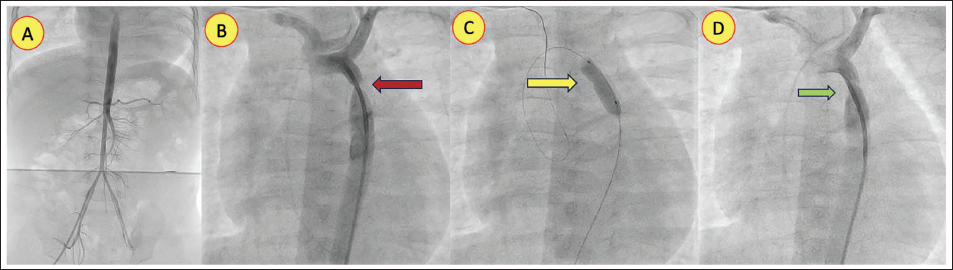
A total of four infants, with a mean age of 5.5 ± 2.38 months and a mean weight of 5.87 ± 1.29 kg, underwent balloon dilation for left heart obstructive lesion. Three of the four patients were male (Tables 1 and 2). The study cohort had three infants with native CoA (Figures 1B; 2A, 2B; 3A). The fourth infant had severe valvular AS complicated by moderate to severe mitral regurgitation and moderate LV dysfunction (Figure 4A). The primary symptoms at presentation were respiratory distress (n = 1) and poor weight gain (n = 2). Two patients had a bicuspid aortic valve as an additional issue.
Demographic and Hemodynamic Characteristics of the Patients.
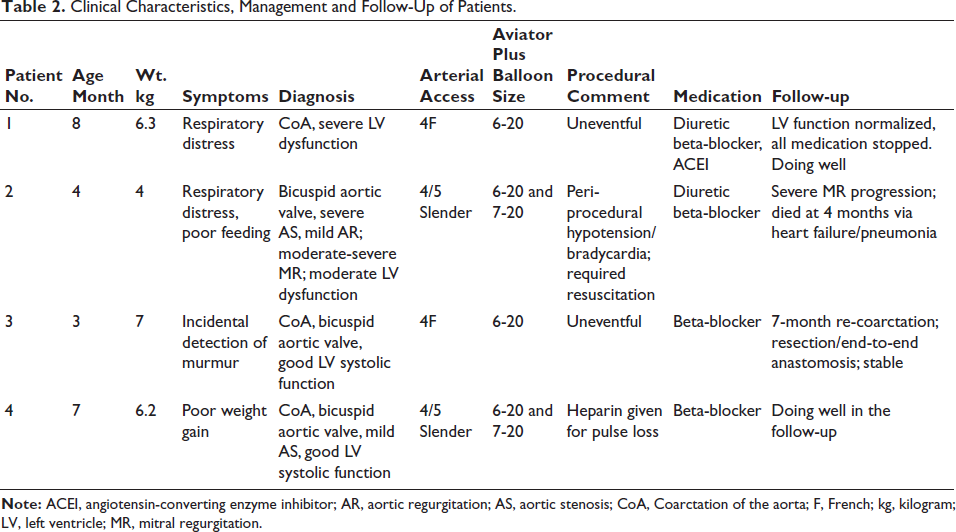
Clinical Characteristics, Management and Follow-Up of Patients.
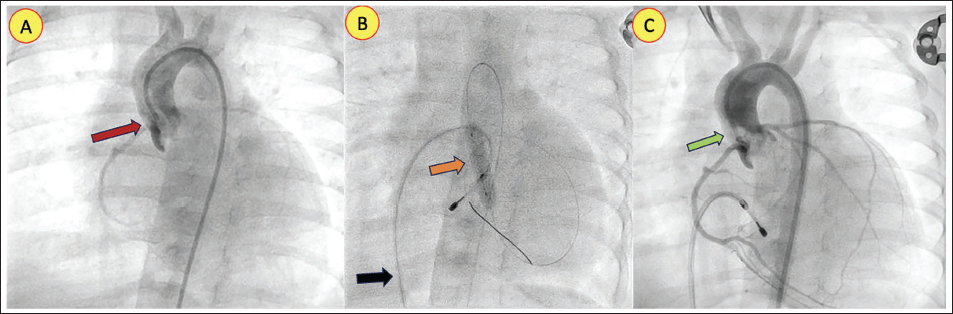
(A) Femoral Arterial Angiogram Showing Markedly Small-caliber Peripheral Vessels. (B) Aortic Angiogram Demonstrating Severe Native Coarctation (Maroon Arrow). (C) Aviator Plus Balloon Inflated Across the Coarctation Segment (Yellow Arrow). (D) Post-angioplasty Angiogram Showing a Widely Patent Coarctation Segment with Improved Luminal Caliber (Green Arrow).
