
Abstract
Background
Low-density lipoprotein cholesterol is one of the prime atherogenic factors, and statins are used to reduce low-density lipoprotein cholesterol. However, concerns about misuse and adverse effects regarding statins have risen lately. This study aims to assess the statin prescription practice and the perceptions about guidelines among doctors in Tamil Nadu.
Methods
A cross-sectional, questionnaire-based survey of physicians practicing in Tamil Nadu was conducted from January 2024 to September 2024. Physicians who have prescribed statins in the past 3 years were included in the study through a voluntary opt-in sampling technique. The estimated sample size was 185. Required permissions and consents were obtained from the ethical committee and individual participants.
Results
The participants had a mean age of 31.5 years, with 62.2% having under 6 years of experience. Although 58.4% were aware of the American College of Cardiology/American Heart Association guidelines, only 5.9% agreed; for the Lipid Association of India, 18.9% were aware, with 2.7% in agreement. Over the past 6 months, 84.8% had modified their statin prescriptions. Atorvastatin was the most commonly prescribed statin. While 85.4% had encountered statin intolerance, only 12.9% were aware of the reporting system, and merely 3.2% had reported such cases, despite frequent observation of side effects, like myopathy (22.2%) and myalgia (8.6%).
Conclusions
The study reveals a gap in physicians’ awareness and application of statin guidelines, with low adherence, inconsistent risk assessment, and dosing practices. It recommends developing ethnicity-specific risk tools and strengthening national guidelines for consistent, evidence-based dyslipidemia management.
Introduction
Elevated low-density lipoprotein cholesterol (LDL-C) is a major modifiable risk factor and one of the most closely linked markers of atherosclerotic cardiovascular disease (ASCVD). In 2021, elevated LDL-C levels were associated with 3.8 million deaths and 1,090 disability-adjusted life years (DALYs) per 100,000 individuals globally. 1 Indians are predisposed to develop ASCVD nearly a decade earlier than people in Western countries, even at lower LDL-C levels. 2
Statins are competitive inhibitors of 3-hydroxy-methylglutaryl coenzyme A (HMG-CoA) reductase, an enzyme involved in the cholesterol synthesis pathway. Thereby, it reduces the hepatic production rate of apoB100-containing lipoproteins, leading to a decrease in both cholesterol and triglyceride concentrations. Statins are effective in lowering LDL-C levels by 20%-50%, lowering triglyceride levels by 10%-20%, and possibly raising serum high-density lipoprotein cholesterol (HDL-C) levels by 5%-10%. 3 Thus, statins are regarded as the cornerstone for primary and secondary prevention of cardiovascular diseases/ASCVD. Statins have been shown to have antiproliferative, anti-inflammatory, antioxidant, and immunomodulatory properties. In addition, statins promote plaque stability and prevent platelet aggregation. The Food and Drug Administration (FDA) and Central Drugs Standard Control Organization (CDSCO) approved statins include atorvastatin, rosuvastatin, simvastatin, pravastatin, fluvastatin, lovastatin, and pitavastatin.4, 5 Newer classes of lipid-lowering therapies, such as ezetimibe and proprotein convertase subtilisin/kexin type 9 (PCSK9) serine protease inhibitors, are typically used as adjuncts to statins.
Statins are still the first line of medical management for those with elevated ASCVD risk, irrespective of their LDL-C values. 6 Recently, concern has been expressed regarding the misuse of statin drugs and the potential for severe adverse effects from statin therapy. 7 The most common side effects of statins are myopathy, hepatotoxicity, and new-onset diabetes mellitus. Major trials and meta-analyses suggest that high-intensity statin therapy is linked to a 9%-12% higher risk of developing type 2 diabetes mellitus, with the JUPITER trial reporting a 26% increase with rosuvastatin.8-10 Rhabdomyolysis is the most serious and rare adverse effect of statin use. 11 There is no specific curative therapy for statin-induced myopathy; however, it is often under-recognized and can be effectively managed if identified early. This raises questions about the potential risk of long-term statin use. The following investigations are suggested before starting statins: alanine aminotransferase (ALT) or aspartate aminotransferase (AST), HDL cholesterol, non-HDL cholesterol, serum creatinine, total cholesterol, triglycerides, and HbA1c.4, 12 Cardiovascular risk assessment scores available include the Pooled Cohort Equations, SCORE, CUORE, and QRISK2, with the most recently updated ones being that by the American Heart Association/American College of Cardiology (AHA/ACC) in 2018 and the European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) in 2019. 13 Most guidelines are based on large European and American studies, with limited validation in South Asians, especially Indians; their applicability remains uncertain. While cardiovascular disease (CVD) risk equations typically include key factors like age, gender, smoking, blood pressure, total cholesterol, and HDL-C, variations in additional risk factors and ethnicity considerations affect their accuracy and applicability across populations. 14
With newer evidence of potential harm from long-term statin use, guideline revisions have taken place globally in a few associations, regulating the dose of statin prescription. 15 Given the lack of implementation of India-specific protocols, statin therapy remains challenging despite a few global guidelines being available. There are no uniform standard guidelines on statin prescription considering risk-benefit analysis for individuals or risk categories of patients (e.g., Asian) based on newer evidence. Hence, the practitioners are at a slight liberty in statin prescription based on their interpretation of the evolving evidence. There is a current need to be updated on the evolving evidence and to comprehend these factors to optimize statin use in India, especially in Tamil Nadu, where the prevalence of CVD is on the rising trend. Therefore, the current study aimed to determine the providers’ statin prescription practice and their perceptions about guidelines among doctors in Tamil Nadu.
