
Abstract
Background:
Ruptured sinus of Valsalva aneurysm (RSOVA) is rare and can mimic many other diseases. It may be misdiagnosed on initial evaluation. Uncorrected almost invariably, it has a rapid downhill course. We present a case which was initially misdiagnosed as acute coronary syndrome (ACS).
Case Summary:
A 49-year-old lady presented to a local hospital with history of chest pain. She was diagnosed with ACS based on history and electrocardiogram findings and treated conservatively. She deteriorated and developed multiorgan failure. She was transferred to our center for further management. On re-evaluation, transthoracic echocardiography showed RSOVA. She was treated with transcatheter device closure. She recovered well and was discharged in stable condition.
Discussion:
This case highlights the diagnostic difficulty when patients present with features of other common diseases. Right heart failure evaluation in the setting of appropriate clinical features should prompt consideration of RSOVA as a differential diagnosis. RSOVA if managed appropriately can lead to complete recovery.
Introduction
Ruptured sinus of Valsalva aneurysm (RSOVA) is rare and can mimic many other diseases. It may be misdiagnosed on initial evaluation. Uncorrected, the rupture almost invariably causes deterioration in heart function and has a rapid downhill course. We present a case of 49-year-old lady whose diagnosis was missed initially and treated as acute coronary syndrome (ACS).
Case Report
A 49-year-old lady with no known comorbidities was admitted to another hospital with history of chest pain and dyspnea. She was diagnosed and treated for ACS based on history and electrocardiogram (ECG) findings. She developed tachycardia, hypotension progressing to multiorgan failure. She was referred to our multispecialty tertiary care hospital for further treatment. ECG was not sent with the patient.
Diagnosis
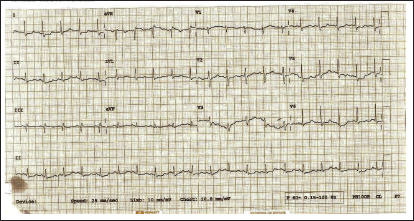
On arrival to our center, she was found to be dyspneic and had sinus tachycardia with heart rate of 120/min. She was hypotensive requiring noradrenaline infusion at 0.2 µg/kg/min. She had mild pitting pedal oedema with elevated jugular venous pressure. Auscultation revealed bibasal coarse crepitations. Grade III continuous murmur was heard best in the left sternal border. ECG showed ST depressions in lead I, II, aVL, and V4 to V6 (Figure 1). Investigations confirmed acute kidney injury (blood urea nitrogen levels 77.8 mg/dL [reference range 8-23 mg/dL], creatinine levels 7.8 mg/dL [reference range 0.8-1.6 mg/dL], acute liver injury (elevated total bilirubin levels 5.6 mg/dL [reference range 0.1-1.2 mg/dL], and direct bilirubin levels 3.29 mg/dL [reference range 0-0.4 mg/dL] with alanine aminotransferase levels 5,160 Units (U)/L [reference range 10-50 U/L], aspartate aminotransferase levels 5,941 U/L [reference range 5-37 U/L]), and coagulopathy (international normalized ratio of 3.5). Transthoracic echocardiography showed dilated right atrium (RA) and right ventricle (RV) and RSOVA with noncoronary cusp to RA shunt, mild aortic regurgitation (AR), mild tricuspid regurgitation, and pulmonary artery systolic pressure (PASP) of 50 mmHg (Figures 2-4). There was no clot or pericardial effusion and no regional wall motion abnormality. Her blood cultures were negative.
A 12-lead ECG showing ST depressions in lead I, II, aVL, and V4 to V6.
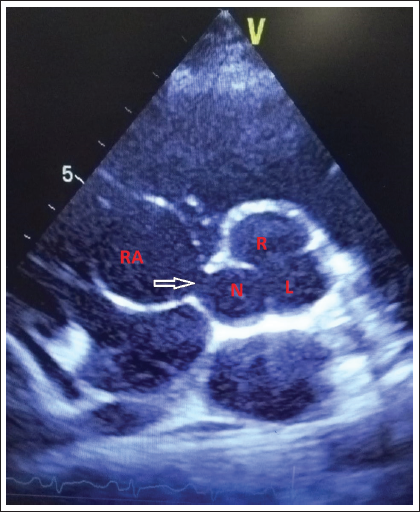
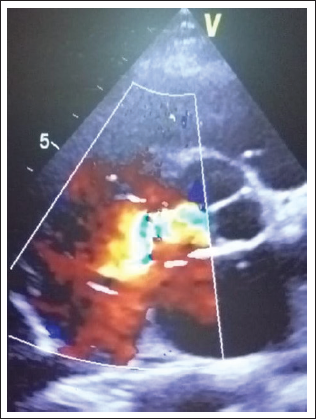
Color flow mapping of parasternal short axis transthoracic echocardiography demonstrating ruptured sinus of Valsalva arising from the noncoronary sinus and communicating with the right atrium.