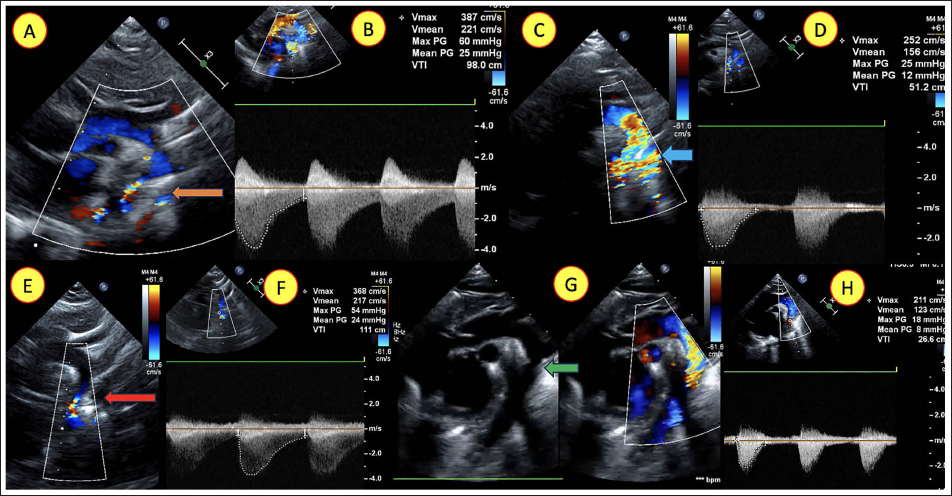
(A) Suprasternal Color Doppler Echocardiogram Demonstrating Severe Coarctation of the Aorta (Orange Arrow). (B) Continuous-wave Doppler Showing a High Gradient Across the Arch with Diastolic Tailing. (C) Post-balloon Angioplasty Echocardiogram Showing Improved Antegrade Flow Across the Coarctation (Blue Arrow). (D) Post-procedure Doppler with Reduced Gradient and Loss of Diastolic Tailing. (E) Follow-up Echocardiogram Demonstrating Severe Re-coarctation (Red Arrow). (F) Corresponding Doppler Tracing with Elevated Gradients and Diastolic Tailing. (G) Post-surgical Repair Echocardiogram Showing a Widely Patent Arch Segment (Green Arrow). (H) Post-surgical Repair Doppler with Markedly Reduced Gradient and No Diastolic Tailing.
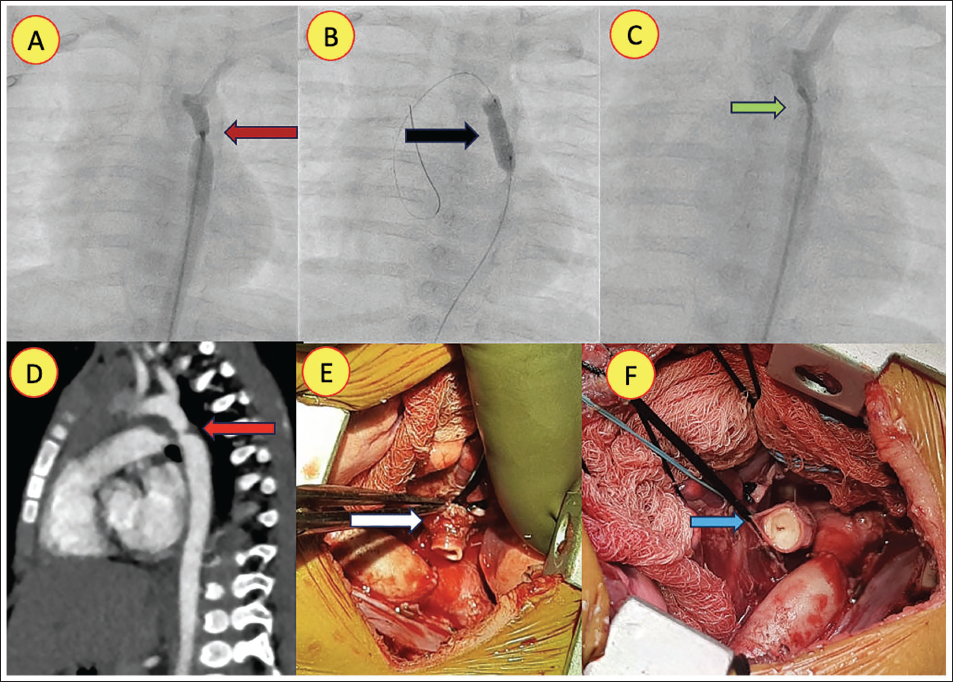
(A) Aortic Angiogram Demonstrating Severe Coarctation (Maroon Arrow). (B) Aviator Plus Balloon Inflated Across the Coarctation Segment (Black Arrow). (C) Post-angioplasty Angiogram Showing a Widened Segment with a Small Residual Waist (Green Arrow). (D) Computed Tomographic Aortogram (Lateral View) Revealing Severe Re-coarctation (Red Arrow). (E) Perioperative Image Showing the Resected Coarctation Segment (Side-on View, White Arrow). (F) En-face View of the same Segment, Demonstrating a Pinhole-like Luminal Opening (Blue Arrow).
(A) Aortic Root Angiogram Demonstrating a Doming Aortic Valve with a Narrow Antegrade Jet Consistent with Severe Aortic Stenosis (Maroon Arrow). (B) Aviator Plus Balloon Inflated Across the Aortic Valve During Temporary Pacing (Orange Balloon, Black Pacing Lead Arrow). (C) Post-valvotomy Angiogram Showing a Widely Opened Valve with Improved Antegrade Flow (Green Arrow).