Methodology
A cross-sectional study was carried out among registered medical practitioners from January 2024 to September 2024 in Tamil Nadu. The sample size of 185 was calculated using the formula n = 4pq/d2, where prevalence (p) was 88% (practice of prescribing statins based on lipid profile (LP)), 16 absolute error (d) was 5%, and a 10% non-response rate. General practitioners (MBBS), diabetologists (Fellowship/Diploma), general medicine (MD/DNB), and their superspecialties (cardiology, nephrology, endocrinology, neurology, and gastroenterology) were selected through a voluntary opt-in sampling technique. Only those who were practicing in Tamil Nadu after registering with the state medical council were included. Those who did not prescribe any statins for the past 3 years were excluded.
Expert opinion from senior consultants of general medicine and a thorough literature review were the foundations for the questionnaire. The questionnaire for assessing the doctor’s knowledge was developed based on the 2018 American College of Cardiology/American Heart Association (ACC/AHA) Guidelines on the treatment of blood cholesterol. 6 Content validity was assessed using the Item Content Validity Index (I-CVI), calculated as the proportion of experts assigning a relevance rating of 3 or 4 to each item (1 = not relevant to 4 = highly relevant), with values ≥0.78 considered acceptable. The study was started after obtaining clearance from the institutional ethical committee. A self-administered questionnaire, which had an initial eligibility check section and voluntary consent documentation, was circulated as an online Google Forms through various closed social media platforms such as doctors’ WhatsApp groups and emails. Data were cleaned for errors and analyzed using Statistical Package for the Social Sciences (SPSS) version 27. Normality testing was done using the Kolmogorov–Smirnov test and the Shapiro–Wilk test. The descriptive data were expressed as numbers/percentages, mean ± standard deviation, or median interquartile range (IQR). If P < .05, associations were considered significant.
Results
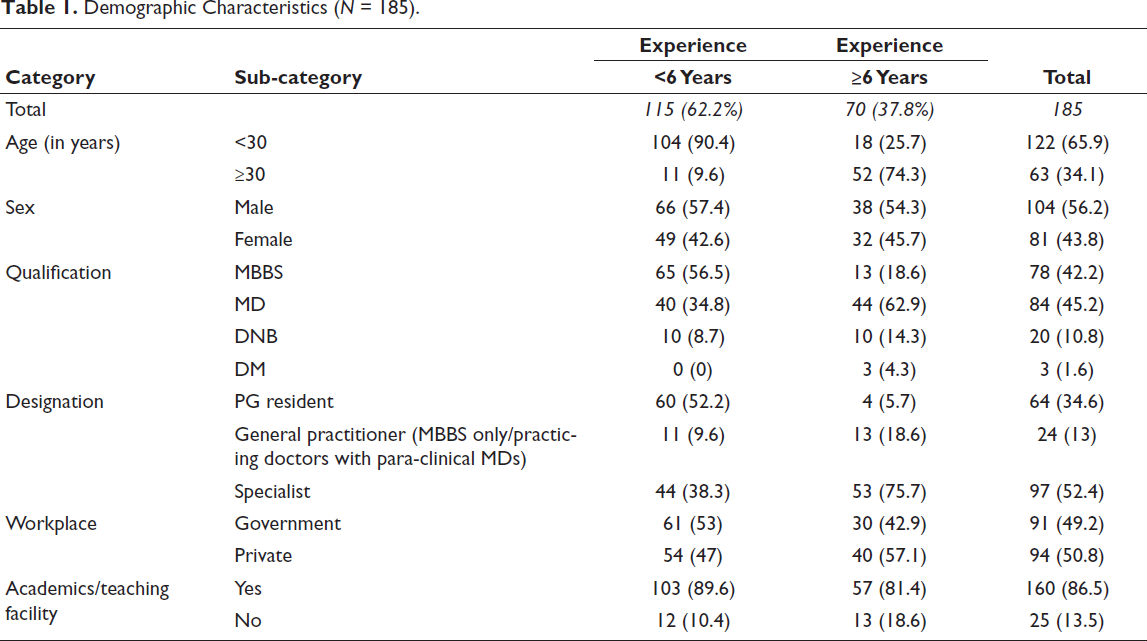
The mean age of the study participants was 31.5 ± 10.5 years, with 122(65.9%) belonging to the age group <30 years. The majority (104, 56.2%) of the participants were males, and 115(62.2%) had less than 6 years of experience. Among the specialists, 80.37% (86 out of 107) were general medicine graduates. Most physicians, 91(49.2%), worked in government hospitals, and 160(86.5%) were in academic settings (Table 1).
