
Abstract
Quadricuspid valve is an extremely rare congenital cause of aortic regurgitation (AR). There are seven types of valves based on the size of the four cusps. They are associated with septal defects and ostial coronary abnormalities, which have important treatment implications. Ross procedure is a viable treatment option in young patients who present without aortopathy.
Brief Introduction
The causes of aortic regurgitation (AR) in childhood are most commonly rheumatic heart disease, bicuspid aortic valve, and subaortic membrane. Rarely, patients can present with quadricuspid aortic valve in the first and second decades of life, with associated aortic regurgitation and aortopathy. We present one such case of quadricuspid aortic valve with severe AR, discuss the Hurwitz classification system, and the treatment options available in such patients.
Case Presentation
A 14-year-old girl presented to the emergency department with palpitations for 2 years and dyspnea on exertion (NYHA-II) for 2 months. The palpitations were of volume overload type and not associated with presyncope or syncope. She also perceived a throbbing sensation in the neck. She did not have orthopnea or paroxysmal nocturnal dyspnea (PND) episodes. She did not have any significant family history.
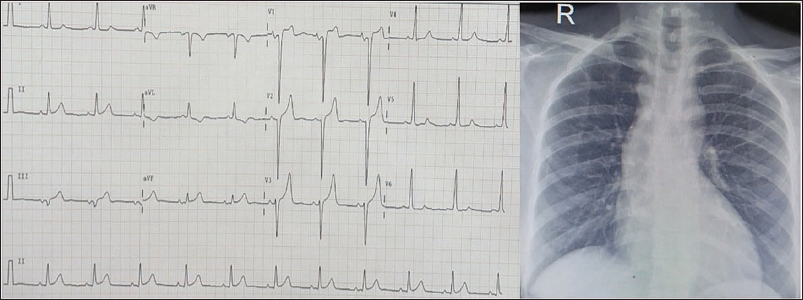
On examination, she had bounding pulses, wide pulse pressure (blood pressure of 110/40 mmHg), and a prominent holodiastolic murmur in the left third intercostal space. Peripheral signs of severe aortic regurgitation, including dancing carotids, Landolfi sign, and pistol shot femoral sounds, were present. A 12-lead electrocardiogram was suggestive of left ventricular hypertrophy of volume overload type. Chest X-ray did not reveal obvious cardiomegaly. However, the ascending aorta was dilated (Figure 1).
Electrocardiogram (ECG) Showing Left Ventricular Hypertrophy (LVH) With Volume Overload Type Pattern. Chest X-ray Showing Dilated Ascending Aorta, Without Obvious Cardiomegaly.
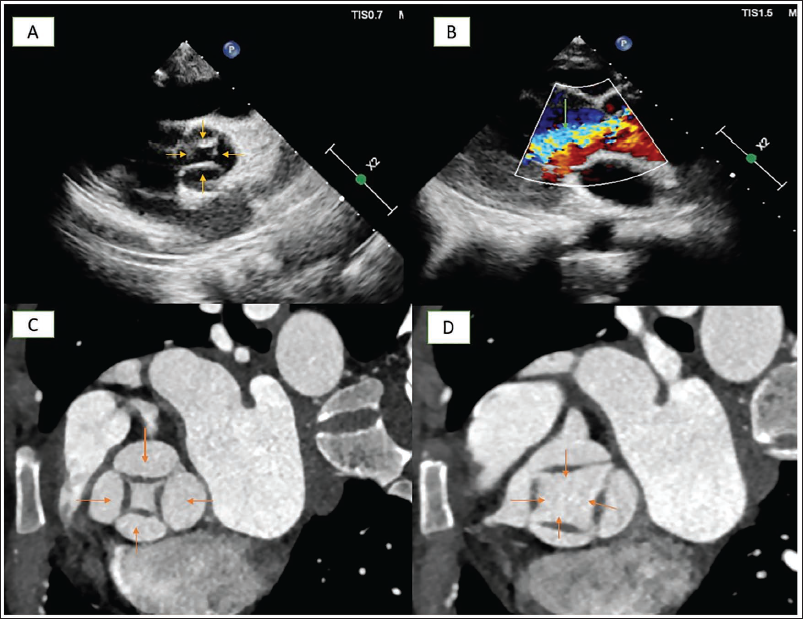
Bedside echocardiography in the parasternal short-axis view revealed a suspicious quadricuspid aortic valve (Panel A). Parasternal long-axis view revealed severe eccentric aortic regurgitation (Panel B) with vena contracta of 6 mm. Cardiac computed tomography confirmed the presence of a quadricuspid aortic valve (Panels C and D) in both systole and diastole. Her coronary arteries were normal (Figure 2).
