
Abstract
Objective:
Atherosclerosis is a chronic inflammatory disease that can be undetected in middle-aged patients. Abdominal aortic calcifications (AACs) are one form of cardiovascular disease (CVD), and these can go undetected during a routine physician visit. Sonography has the potential to assess CVD progression, quantify plaque in the aorta, and help to quantify risk in asymptomatic patients.
Methodology:
This pilot study modified a current AAC grading system to create a scoring method for sonographic images among a small cohort of asymptomatic participants. A traditional portable ultrasound unit was used to image participants, and a subset underwent the same imaging with a handheld transducer and tablet.
Results:
In this cohort, six males and five females, it was possible to adequately visualize and assess plaque, utilizing both types of ultrasound equipment. The abdominal aorta was divided into segments on the sonogram for quality of grading. Ten participants were categorized with a grade II and one participant was given a grade IIIA.
Conclusion:
Replication of this modified grading system is needed to better understand the clinical utilization of sonography as a risk assessment tool. The risk assessment scoring was not dependent on the type of device used.
Atherosclerosis is a chronic inflammatory disease that develops from the formation and growth of plaque, within the arterial lumen, and concurrent loss of elasticity, within the arterial wall.1,2 This plaque is made up of fatty substances, cholesterol, cellular waste products, calcium, and fibrin. 3 When calcium is part of the composition of a plaque, it may be referred to as calcification. As this plaque continues to build up, this can affect the blood flow and the elasticity of the vessel. The progression of the disease begins early in life and is often asymptomatic. It can evolve rapidly in individuals as early as 30 years old, while in others, atherosclerosis may not progress until later in life.1,3 Unfortunately, atherosclerosis can arise in a variety of ways and affect multiple different arteries. The accumulation of plaque within these areas can contribute to cardiovascular disease (CVD) and also result in stroke, heart attack, and peripheral arterial disease. 2 The accumulation of plaque and calcifications, within the aorta, can be noted in older adults. Abdominal aortic calcifications (AACs) can contribute to cardiovascular events and impact medical and surgical treatment. 4 In a previous study of 617 participants, AAC was present in both men and women and affected multiple areas within the aorta from the L1 to L4 lumbar region. The highest prevalence of calcification was shown at the L3 and L4 levels. 5 In a multiyear, longitudinal study of patients, O’Connor et al, found a statistically significant advantage to imaging the abdominal aorta with a nonenhanced computed tomography (CT) compared with screening with a Framingham risk score. 6 The abdominal aortic CT was shown to be a better predictor of future CVD events than the Framingham risk score. 6 Additional literature has shown similar risk factors between aortic and coronary artery calcifications. In these studies, it was noted that AAC measured by CT was an independent and effective predictor of future adverse CVD events.7-9 These previously listed studies advocate for the use of CT to better quantify aortic plaque. Dual-energy x-ray absorptiometry (DXA) and quantitative computed tomography (QCT) have proven to be additional diagnostic methods for measuring AACs. DXA has been demonstrated to have high reproducibility among users and has shown to yield similar results to radiography. 10 The QCT approach was compared with DXA and radiography, and was found to be highly comparable in providing an AAC score. 11 The current standard for grading AACs, when utilizing a lateral radiograph of the aorta, is the AAC-8 system. This method uses the length of vertebral segments comparatively with the length of the AAC. Grades range from one to eight, increasing with severity. This scale requires that the image of the aorta also has corresponding visualization of vertebral bodies. 12
Given that screening of potentially healthy individuals may be necessary, nonionizing imaging techniques may provide similar data without the risk of ionizing radiation. Current radiographic measurement methods have several drawbacks among them, including exposing patients to radiation and being costly to perform. Due to these concerns, widespread utilization of these imaging techniques may be prohibitive for a CVD risk assessment program in a primary care setting. Jayalath et al identified that imaging modalities that can quantify abdominal aortic plaque may be a useful tool in understanding and assessing risk in patients. 4 The current measurement methods being used with radiographs and DXA could be adapted to sonographic imaging, as a nonionizing evaluation methodology.
Currently, sonography is used to assess the abdominal aorta for the presence of vessel pathology such as plaque, aneurysm, endoleak, and dissection. 13 Limited research has been done on quantifying AACs, with the use of sonography. However, in a previous study of 1667 participants, consecutive sonograms of the abdominal aorta were completed with measures of AACs, as well as coronary angiography. AAC, demonstrated on sonography, was an independent factor associated with the presence and severity of coronary artery disease shown on coronary angiography. 14
Given the silent progression of atherosclerosis, reliable methods to assess patient risk for CVD and events are paramount. 15 Noninvasive imaging techniques could assess disease progression and help to quantify risk in asymptomatic patients. The purpose of this pilot study was twofold. First, a current AAC grading system was modified to create a scoring method utilizing sonograms. Second, a traditional portable ultrasound unit was used to image participants, who might be at risk for AACs. Some participants were also selected to undergo additional imaging with a handheld transducer and tablet. This subset of participants was imaged again, with the handheld transducer and tablet, to check the image quality and consistency of AAC scoring.