Demographic Characteristics (N = 185).
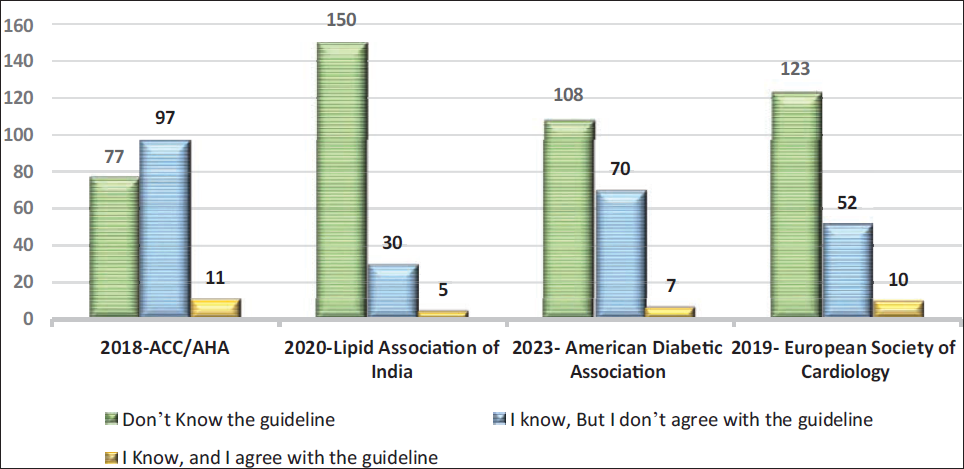
Notably, 108(58.4%) of practitioners were aware of the ACC/AHA guidelines, but only 11(5.94%) of the total agreed with these guidelines. The majority, 150(81.1%), did not know about the Lipid Association of India (LAI), and even among those who were aware, only 14% (5/35) agreed with the guideline (Figure 1).
Knowledge and Attitude of Physicians on Various Statin Guidelines (N = 185).
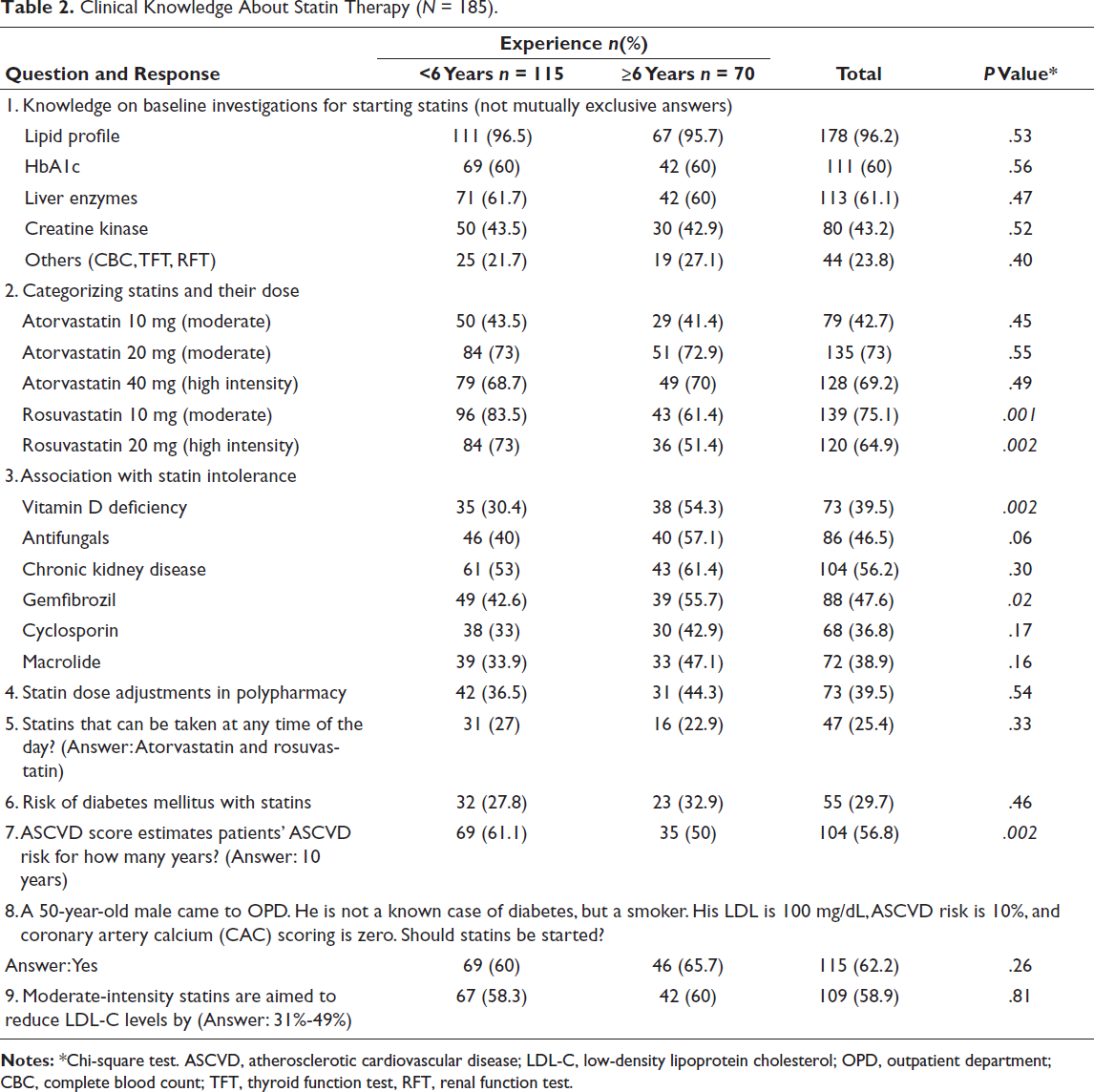
Knowledge About Statin Therapy
Most physicians, 178 (96.2%), knew that an LP test before prescribing statins is recommended, and there was no significant difference in this with years of experience (Table 2). The mean knowledge score on categorizing the dose of statins was 0.65 ± 0.23 (on a scale of 0-1), and less experienced practitioners significantly outperformed in recognizing rosuvastatin doses. One-fifth (39, 21.1%) categorized all doses of atorvastatin correctly, 93(50.3%) categorized all doses of rosuvastatin correctly, and 25(13.5%) categorized all the statin doses correctly. The knowledge on side effects of