
Abstract
Coronary artery anomalies are uncommon and are most frequently identified incidentally during coronary angiography. Among these, the presence of a dual left anterior descending artery is relatively frequent, with an incidence of around 1%, whereas a double right coronary artery is uncommon. We describe the case of a 63-year-old male who presented with Class III angina. Coronary angiography revealed complex multivessel coronary artery disease with dual left anterior descending artery (Type A.2.1.2) and double right coronary artery (Type G2). The patient underwent coronary artery bypass grafting performed with the aid of cardiopulmonary bypass. Complete myocardial revascularization was performed by anastomosing the left internal mammary artery to the septal left anterior descending artery, along with reversed saphenous vein grafts to obtuse marginal branches 1 and 2, and the second right coronary artery. This case underscores the simultaneous presence of two rare coronary anomalies in a single patient undergoing surgical coronary revascularization. To the best of our knowledge, this may be the first reported case to undergo surgical revascularization. Recognition of such variants is essential to ensure complete revascularization and prevent postoperative ischemia.
Keywords
Introduction
Coronary artery anomalies are infrequent and are typically discovered incidentally during coronary angiographic evaluation or at postmortem examination, with an incidence ranging from 0.24% to 1.3% in large angiographic series of over 70,000 patients. 1 These anomalies usually pertain to variations in the origin or anatomical course of the coronary arteries, with separate ostial origins of the left anterior descending artery (LAD) and left circumflex artery representing the most common pattern. While many coronary anomalies are hemodynamically insignificant, their identification becomes crucial in patients undergoing myocardial revascularization. Accurate recognition facilitates appropriate surgical planning, optimal graft selection and placement, and helps prevent incomplete revascularization. A double right coronary artery (RCA) represents a rare coronary anomaly and is generally regarded as a benign variant, but it may still be susceptible to atherosclerotic disease. 2 The coexistence of a double RCA with other anomalies, such as a dual LAD, is extremely rare and may complicate both diagnosis and revascularization. We present the report of a 63-year-old man with complex multivessel coronary artery disease and the rare coexistence of a dual LAD and a double RCA, an unusual anatomical combination that was successfully managed with coronary artery bypass grafting (CABG). This report highlights the importance of recognizing such anomalies to avoid incomplete revascularization with subsequent risks of residual ischemia, postoperative angina, and graft failure due to inappropriate target selection. The requirement for patient consent was waived in view of the retrospective nature of this report.
Case Report
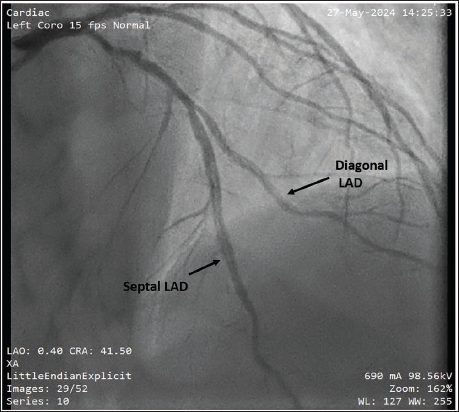
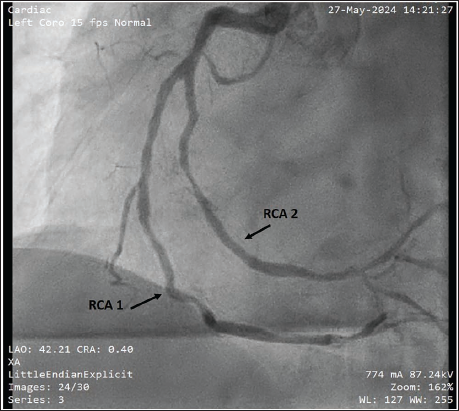
A 63-year-old man presented with a 2-week history of exertional dyspnea and chest discomfort, indicating marked limitation of physical activity. His past medical history included hypertension and diabetes mellitus, both diagnosed 5 years earlier, along with long-standing bronchial asthma. On examination, blood pressure was 140/80 mmHg and heart rate 68 beats per minute. A treadmill stress test demonstrated inducible ischemia. Transthoracic echocardiography demonstrated concentric hypertrophy of the left ventricle accompanied by mild (Grade I) diastolic dysfunction. Coronary angiography revealed multivessel disease and two anomalies: a dual LAD, Type A.2.1.2 (Sajja classification) (Figure 1), 3 and a double RCA, Type G2 (Acet classification) (Figure 2). 4 Significant stenoses were noted in the septal LAD, two obtuse marginal branches, and RCA 2, the dominant vessel.