Methods and Materials
A preexperimental design was used for imaging and demographic data collection based on a convenience sample of 11 participants. This cohort consisted of six asymptomatic males and five asymptomatic females, between the ages of 40 and 56 years. The study was institutional review board approved, and all participants were consented prior to performing any imaging or data collection. Any participants between the ages of 40 and 60 years were invited to the study as well as not having met the exclusion criteria before enrollment. Exclusion criteria for this study consisted of any history of symptomatic cardiovascular events such as myocardial infarction or stroke. After the consent was obtained, images of the abdominal aorta from iliac bifurcation to renal arteries were acquired. The participants’ medical records were also reviewed for additional pertinent data related to demographics and body mass index (BMI) calculation.
Equipment
All ultrasound equipment and transducers are regularly validated for quality control (QC) and assurance. Transducers are checked monthly to ensure accurate caliper placement and measurements, by the use of a QC phantom. All measures were recorded and evaluated to ensure there are minimal to no changes in equipment quality.
A GE Logiq I (Waukesha, WI, USA) portable ultrasound laptop unit with a 2- to 5-MHz curvilinear transducer was used to collect images on all participants. The abdominal imaging preset was used on the Logiq, but the frequency was downshifted to 2.0 MHz, overall gain adjusted to 69, and the output power was increased to 100%. Time gain compensation and overall gain were the only adjustments made in the sonographic imaging technique. As mentioned, the focal zone was adjusted to a far field depth that included the aorta and vertebral body interface. Only three participants agreed to a repeated imaging examination with a novel handheld Philips Lumify Ultrasound (Bothell, WA, USA) transducer and Android Surface Pro tablet. The Lumify 2- to 5-MHz curvilinear transducer was used for the added sonographic imaging, and limited presets were available. This transducer can be connected to any device that has the Lumify ultrasound application for image acquisition. For the purposes of this study and to match the imaging of the Logiq I transducer as closely as possible, an Android tablet was used for easier viewing.
The added sonographic examination with this novel handheld ultrasound system was done to gauge the usability, utility, and desirability (UUD) of this equipment in providing this type of risk assessment, in nearly any imaginable setting.
Sonographic Examination
For all the sonographic examinations, the participants were asked to lie in the supine position. The participant’s abdominal aorta was imaged from the ventral position, starting at the aortic bifurcation and continuing to the proximal abdominal aorta. These images were acquired in the sagittal, transverse, as well as oblique planes for postprocedure evaluation and assessment. From the sonographic images obtained, each region was examined for calcifications and the aortic intima-media thickness (a-IMT). This was acquired by imaging a section of the aorta and then using the equipment calipers to measure the thickness down to one tenth of a millimeter. See Figure 1 for a-IMT measurement example.
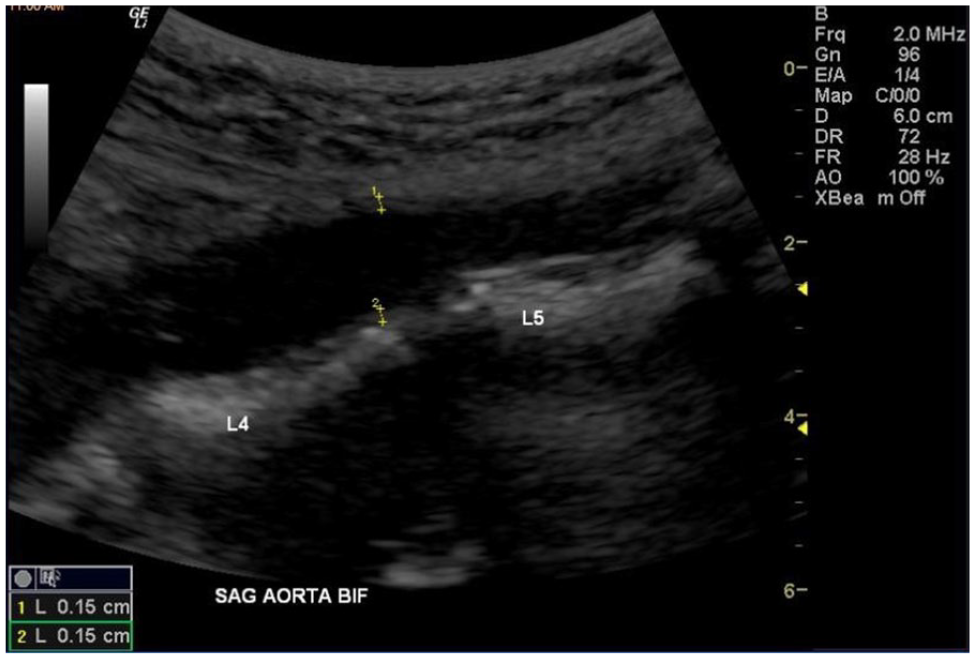
Measurement of aortic intima-media thickness between the L4 and L5 vertebrae.
