
Abstract
Quadricuspid aortic valve (QAV) is a rare congenital anomaly with <200 cases reported to date. Most patients are asymptomatic. Symptoms depend on the functionality of the valve and associated heart defects, most often presenting as aortic regurgitation followed by aortic stenosis. Management guidelines are ill-defined. We present two cases of QAV with rare associations (ventricular septal defect) and variable clinical presentation.
Background
Quadricuspid aortic valve (QAV) is a rare congenital heart disease with an incidence of 0.04% in echocardiographic series with <200 cases reported to date.1, 2 The majority of patients are asymptomatic, with a minority developing aortic regurgitation (AR) later in life. 1 QAV may be rarely associated with other congenital anomalies. 3 We present two cases (Table 1) of QAV with rare associations and variable clinical presentation.
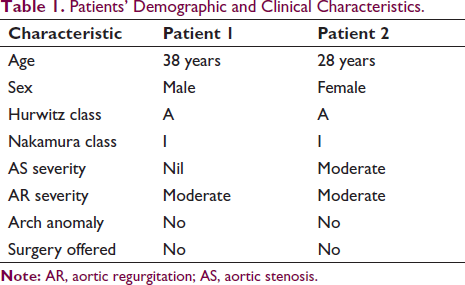
Patients’ Demographic and Clinical Characteristics.
Case 1
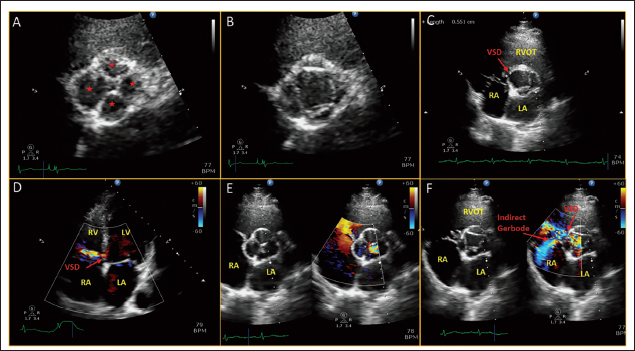
A 38-year-old male, known to have had ventricular septal defect (VSD) from the 16 years of age, was noted to have moderate AR on follow-up. The left ventricle was mildly dilated (end-systolic diameter 39 mm) with normal left ventricular function and proximal aortic dimensions. A closer look at the aortic valve showed that the valve was quadricuspid (Figure 1A and B) with moderate AR (Supplementary Figure 1) and mild prolapse of the right coronary cusp (Figure 1C). The subaortic ventricular septal defect was small with an interventricular gradient of 80 mm Hg, indirect Gerbode effect (Figure 1D–F) and no pulmonary hypertension. All four leaflets were of similar size. The patient was kept on close medical follow-up.
Case 2
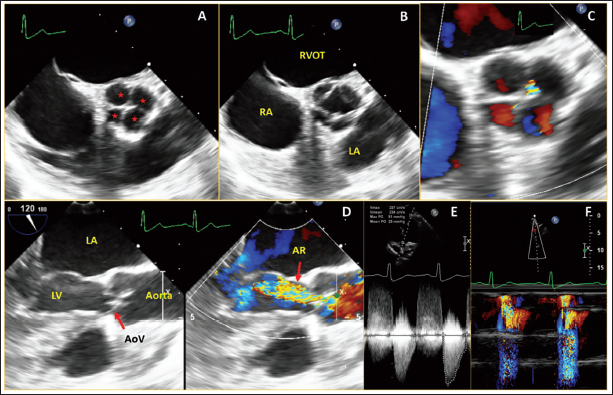
A 28-year-old female, was evaluated for cardiac murmur. Echocardiography showed moderate aortic stenosis (AS), and mild AR with a nondilated left ventricle. Transesophagal echocardiogram (TEE) showed quadricuspid aortic valve (Figure 2A and B) and moderate AS with AR [AS mean gradient 25 mm Hg, peak velocity 3.51 m/s, early diastolic flow reversal in descending thoracic aorta] (Figure 2C–F). All four leaflets were of similar size. We suggested a medical follow-up.