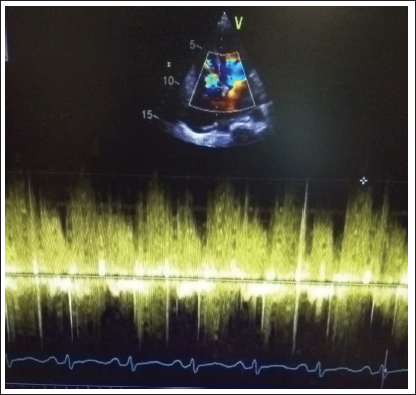
Spectral doppler demonstrating continuous flow across ruptured sinus of Valsalva into right atrium.
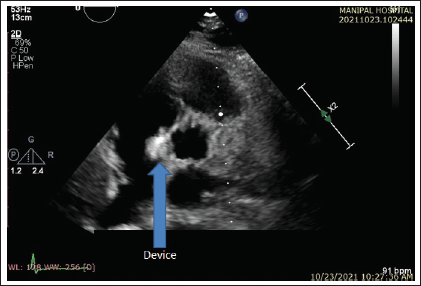
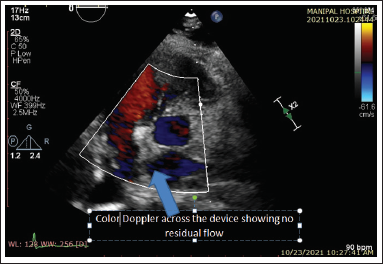
After discussion about risks and benefit on the background of unstable patient condition, patient and family chose percutaneous closure. She underwent transcatheter device closure of RSOVA following urgent cardiologist review. Procedure was performed through a left femoral artery approach with 12/10 Hifetech Patent Ductus Arteriosus closure device deployed across the RSOVA. Transthoracic Echocardiography (transesophageal echocardiography [TOE]) after the procedure showed no residual shunt or AR (Figures 5–6). Her PASP post procedure was 50 mmHg. After closure, her hemodynamic status rapidly improved and was weaned off vasoactive medications. She required tracheostomy to facilitate prolonged weaning from the ventilator. She was transferred to the ward on day 23. Her renal function recovered completely. She was discharged home in a stable condition after decannulation of the tracheostomy tube with advice for regular follow-up and screening of the family in view of possible hereditary etiology.
Parasternal short axis transthoracic echocardiography image demonstrating device is well placed.
Color flow mapping of parasternal short axis transthoracic echocardiography demonstrating no residual flow across the device.
Discussion
Sinus of Valsalva aneurysm (SOVA) is dilatation of the aortic wall located between the aortic valve and the sinotubular junction. Its location is related to one of the coronary arteries designated as the right coronary sinus, left coronary sinus, and noncoronary sinus. As dilatation progresses, it ruptures on to either cardiac chambers or mediastinum. Frequency of rupture of sinus of Valsalva varies according to the location (60% in right sinus, 42% in noncoronary sinus, and 10% in left sinus). Most common site of drainage is RV (70%). It is commonly congenital in origin but can be acquired because of infection, trauma, or degenerative diseases. Reported incidence is 0.09% and higher incidence is reported in Asians (0.46-3.5%). 1 Cardiac failure and sudden auscultation changes suggest possibility of rupture. Typical features are thoracic pain, dyspnea, cough, fatigue, and tachycardia. Severity of symptoms depends on the rapidity, site, and the size of the rupture. Characteristic finding on TOE is windsock deformity. 2 Angiography is considered as gold standard but rarely necessary. 3 RSOVA may lead to diagnostic dilemma. On initial evaluation, it may be misdiagnosed as endocarditis or myocardial infarction (MI).4, 5 Endocarditis could be primary or secondary to congenital SOVA. 4 MI could be due to compression of the coronary arteries from the aneurysm. Our patient was diagnosed with ACS but is unlikely as rupture was at the site of noncoronary sinus. Uncorrected, the rupture almost invariably causes deterioration in heart function and has a rapid downhill course. Treatment of RSOVA is surgical or catheter occlusion. The transcatheter technique for rupture of sinus of Valsalva closure is done with Rashkind umbrella device, Gianturco coils, Amplatzer duct occluders, and Amplatzer septal occluders. Residual shunting and procedure-related AR are the potential complications of transcatheter device closure and these patients need long-term follow-up. Our patient underwent transcatheter device closure and had a successful recovery with no such complications.
Clinical Significance
RSOVA is a relatively uncommon condition and can mimic many other diseases. Our patient was misdiagnosed and treated for ACS and deteriorated further with development of multiorgan failure. Right heart failure evaluation in the setting of appropriate clinical features should prompt consideration of RSOVA as a differential diagnosis. RSOVA if managed appropriately with surgical correction or device closure can lead to complete recovery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.