Procedural details are summarized in Tables 1 and 2. Arterial access was achieved using either a 4F Terumo radial sheath for single-balloon procedures or a 4/5F Terumo Slender sheath for two-balloon procedures. The femoral vessel of one patient was very small, and gentle dilatation with a 4F dilator was done before taking the balloon (Figure 1A). Two patients were treated with a single 6 × 20 mm Aviator Plus balloon, while two others required a two-balloon technique with a 6 × 20 mm and a 7 × 20 mm Aviator Plus balloon (Figures 1B; 3B; 4B). Repeat balloon dilations were performed as needed, using the same or the next larger balloon size, guided by residual gradient assessment and confirmed with post-dilation angiography. All procedures were successfully performed. The mean pre-procedural coarctation gradient in the three patients was 38 ± 5.29 mmHg, which was reduced to a mean post-procedural gradient of 15 ± 4.35 mmHg. The mean fluoroscopy time for the procedures was 7.7 ± 5.06 min. One infant underwent balloon aortic valvotomy with a significant reduction in the gradient from 39 to 26 mmHg (Figures 4B, 4C). Peri- and post-procedure angiogram and echocardiogram showed significant opening of the narrow segment and improvement in the flow (Figures 1C, 1D; 2C, 2D; 3B, 3C). One patient experienced a transient intraprocedural complication of hypotension requiring supportive care. Another patient had pulse loss during the procedure, which was revived within 24 h after being given heparin.
The mean follow-up period was 8.5 ± 6.8 months. One infant who initially showed clinical improvement after balloon dilation for severe AS with documented post-intervention gradient reduction tragically died 4 months post-procedure due to progression of severe mitral regurgitation and intercurrent respiratory infection, rather than any balloon dilatation-related complication or procedural adverse event. Another infant developed restenosis 7 months after the procedure, despite an initial reduction in gradient, and subsequently underwent successful surgical repair. During surgery, a tight coarctation segment with a prominent shelf was identified and resected, followed by end-to-end anastomosis (Figures 2E-H; 3D-F).