statin therapy included myopathy (95%), myalgia (89%), hepatitis (54%), rhabdomyolysis (25.9%), gastrointestinal discomfort (19.5%), transaminitis (3.2%), and renal failure (2.2%). Risk of diabetes mellitus with statins was known to 55(29.7%), and experienced practitioners knew that vitamin D deficiency (54.3%) and gemfibrozil (55.7%) were associated with statin intolerance. Overall, only 39.5% knew that statin dose adjustments are required in polypharmacy (Table 2).
Clinical Knowledge About Statin Therapy (N = 185).
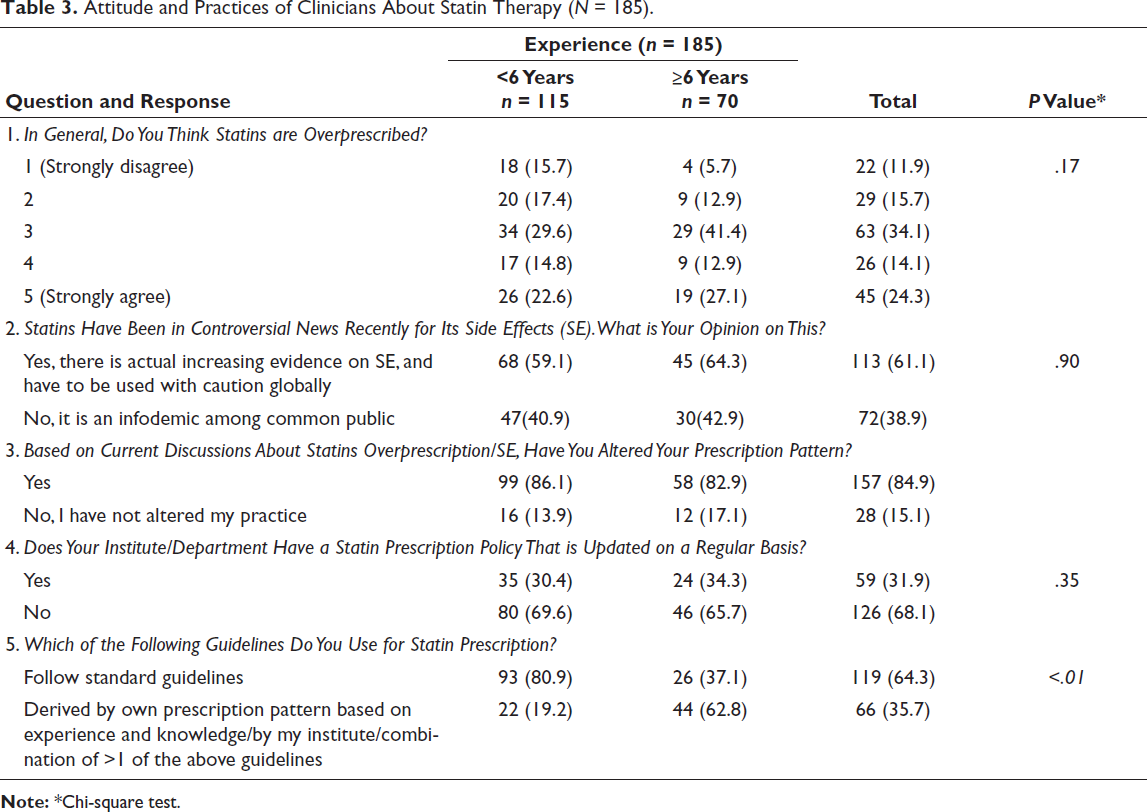
Attitude Toward Statin Prescription
Around 38% of practitioners agreed that statins are overprescribed. There is recent evidence that increasing side effects due to statins were reported by 113(61.1%), and 72(38.9%) felt that it is only an infodemic (Table 3). A majority, 126(68.1%), report a lack of updated institutional policies for statin prescriptions. Only 95(51.4%) said it is always necessary to calculate the ASCVD score before prescribing statins, and 2(1.1%) and 23(12.4%) considered it not needed or needed only for research purposes, respectively (Table 3).