Dual Left Anterior Descending Artery (LAD), Type A.2.1.2 of Sajja Classification.
Double Right Coronary Artery (RCA) (Acet Type G2).
The patient underwent elective CABG with the aid of cardiopulmonary bypass (CPB) and del Nido cardioplegia for myocardial protection. Myocardial revascularization was performed by anastomosing the left internal mammary artery to the septal LAD, complemented by reversed saphenous vein grafts to the obtuse marginal branches, and RCA 2. Intraoperatively, two RCAs were visualized in the atrioventricular groove, lying superimposed. RCA 2 was dominant, coursing deeply and giving rise to both the posterior descending and posterolateral branches. Arteriotomy was performed distal to the stenotic segment, with graft placement confirmed by coronary probing. RCA 1 was found to be nondominant and free of critical stenosis, and hence was not grafted. Intraoperatively, dominance was confirmed by tracing the posterior descending artery (PDA) origin, which arose from RCA 2, establishing right dominance. Intraoperatively, both LAD branches were carefully dissected, and the septal LAD was identified within the anterior interventricular groove. The diagonal LAD had a more lateral course without entering the groove, consistent with preoperative imaging. The presence of two parallel RCAs within the right atrioventricular groove required careful separation to avoid graft misplacement. No significant technical difficulties in accessing the targets were encountered, although differentiation of RCA 2 from RCA 1 intraoperatively required direct flow assessment and anatomical tracing. The patient’s postoperative recovery was smooth and uncomplicated, and he was discharged on the fifth postoperative day.
Discussion
Coronary artery anomalies are typically identified incidentally during coronary angiographic evaluation. A dual LAD is observed in approximately 1% of patients; however, its concomitant presence with a double RCA is exceedingly uncommon. 2 These anomalous arteries may also develop atherosclerotic disease, necessitating surgical or percutaneous revascularization. 5 Reports of revascularization in such cases are few, and surgical management of combined dual LAD and double RCA highlights the importance of meticulous preoperative imaging.
Precise recognition of coronary anatomy is crucial for the correct placement of the arteriotomy and the graft. Therefore, careful preoperative imaging and intraoperative verification are essential to reduce perioperative morbidity. In double RCA, the vessel giving rise to the PDA is considered dominant and requires grafting to achieve complete myocardial perfusion. Classification systems describing morphological variants of dual LAD and double RCA support surgical planning and intraoperative decision-making.3, 4 In our case, the dual LAD originated from a common trunk, with the diagonal LAD coursing leftward without entering the anterior interventricular groove (Sajja Type A.2.1.2). The double RCA (Acet Type G2) arose from a single right aortic sinus and divided into two branches running parallel and superimposed within the atrioventricular groove toward the posterior interventricular sulcus. Lack of recognition may result in grafting only the superficial RCA while missing the deeper dominant vessel, leading to incomplete revascularization. To our knowledge, there are no published case reports describing the coexistence of both dual LAD and double RCA in a single patient undergoing CABG. While isolated reports of each anomaly exist, this case underscores a rare anatomical constellation that may pose cumulative challenges in diagnosis and revascularization strategy.
In cases where the septal LAD is difficult to identify intraoperatively, techniques such as intraoperative Doppler assessment, use of epicardial echocardiography, or tracing from anatomical landmarks (e.g., pulmonary artery root) may assist in localization. Similarly, in the setting of double RCA, flow assessment and ST-segment changes during cardioplegia administration or off-pump may guide the decision to graft both branches, particularly if electrocardiography (ECG) changes or regional wall motion abnormalities are noted.
Conclusion
Accurate recognition of coronary artery anomalies is vital in surgical planning to prevent errors and achieve complete myocardial revascularization.
Footnotes
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study complies with the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Committee with the reference number SH/IEC/M/03/2023-2024/001.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed consent was waived by the Institutional Ethics Committee due to the retrospective nature of the case report.