Discussion
Severe left heart obstructive lesions in infancy, such as native CoA and critical valvular AS, remain among the most challenging conditions in pediatric cardiology. In neonates and young infants under 3 months of age, surgical repair continues to be the preferred strategy for severe coarctation. Nevertheless, balloon angioplasty has emerged as a valuable therapeutic alternative, particularly for critically ill neonates, in resource-limited settings, or as a palliative bridge to surgery.3-5 Evidence suggests that balloon angioplasty achieves meaningful acute gradient relief with acceptable mid-term durability, although restenosis rates are higher in neonates and younger infants.3, 4 Beyond the neonatal period, especially in cases of discrete coarctation, outcomes approach those of surgical repair.5, 6 Balloon valvuloplasty, in contrast, is widely accepted as the first-line therapy for isolated severe valvular AS in infants.7, 8
A key determinant of procedural success in this population is the choice of balloon. The ideal balloon for neonatal or infant angioplasty should combine a low crossing profile (to enable delivery through 4F and 4/5F Slender Glide sheaths), a broad range of diameters and lengths, compatibility with fine guidewires, and reliable trackability. Additional features such as radiopaque markers for precise positioning, rapid inflation and deflation to minimize hemodynamic compromise, and low- or non-compliant material to ensure predictable expansion without vascular injury are critical. High burst pressure tolerance, controlled waist formation, and resistance to rupture further enhance procedural safety in this fragile age group.9, 10
Off-label adaptation of balloon systems remains common in neonatal and infant catheterization because commercially available pediatric-specific platforms are limited in size range and availability. Published series consistently identify Tyshak and Tyshak II balloons (NuMED) as the most widely used platforms in infants, owing to their favorable balance of profile, wire compatibility, and rated burst pressure, which is typically sufficient since most lesions yield at ≈3 atm.5,6,11-13 The Tyshak Mini variant extends utility in very small infants with even lower profiles (3-4 Fr compatibility) and diameters down to 4 mm.6, 11, 12 Other low-profile balloon systems, such as Trek (Abbott), which is available up to 5 mm in diameter, and Sterling (Boston Scientific), which offers a broader size range, have also been used, though less frequently. 5 For resistant or fibrotic lesions, higher-profile, non-compliant balloons such as PowerFlex (Cordis), Z-Med II (NuMED), or Cook ATB (Cook) may be necessary, but their larger sheath and wire requirements limit application in small infants.5, 6 Collectively, the literature supports Tyshak/Tyshak Mini as first-line tools, with high-pressure devices reserved for refractory lesions.
Against this background, the present series introduces the Aviator Plus balloon as an off-label cost-effective alternative in infants with left heart obstructive lesions. The Aviator Plus balloon is originally meant for peripheral angioplasty with special reference to carotid and renal arteries.1, 2, 14 All four procedures—three coarctations and one critical AS—were successfully completed with significant gradient reduction (mean decrease in coarctation gradient from 38 ± 5.29 to 15 ± 4.35 mmHg) and no major procedural complications. The ability to deliver the Aviator Plus through 4F and 4/5 Slender Glide sheaths facilitated access in small-caliber vessels, while its handling characteristics and rapid inflation–deflation kinetics enabled effective lesion dilation with short fluoroscopy times. Minor access-related complications and transient hypotension were managed conservatively, reflecting an acceptable safety profile. Restenosis after balloon angioplasty is a recognized limitation in infants, particularly in the first year of life, and has been reported across several published series.5, 6 In this case, angioplasty was undertaken as a staged or temporizing strategy after multidisciplinary evaluation, with surgery anticipated if re-obstruction developed. One late death was attributable to progression of mitral regurgitation and intercurrent infection, not the balloon procedure.3-5
In selected circumstances, the technical attributes of the Aviator Plus may permit its use in infants when appropriately sized, although established low-profile balloons such as the Tyshak and Tyshak Mini continue to represent first-line platforms in this age group.5, 6 Its low profile, high burst pressure, superior pushability, and rapid exchange system make it particularly suited for delicate infant anatomy.1, 2 In comparison to Tyshak/Tyshak Mini, it offers higher-pressure capacity, which may assist in resistant or fibrotic lesions, though supporting data remain limited in infants. 15 Unlike coronary balloons, whose shaft length and limited diameter range restrict utility in this age group, the Aviator Plus bridges the gap by combining high-pressure performance with appropriate lengths and sheath compatibility for infants. The availability of a 4/5 Slender Glide sheath comes as an additional support for the use of a larger Aviator balloon while remaining gentle to the arteries and reducing risk. 16 In our setting, the lower cost and ready availability of the Aviator Plus balloon facilitated its consideration in selected infants, although cost considerations alone should not supersede clinical judgment or existing evidence. The requirement for a 5F introducer sheath with larger balloons can be mitigated by using a 4/5 Terumo Slender sheath, which provides the functional profile of a conventional 4F sheath and is less traumatic to the vessel. This platform contributed to successful dilation in this limited cohort, but established low-pressure systems remain first-line in infants. This report reflects an early single-center experience with balloon dilation in infants, undertaken in a setting where case frequency and hardware availability are limited, and procedural selection often requires individualized consideration.