Attitude and Practices of Clinicians About Statin Therapy (N = 185).
Practice of Statin Prescription
In the past 6 months, the median number of patients to whom respondents prescribed statin therapy was 40 (IQR 20-100). Among the 157(84.8%) who had altered the prescription, 58(31.4%) reduced the dose of the prescription, 77(41.6%) reduced the number of prophylactic doses, and 48(25.9%) started following the ASCVD score. Currently, 103(55.7%) follow AHA/ACC guidelines for statin prescription, five (2.7%) follow LAI guidelines, four (2.2%) follow American Diabetes Association (ADA) guidelines, and seven (3.8%) follow Employees’ State Insurance (ESI) guidelines. And 66(35.7%) have their own prescription pattern based on their experience, or combining more than one guideline or an institutional policy that does not directly adopt any of the above guidelines. The most common reasons for choosing a guideline again were institutional policies, senior consultant suggestions, being globally accepted, easy to follow, and evidence-based. About 70(37.8%) always calculated ASCVD before prescribing statins (Table 3).
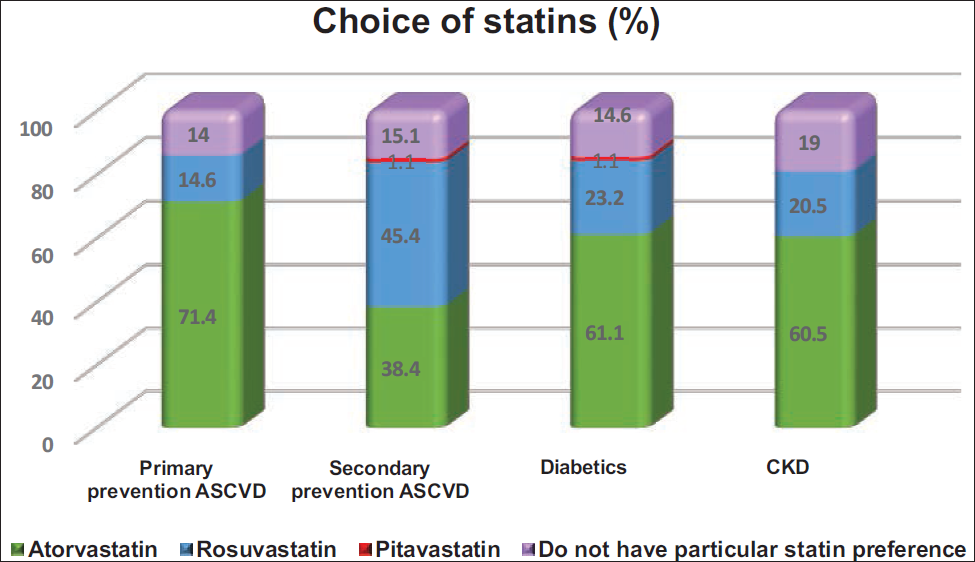
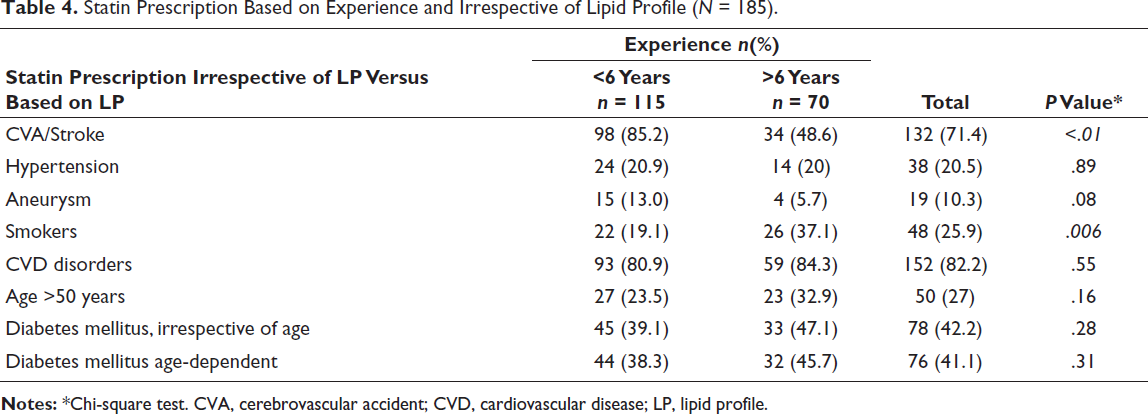
Atorvastatin was chosen over other statins for primary prevention of ASCVD by 132(71.4%), for those with diabetes mellitus (113, 61.1%), and with chronic kidney disease (112, 60.5%) (Figure 2). The majority (79, 42.7%) prescribed LP testing once every 3-6 months for those on statins, and the correctness of monitoring did not differ by experience. The LDL-C target was set at less than 100 mg/dL by the majority of participants (122, 65.9%), with a higher proportion of those with lesser experience having this target (P = .03) (Table 3). As per the physician, the time taken by their patients to achieve the target LP following statin therapy was 6 (IQR 4-12) months. Irrespective of the LP, statins were prescribed by 152(82.2%) for those with CVD disorders, and by 132(71.4%) for cerebrovascular accident (CVA)/stroke. However, statin prescription irrespective of LP did not differ with experience, except for smokers and those with CVA (Table 4).
Preferred Statin Choice Among Doctors in Hyperlipidemic Patients.
