
Abstract
Ruptured sinus of Valsalva aneurysms are rare congenital anomalies that can lead to significant hemodynamic compromise, thus requiring urgent intervention. This case series describes three successful transcatheter closures of large ruptured sinus of Valsalva defects (>10 mm) using dual-device deployment techniques when single devices failed due to prolapse or residual shunts. Cases involved ruptured sinus of Valsalva from the noncoronary cusp to the right atrium and the right coronary cusp to the right ventricular outflow tract, with complete occlusion achieved using combinations of Cocoon duct occluders and muscular ventricular septal defect occluders, demonstrating the feasibility and safety of percutaneous approaches in suitable anatomies.
Introduction
Sinus of Valsalva aneurysms originate from the aortic root above the aortic valve annulus and may rupture into adjacent cardiac chambers, causing acute heart failure due to left-to-right shunting. Ruptured sinus of Valsalva accounts for 0.1%-3.5% of congenital cardiac anomalies, with rupture typically occurring in the 3rd or 4th decade, often precipitated by exertion or trauma in patients with underlying connective tissue weakness. Surgical repair has been the traditional gold standard, but transcatheter closure has emerged as a less invasive alternative for isolated defects with favorable anatomy, offering shorter recovery and reduced morbidity.
Case Report
Case 1
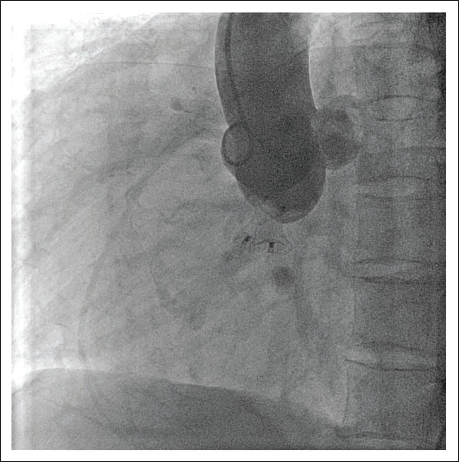
A 35-year-old male, a chronic smoker, presented with the sudden onset of chest pain following lifting a heavy object. His chest pain subsided, but after that, he started feeling a continuous superficial vibration near the sternum. On examination, the patient had a large volume pulse with increased pulse pressure and a continuous thrill in the right third and fourth parasternal region. There was a continuous murmur of grade 4/6 with a prominent systolic component in the right third and fourth intercostal spaces on auscultation. Echocardiography was done, which revealed the presence of a large ruptured sinus of Valsalva (RSOV) from the noncoronary sinus to the right atrium (RA), measuring about 10 mm at the neck of the windsock at the aortic end (Figure 1). The patient was then planned for transcatheter device closure. Using a 5F pigtail catheter, an aortogram was done through the femoral arterial approach in left anterior oblique (LAO) 60 (Figure 2) and right anterior oblique (RAO) 30, which showed a large rupture of the sinus of Valsalva from the noncoronary cusp (NCC) to the RA. Using a 6F Judkins Right (JR) catheter and 0.035” hydrophilic wire (Terumo Inc., Japan), the RSOV defect was successfully crossed from the arterial side to the RA and placed in the inferior vena cava (IVC). The wire was snared through the venous side, creating an arteriovenous (AV) loop over which a 5F JR was crossed from the venous side and placed in the descending aorta. The wire was exchanged with 035 extra stiff wire. A 12F Cook sheath was introduced into the aorta, through which a 12/14 mm Cocoon duct occluder was deployed (Vascular Innovations, Thailand). However, the device prolapsed into the RA, and the windsock was not fully occluded by the device. The defect was closed using two devices: a 12/14 Cocoon duct occluder and an 8/10 Cocoon duct occluder were deployed simultaneously (Figure 3). Angiography done post-procedure showed no residual shunt or aortic regurgitation (Figure 4).
Image Showing Parasternal Short Axis View Using Transthoracic Echocardiogram with Slight Angulation to Show the Classical Windsock Appearance (Yellow Arrow) of the Ruptured Sinus of Valsalva Involving Noncoronary Sinus into the Right Atrium.