Discussion
Quadricuspid aortic valve is usually an isolated anomaly, but other congenital heart defects can be associated in 18%–32% of the patients, including coronary artery and coronary ostium anomalies, atrial septal defect (ASD), VSD, patent ductus arteriosus, tetralogy of Fallot, sinus of Valsalva fistula, subaortic fibromuscular stenosis, mitral valve prolapse, hypertrophic nonobstructive cardiomyopathy, and transposition of great arteries.1, 3, 4 Identification of this entity has improved due to the extensive use of transesophageal echocardiography to characterize valve anomalies before repair. The speculated mechanisms of development of QAV include inflammation causing separation of valve cushion, anomalous septation, or anomalous coronary development leading to leaflet anomalies.5, 6
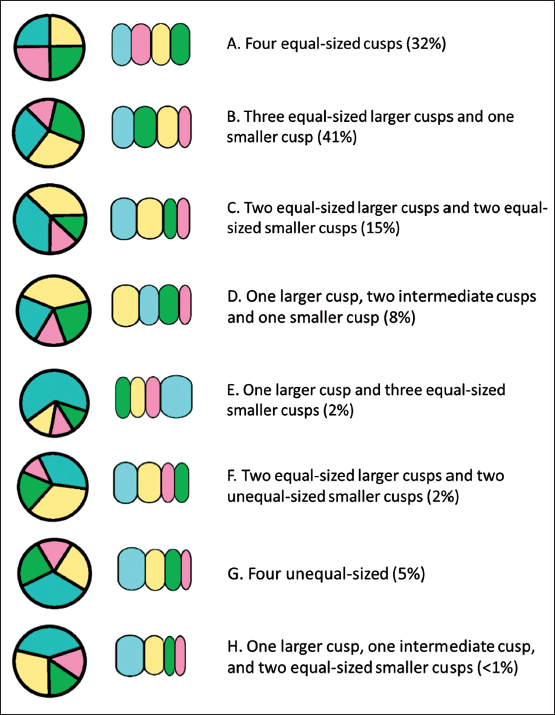
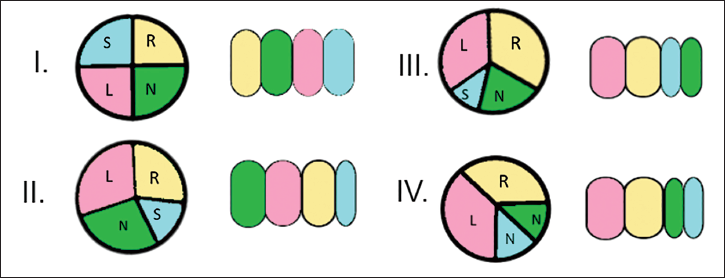
Based on the relative size of the supernumerary cusp Hurwitz and Roberts have classified QAV (Figure 3) into seven types from A to G, to which a type H has been added. 3 Types A to C represent more than 85% of cases. A simplified classification (Figure 4) depending on the position of the supernumerary cusp has been developed later. 5 TEE can give accurate information regarding morphology and coronary ostia. Clinical manifestation of QAV is variable with the commonest presentation being AR in 75% of cases, AS and AR in 9%, and normal functioning valve in 16% of cases. Aortopathy is not reported to be associated with QAV.
Classification of QAV according to leaflet morphology, adopted from Hurwitz & Roberts 3 classification of quadricuspid aortic valve with Vali et al. supplement.
Debates remain in the management strategies of the patients with a QAV in terms of surgical indication, surgical procedure of choice, and antibiotic prophylaxis against infective endocarditis. The functional status of QAV is predominantly pure AR, although stenosis may develop at a later stage. The temporal progression of AR and an association between morphological characteristics of QAV and the severity of AR have not been convincingly described. The occurrence of AR has been reported to be relatively less in type A. However, both our patients had type A QAV and AR. Progressive cusp fibrosis with subsequent failure of cusp coaptation over time has been suggested as the key mechanism in AR. During repair or replacement procedures, care should be taken to avoid coronary ostial obstruction.
Quadricuspid aortic valve with associated VSD is extremely rare in the literature. One case of QAV with a history of surgery for ASD in past was reported from Turkey in 2013 having four leaflets of differing sizes, mild AR and a membranous VSD (The authors decided to close this defect because the patient was symptomatic and pulmonary to systemic blood flow was higher than normal). 7 Two other cases were described in Mayo clinic series and one more in Hurwitz and Roberts et al.1, 3 series. Our justification to pursue medical management was based on the nonprogression of AR, mechanism of AR being central noncoaptation of leaflets rather than prolapse of the leaflet which usually mandates early surgery and the absence of significant VSD shunt.
Conclusion
Quadricuspid aortic valve is a rare diagnosis and the most appropriate course of management is yet to be established. Progression of AR usually mandates aortic valve replacement (AVR), along with closure of associated septal defects, if any. However, our cases represent symptom-free long-term survival with QAV in situations with nonprogressive AR and good left ventricle function justifying their follow-up medically.
Author Contribution
SM (Conceptualization: Equal; Formal analysis: Lead; Writing – original draft: Lead; Writing – review & editing: Lead).
DSK (Conceptualization: Equal; Investigation: Equal; Supervision: Equal ; Writing – original draft: Equal).
Footnotes
Data Availability Statement
No new data were generated or analyzed in support of this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statement
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The written informed consent was obtained.
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.