Statin Prescription Based on Experience and Irrespective of Lipid Profile (N = 185).
Nearly 158(85.4%) practitioners have encountered some form of statin intolerance among their patients. In case of encountering a statin intolerance, 73 clinicians (39.5%) continued treatment by reducing the statin dose, 57 clinicians (30.8%) discontinued therapy until symptoms resolved and then restarted a lower dose, whereas 38 clinicians (20.5%) opted for a switch to an alternative statin. About 9.7% opted to stop statins until being investigated thoroughly and used non-statin drugs in the meantime. Only 24(12.9%) of respondents were aware of the statin intolerance reporting system, and six (3.2%) had also reported it. Among those who did not know where to report, 22(11.9%) had encountered statin intolerance. Six (3.2%) said that statins do not have any major side effects that need to be reported. About 75(40.5%) either strongly agreed/agreed that there is a need for uniform and evidence-based guidelines for statin prescription.
Discussion
The prescription of statins has been widely adopted for prophylactic purposes since their early trials in the late 20th century. 17 Despite their widespread use, controversy remains regarding the long-term safety of statins, as early trials provided limited and inconclusive data on adverse effects and comprehensive risk-benefit analysis. A meta-analysis had reported a neutral effect of statins on cancer. 18 Recent European guidelines on statin prescription demonstrated a significantly lower eligibility rate (4%) compared to 20%-34% under other international guidelines, despite maintaining a high sensitivity and only minimal losses in specificity. 15 In light of emerging evidence on adverse effects and the potential for lower doses to offer similar benefits with fewer risks, the importance of optimizing prophylactic dosing has gained attention.19, 20 In India, where the burden of ASCVD is substantial, the absence of population-specific national guidelines has contributed to uncertainty among practitioners in assessing the risk-benefit profile and making informed treatment decisions. Therefore, the current study aims to assess the existing knowledge, preferred guidelines, and statin prescribing practices among doctors.