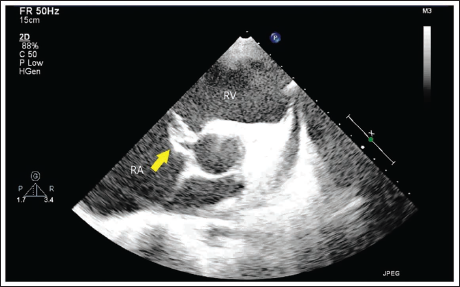
Image Showing Pigtail Aortogram in Left Anterior Oblique (LAO) View Demonstrating Shunt (Yellow Arrow) Across the Noncoronary Sinus to the Right-sided Chamber.
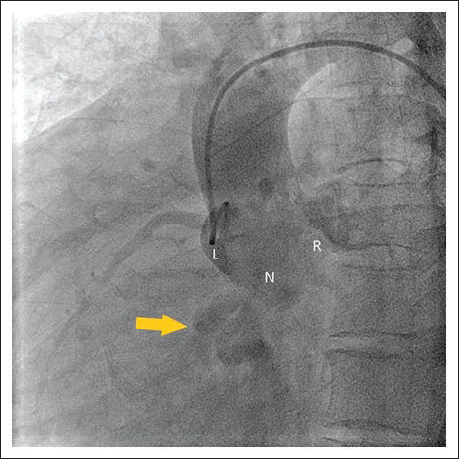
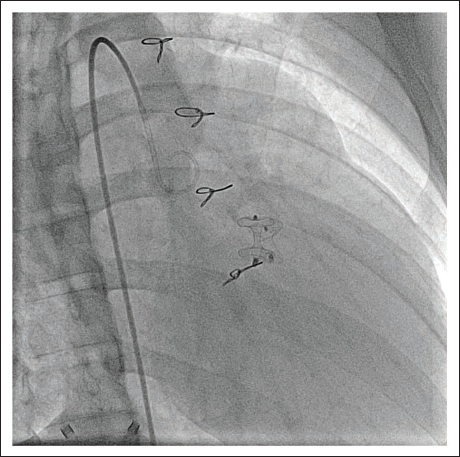
Image Showing Pigtail Aortogram in Left Anterior Oblique (LAO) View When Both the Cocoon Duct Occluder Devices were Being Simultaneously Deployed.
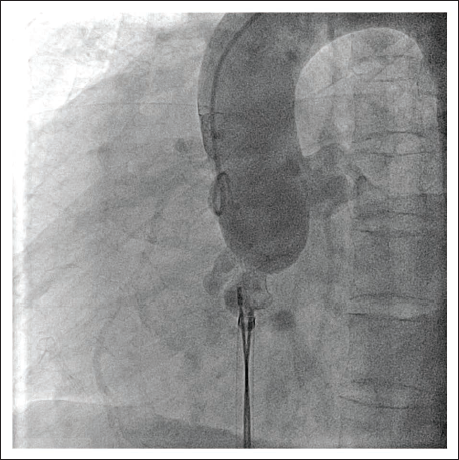
Image Showing the Final Pigtail Aortogram in Left Anterior Oblique (LAO) View with Both the Cocoon Duct Occluder Devices and No Residual Shunt Across the Sinus of Valsalva Aneurysm.