This early experience suggests that the Aviator Plus balloon may serve as an additional option in carefully selected infants with left heart obstruction, particularly where device choice is constrained. While surgical repair remains the preferred and definitive strategy for CoA in neonates and young infants, several contemporary series have demonstrated that balloon angioplasty may represent a reasonable alternative in selected infants beyond 3 months of age, particularly as a temporizing or stabilizing intervention.5, 6 In our practice, the decision to proceed with balloon dilation was undertaken after multidisciplinary review with the congenital surgical team and in consultation with the family, with the understanding that surgery remained the standard of care and angioplasty was used only in selected cases where it was deemed clinically appropriate. This series supports the concept that, in selected infants, a high-pressure, low-profile balloon such as the Aviator Plus may provide an additional option alongside well-established platforms like the Tyshak and Tyshak Mini. While our early procedural results are encouraging, this experience represents only an initial feasibility signal. Importantly, neither of the two adverse outcomes was attributable to balloon failure or procedural complication, and no vascular injury, aneurysm, or balloon-related sequelae were observed. In settings where case volumes are small and equipment options remain limited, early experience—even with small numbers—may help broaden procedural familiarity and inform future adoption. Larger studies with more diverse patient groups—including critically ill neonates—and extended follow-up will be essential to confirm long-term durability, assess the risk of restenosis, and define the comparative role of the Aviator Plus balloon alongside surgery and established balloon systems.
Limitations
This study has several inherent limitations. Being retrospective, it is susceptible to documentation gaps and unmeasured confounders. The small sample size restricts the generalizability of the findings. Selection bias cannot be excluded, as all patients with left heart obstructive lesions were evaluated, selected, and treated by a single lead operator at a single center. Although the procedural success and safety outcomes are encouraging, larger, multicenter prospective studies with standardized selection criteria, procedural protocols, and long-term follow-up are required to validate these findings and establish broader applicability. Given the very small sample size, this series cannot estimate restenosis incidence, nor were long-term durability or comparative outcomes assessable.
Conclusion
This case series provides an early single-center experience with off-label use of the Aviator Plus balloon for the relief of left heart obstruction in infants. In this small cohort, the balloon could be delivered safely through small-caliber vessels and achieved immediate gradient reduction in coarctation and AS. Although one patient required subsequent surgical repair and another experienced a late death from non-procedural causes, no adverse outcome was attributable to device performance or catheter-based complications.
The findings underscore the potential feasibility of the Aviator Plus balloon as an additional catheter-based option in carefully selected infants, particularly in settings where pediatric-specific devices are limited, and balloon therapy is being used as a stabilizing or temporizing strategy. Established platforms, including the Tyshak family, continue to represent first-line choices for this age group, and surgery remains the standard treatment for coarctation in young infants. Larger multicenter cohorts with longer follow-up will be required to clarify durability, quantify restenosis risk, and define how the Aviator Plus balloon may fit alongside surgery and existing balloon systems in the management of left heart obstructive lesions in infancy.
Footnotes
Acknowledgments
The authors extend their sincere appreciation to the staff of the Pediatric and Congenital Heart Disease Department, Ms. Moumita Sil (Cardiology Technician), Ms. Pratima Hembram (Nursing Coordinator), and Ms. Mandira Mondal and Ms. Susmita Roy (OPD Coordinator) for their invaluable assistance with patient assessment and data collection. They express their deepest gratitude to the Department of Cardiology and Catheterization Laboratory Services, cardiothoracic surgery, IT service, and the Manipal Hospital authority for their unwavering support throughout the study. We are particularly grateful to the Dr. Anil Singhi Foundation for their generous academic support of our scientific research endeavors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Patient Consent
This scientific work adhered to the approved protocol of the Institutional Clinical Ethics and Research Committee (CERC/2021/Jun/iv). Patient confidentiality was ensured by anonymizing all data used in images and analysis. The ethics committee protocol waives the requirement for individual patient consent for anonymous record-based analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.