Most of the physicians (58.3%) were aware of the ACC/AHA guidelines, but only 5.94% of the total agreed with this guideline. Regarding the 2013 AHA guidelines, a previous study 21 in Singapore showed that only 35% were aware. In another study, though the majority 96% were aware, 47% disagreed with the guidelines, followed by the majority saying they were not fully educated about the same to implement them. 8 Current risk prediction tools, like the ASCVD risk calculator, based on the Framingham Heart Study, may misestimate CVD risk in ethnic groups such as Indians, as they primarily include White and African American populations. The majority (81.1%) did not know about LAI, and even among those who were aware, only 14% agreed with the guideline, and of the total, only 2.2% followed LAI. The series of LAI consensus statements I-IV state that the earlier and aggressive ASCVD among Indians needs both intense management and lifetime ASCVD risk, instead of the usual 10-year risk. The wide availability and low cost of statins in India enable the implementation of effective LDL-C-lowering therapy in individuals at high risk of ASCVD.22-24 Notably, the comprehensive recommendation of LAI was not made exclusively from Indian data due to insufficient data availability. 22 The 10-year CVD risk threshold for starting statins differs by country: 20% in India, 10% in the UK, and 5%-7.5% in the USA. 25 Notably, literature from the Western population also shows that reducing statin treatment to a 10-year ASCVD risk of 3% will still outweigh the risk-benefit ratio and be cost-effective. Statins have been proven to be very effective in reducing ASCVD risk, with no apparent threshold at which LDL-C lowering is not associated with reduced risk. Yet, a significant on-treatment residual risk of major cardiovascular (CV) events still exists according to meta-analyses of statin trials. Findings like this point to the unmet needs of the patients on statin treatment. About one-fifth correctly classified all doses of atorvastatin. While many were unable to identify the intensity of rosuvastatin based on dose, experienced clinicians performed better than their counterparts. But in the reports of Zaitoun et al., 26 a higher proportion (40.6%) of physicians correctly identified the various statin intensities. Doctors disagree with the 2013 ACC/AHA guidelines on the definitions of high-, moderate-, and low-intensity statins and their use in high-risk individuals, according to a study by Setia et al. 21 This disagreement may be related to safety concerns with Asian patients. Only a quarter (25.4%) correctly identified statins that can be taken at any time. However, in studies by Al-Ashwal et al. 27 and Elnaem et al., 28 only 21.9% and 52.3%, respectively, did so. The revised guidelines prioritize risk stratification over lipid targets in cholesterol management and lower the thresholds for initiating drug therapy for primary prevention. 15 This shift has sparked debate concerning the risk calculator’s accuracy, the absence of lipid targets, and broader statin use. In response, follow-up studies affirmed the calculator’s reliability and underscored shared decision-making and treatment efficacy. Both the AHA and the ESC guidelines state that applying their recommendations for Asians needs special considerations, like not completely relying on the ASCVD risk estimator, but rather to have shared clinical decision-making, or multiplying the risk by 1.3, respectively. 26
In accordance with high awareness of myopathy, myalgia, and rhabdomyolysis as statin-related adverse effects, Clough et al. 29 also found that 97.2% of physicians recognized myopathy, and 83.3% recognized rhabdomyolysis. Among the observed adverse events (AEs), muscle AEs (myopathy and myalgia) were the commonest, as in the reports of Golomb et al. 30 and a systematic review (1%-10%) until 2016. 8 This muscle AEs were found in relation to elevated creatine kinase (CK). 11 Literature indicates that Asian ethnicity predisposes individuals to statin-induced myalgia. 31 Most of them (29.7%) knew that statins had the risk of diabetes mellitus, and this was consistent with previous reports that stated that the risk was high with prophylactic statins of high intensity and longer duration.31-34 In accordance, Clough et al. 29 also showed that 27.8% of the physicians believed that statins had a risk of diabetes mellitus. As AEs of statins, 54% of physicians knew about hepatitis, and 3.2% knew about transaminitis. Clough et al. 29 also reported that 66.7% of doctors knew that liver injury was related to statins. Muldoon et al. 32 and Clough et al. 29 showed evidence of cognitive disturbances with statins. However, none in the current report mentioned that. Compared to the prevalence of AEs, a good proportion of doctors knew about the side effects of statins. The adverse effects of statins are dose-dependent and are high when statin potency is increased by another drug or other pathologies. The mechanism is explained by the inhibition of the cytochrome P450 3A4 system. 33
Most physicians, 96.2%, knew that LP testing is recommended before prescribing statins. Wander et al. 16 found that 88% of doctors ordered an LP before statin prescription. Monitoring lipids after initiating statin therapy was done by 42.7% of practitioners every three to 6 months. Al-Ashwal et al. 27 reported that 57.4% felt that monitoring the LP after 3 months of statins was correct. In accordance, Bucheit et al. 34 also showed that 41% of the physicians monitored LPs after initiating a statin. But in the reports of Wander et al., 16 the percentage was higher (80%). About 60% ordered HbA1c, 61.7% liver enzymes, 43.5% CK, and 21.7% other (CBC, TFT, RFT) investigations before starting statins. In the study by Al-Ashwal et al., 27 42.1% ordered HbA1c, 77.3% liver enzymes, and 20.4% CK before starting statins. These considerations of baseline investigations indirectly reflect the knowledge on AE of statins or the cautious risk-benefit analysis of prescriptions.