Case 2
A 17-year-old male with a history of surgical closure of a ventricular septal defect (VSD) in childhood with a patch presented with chest discomfort for the past 1 month, following an accident. The electrocardiogram was normal, and on auscultation, a grade 3/6 continuous murmur was heard in the left second intercostal space with diastolic accentuation. Transesophageal echocardiography revealed the presence of a large defect in the sinus of Valsalva from the right sinus to the right ventricular outflow tract (RVOT), with an aortic end measuring 11 mm at the neck of the windsock at the aortic end (Figure 5). Using a 5F pigtail, an aortogram was done first. Then, using right femoral artery access and a 6F JR catheter and 0.035″ wire, RSOV was crossed, and the right ventricle was entered, and then the wire was placed in the pulmonary artery. Using the right femoral vein access, the wire was snared to create an AV loop. The wire was exchanged with a 0.035″ stiff wire, and an 8F sheath (Cook, USA) was taken via the RSOV defect into the aorta. Attempts were made to close the defect using two 6/8 Cocoon duct occluders, but they failed. Finally, the defect was closed with two devices, namely, an 8/10 mm Cocoon duct occluder and an 8 mm muscular VSD occluder, deployed simultaneously (Figure 6). Post-deployment angiography and echocardiography showed no residual shunt or aortic valve regurgitation (Figure 7). The RSOV, which protrudes into the RVOT, complicates wire crossing from the aorta. Proximity to the right coronary artery (RCA) ostium demands a >5 mm gap and confirmation via selective RCA angiography to avoid ostial obstruction, but in our case, the RCA ostium was more than 5 mm.
Image Showing Transesophageal Echocardiogram at the Mid Esophagus Level at 134° Showing Shunt Across the Posterior Aortic Sinus into the Right Ventricular Outflow Tract.
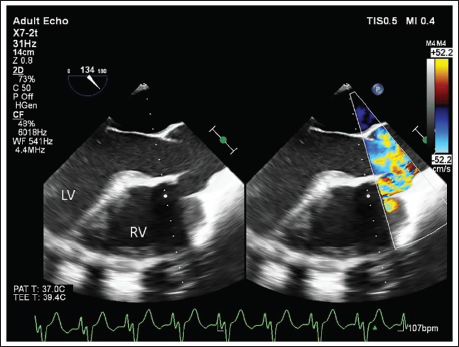
Image Showing Pigtail Aortogram in Right Anterior Oblique (RAO) View Demonstrating Shunt (White Arrow) Across Right Sinus to Right Ventricular Outflow Tract.
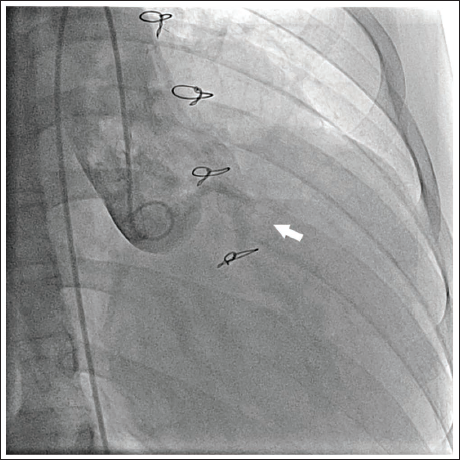
Image Showing Final Pigtail Aortogram in Right Anterior Oblique (RAO) View with the Two Devices Across the Right Sinus of Valsalva Aneurysm and with No Residual Shunt Across the Defect.
Case 3
A 23‑year‑old man presented with a sudden onset of dyspnea for 2 days, with orthopnea and no history of chest pain, fever, palpitations, or edema. Examination revealed tachycardia (116/min), blood pressure of 100/50 mm Hg, loud P2, a continuous murmur maximal at the aortic area with a thrill, and bilateral basal crepitations. The electrocardiogram showed sinus rhythm with normal axis and no ischemic changes.
Transthoracic echocardiography demonstrated a dilated left ventricle (LV) with no regional wall motion abnormality, a dilated RA, right ventricle, and pulmonary artery, and a 10 mm continuous flow jet from the noncoronary cusp of the aortic sinus into the RA, with moderate tricuspid regurgitation, consistent with an RSOV. In view of suitable anatomy and the absence of associated surgical lesions, percutaneous closure was planned.