Panel A Shows Four Aortic Cusps (Yellow Arrows) in Parasternal Short-Axis View. Panel B Shows Severe Aortic Regurgitation (Green Arrow) in Parasternal Long-axis View. Panels C and D Show a Quadricuspid Aortic Valve (Red Arrows) in Both Systole and Diastole.
Discussion
The most common causes of aortic regurgitation in children are bicuspid aortic valve, rheumatic heart disease, and subaortic membrane. However, in this case, there is no thickening of valve leaflets suggestive of rheumatic heart disease. Similarly, there is no subaortic membrane. The aortic regurgitation is at the valvular level due to a quadricuspid aortic valve. Quadricuspid aortic valve is an extremely rare congenital cause of aortic regurgitation with an incidence of 0.013%. 1 It occurs more commonly in females, usually presenting in the fourth decade of life. 2 Interestingly, there is no significant survival difference between quadricuspid and non-quadricuspid aortic valve populations when matched for sex and age. 1
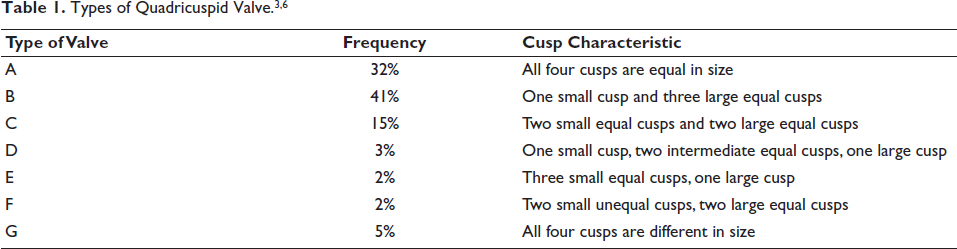
There are seven subtypes in the Hurwitz system used for classification based on the relative sizes of the four cusps, with type A being the most common. 3 Our patient has a type G valve with four unequal cusps (Table 1). A second classification, known as Nakamura’s classification, is based on the position of the supernumerary cusp in relation to the left, right, and noncoronary cusps. 4
Quadricuspid valve is associated with aortic dilation, atrial and ventricular septal defects, myxomatous changes of the mitral valve, subaortic stenosis, and coronary anomalies.1, 2, 5 The most common among these associations is abnormality of the coronary arteries and ostium, which is found in about 10% of these patients. 1 The initial step in diagnosis is the visualization of four cusps during echocardiography. Computed tomography (CT) angiography is usually performed as additional important information about the coronaries can be deduced, which has important management implications.
This patient had significant left ventricular (LV) dilatation and an ejection fraction of 45% without aortopathy and other associated anomalies. She was stabilized with diuretics and planned for Ross procedure.
To conclude, quadricuspid aortic valve is a very rare cause of aortic regurgitation in childhood and adolescence. Echocardiographic and computed tomography assessments are crucial to confirm the diagnosis and identify associated anomalies. Valve repair and Ross procedure are the preferred options, while valve replacement is reserved for cases where the valve apparatus is severely distorted.
Footnotes
Data Availability Statement
All data are incorporated into the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable as it is an anonymous case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Obtained from the patient in line with COPE guidance.