Atorvastatin and rosuvastatin were the most preferred choices for primary prevention (71.4%) and secondary prevention (45.4%) of ASCVD, respectively. Although Wander et al. 16 also reported atorvastatin as the preferred choice for primary prevention (72.9%), their study showed that physicians opted for the same for secondary prevention (54.6%). Though in accordance with Wander et al., it also showed that atorvastatin was the preferred choice in primary prevention (72.9%), and physicians opted for the same for secondary prevention (54.6%). But a similar proportion of physicians preferred rosuvastatin for secondary prevention (46.7%) in a study by Wander et al. 16 In the reports of Narasingan et al., 35 rosuvastatin was preferred for both primary (50.6%) and secondary prevention (49.4%), and only 38.5% preferred atorvastatin for primary prevention. For those diagnosed with CVD, the majority (82%) were prescribed statins irrespective of LP. According to Clough et al., 29 most of the physicians (59.8%) stated that cardiac risk factors affect the prescription of statins very often/often. In the current study, clinicians preferred atorvastatin (61.1%) and rosuvastatin (23.2%) for people with diabetes (PWD). The choice of atorvastatin over rosuvastatin for PWD was also previously reported. 16 But Narasingan et al. 35 and Setia et al. 21 showed that rosuvastatin (27.5%) was the most preferred statin. For PWD, 42.2% gave statin prophylaxis irrespective of LP and age. Wander et al. 16 found that most of the respondents (49.6%) opted not to prescribe statins to PWD, regardless of their LDL-C levels. Atorvastatin was highly preferred for CKD (60.5%), and in accordance with a study in Qatar, it has been shown that atorvastatin is the safest statin in CKD patients. 36 Narasingan et al. 36 also reported that atorvastatin was highly preferred, but by a lesser proportion (44.4%). In contrast, Setia et al. 21 showed that rosuvastatin was the most preferred for CKD. Irrespective of the LP, statins were prescribed by 71.4% of CVA/stroke patients to prevent further episodes of cardio/cerebrovascular events. Long-term statin use for more than 5 years has been associated with a slight increase in the annual risk of hemorrhagic stroke, but this increase is observed only in individuals with a prior history of stroke. Nevertheless, the overall benefits of preventing ischemic stroke outweigh this risk. 37 Setia et al. 21 reported that rosuvastatin was preferred over atorvastatin for those with a history of stroke. The majority (65.9%) of physicians reported that the treatment target for LDL-C with statins is less than 100 mg/dL.
The LAI and the European guidelines recommended a more stringent target of <70 to <50 mg/dL and <55 to <40 mg/dL, respectively, based on ASCVD risk being in the very high category.23, 38 The large global INTERHEART trial highlighted that Indians are prone to myocardial infarctions even at a lower LDL-C level, and the study also focuses on small, dense, and atherogenic LDL particles (LDL-Ps), which are higher in Indians. 39 The majority (51.4%) said that it is always necessary to calculate the ASCVD score before prescribing statins, but in actual practice, 37.8% followed it. Although a higher proportion of physicians reported always or very often calculating the 10-year ASCVD risk score, 51.5% of primary care providers believed that it was based on other clinical factors. 29
About 85.4% of physicians reported encountering statin intolerance in their practice, which is consistent with the findings of Wander et al., 16 who reported a 92% incidence. During an intolerance, 39.5% opted to lower the statin dose directly, and 30.8% opted to stop and restart at a lower dose. In accordance with Wander et al., 16 it was also reported that the most preferred option for management of statin intolerance was reducing the statin dose (39%), closely followed by stopping and restarting the statin at a lower dose (34.5%). In general, owing to the current knowledge on statins, 84.8% had altered their statin prescription patterns. This is expected in the evidence-based era, as the literature has documented the non-inferiority of moderate-intensity statins compared to higher-intensity statins. 19 The preference for non-statin drugs in case of intolerance was opted for only by a few (9.7%). A similar finding (10.9%) was reported by Wander et al. 16 Ezetimibe and Bempedoic Acid have been shown to complement statins in lowering LDL through a different pathway and may prove beneficial in those with statin intolerance in the future.40, 41 As the study population predominantly comprised younger physicians, the findings may not be generalizable to senior physicians. Additionally, voluntary opt-in sampling through social media platforms introduces selection bias, favoring younger, academically inclined physicians.
Conclusion
This study highlights a significant gap between physicians’ awareness and the practical application of evidence-based statin prescribing guidelines. While general awareness of the ACC/AHA recommendations exists, adherence remains low, and familiarity with local guidelines is limited. The findings reveal deficiencies in knowledge related to appropriate statin dosing, risk assessment, and adverse effect management, particularly among early-career physicians, mostly due to the varied updated international guidelines. Despite recognizing the importance of lipid profiling and ASCVD risk scoring, these are not consistently practiced. The prevalence of misconceptions, variability in prescribing patterns, and underreporting of statin intolerance underscores the urgent need for targeted, stronger implementation of national guidelines and standardized institutional protocols to enhance the quality and consistency of dyslipidemia management.
Recommendation
Since the risk of ASCVD is known to vary based on ethnicity, the study recommends, the development of ethnicity-specific risk prediction tools and treatment guidelines, with the core principle being maintained. Also, the current LAI may be strengthened both in its evolving evidence-based recommendations and in its implementation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The study was started after obtaining clearance from the institutional ethical committee. A self-administered questionnaire, which had an initial eligibility check section and voluntary consent documentation, was circulated as online Google forms through various closed social media platforms such as doctor’s WhatsApp groups and emails.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.