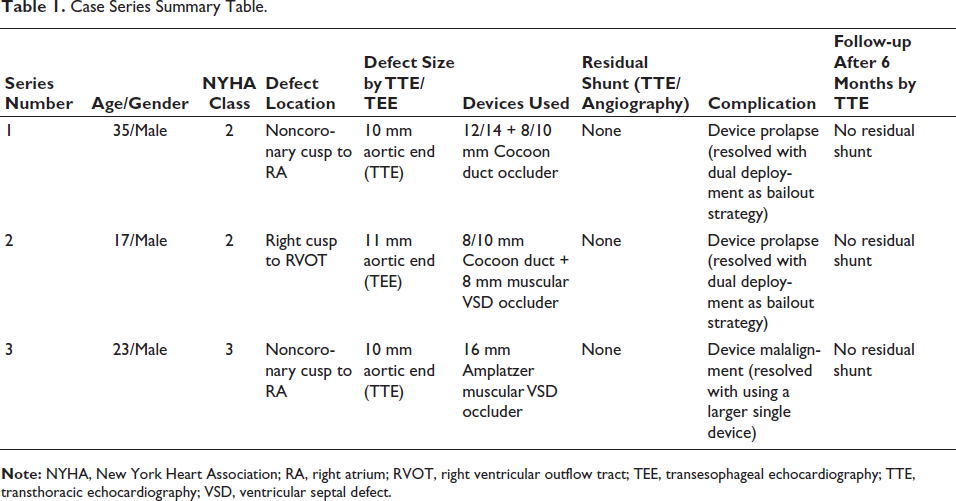
Case Series Summary Table.
Access was obtained via the right femoral artery and vein, the RSOV was profiled with a 6F pigtail catheter, and the defect was crossed from the aortic side using a 6F JR catheter and a straight Terumo wire, which was snared in the RA to form an AV loop. Patent ductus arteriosus occluder devices (8/10 and 12/14 mm) were initially used but resulted in malalignment and residual shunt, so a 16 mm Amplatzer muscular VSD occluder was deployed under angiographic and transthoracic echocardiographic guidance, achieving complete closure.
The patient’s symptoms improved immediately, with resolution of pulmonary congestion and stable hemodynamics. Follow‑up echocardiography showed a well‑seated device, no residual shunt, and no new aortic regurgitation, illustrating successful transcatheter management of RSOV from the noncoronary cusp to the RA.
Discussion
Transcatheter closure of RSOV aneurysms represents a viable alternative to surgical repair, particularly for large defects (>10 mm) with suitable anatomy, as demonstrated in this case series using dual-device deployment with Cocoon duct occluders and muscular VSD occluders. 1 Patient characteristics are summarized in Table 1.
Ruptured sinus of Valsalva ruptures often originate from the right or NCC into the RA or ventricle, causing acute hemodynamic instability, as seen in these young patients (ages 17-35) with continuous murmurs and shunts confirmed by echocardiography and aortography. Dual-device techniques succeeded where single devices prolapsed or left residual shunts, achieving complete occlusion without aortic regurgitation or procedural complications. 2 This approach aligns with reports favoring patent ductus arteriosus (PDA) or duct occluders for their conformity to the RSOV windsock morphology, enabling precise deployment via AV loops.3, 4
Dual devices were chosen as a bailout strategy when a single device did not completely occlude the shunt and to completely occlude the windsock without impinging upon nearby structures like the coronary ostium or the aortic valve. It can be used for large defects or proximity to critical structures like the aortic valve or coronary ostia. It can be used when a single RSOV is >10 mm with a Windkessel effect or tortuosity hindering a single-device fit.
Percutaneous methods offer shorter hospital stays, immediate extubation, and reduced morbidity compared to surgical patch closure under cardiopulmonary bypass.1, 5 Systematic reviews confirm high technical success (75%-95%) in selected cases, with mid-term follow-up showing New York Heart Association (NYHA) Class I status and minimal residual shunts.3, 6 Cocoon devices, coated with nano-platinum for biocompatibility, have proven effective even in very large defects up to 20 mm, supporting their use in bailout dual deployment.2, 7
Patient selection remains critical, excluding multilevel ruptures, significant aortic regurgitation, or endocarditis. 3 While short-term outcomes are favorable, long-term data (>5 years) on device durability and AR progression are limited, warranting extended surveillance. Larger multicenter series could validate dual-device strategies for complex RSOV anatomies.5, 8
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
Not needed since retrospective case analysis was done over 3-year period.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patients written consent obtained for publications.