Image Analysis
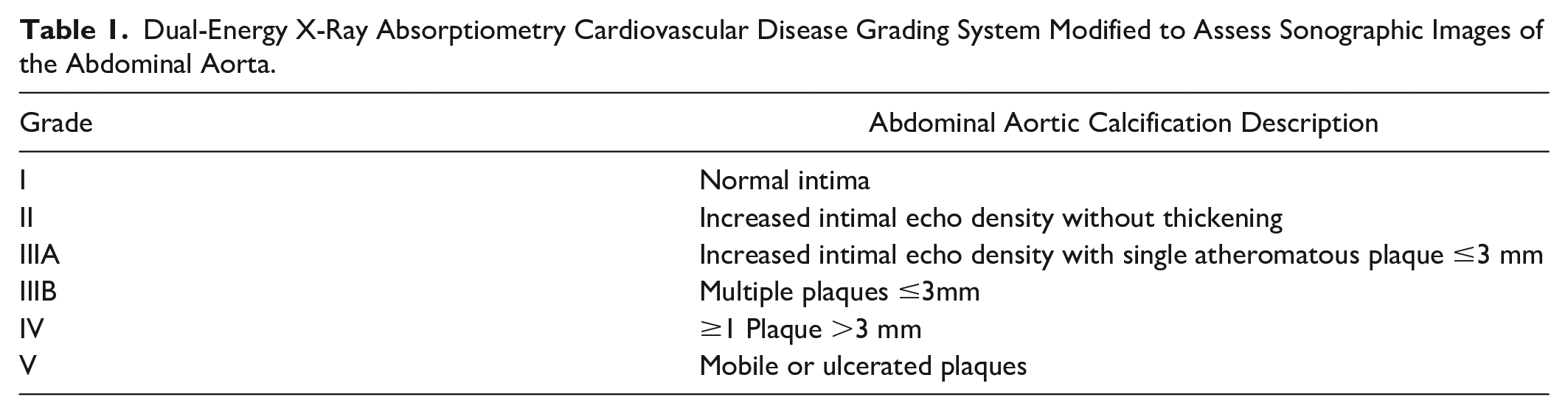
Multiple images were saved to the hard drive of both the laptop and the novel handheld ultrasound systems. All the images were reviewed postexamination for analysis, measurement, and scoring. The aortic calcifications, noted sonographically, were evaluated with the DXA grading system, with slight modifications. The DXA-based grading system involved reviewing the abdominal aorta image and counting the calcific plaques, as well as measuring their size (see Figure 2). The DXA-based grading system ranks the level of CVD risk, based on the thickness of the calcification. This evaluative system assigns a grade from I to V, for CVD risk 16 (see Table 1)
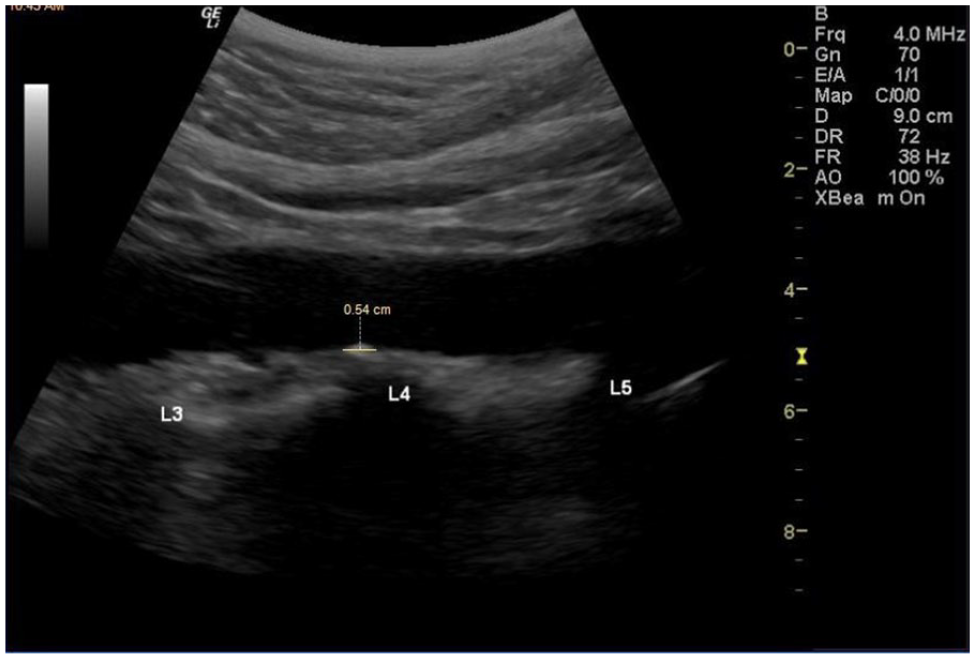
Calcified plaque measured within region 1 (R1).
Dual-Energy X-Ray Absorptiometry Cardiovascular Disease Grading System Modified to Assess Sonographic Images of the Abdominal Aorta.
The slight modifications to the scoring system required terminology adjustments, allowing for it to be translated to sonography. Another adjustment, unlike DXA or radiography, sonographic images of the aorta cannot routinely capture the entire length of the vessel in one image. For this reason, an additional modification was needed so that the grading system could be broken up into three regions. These regions were defined by using the vertebrae and aortic bifurcation as landmarks (see Figure 3).
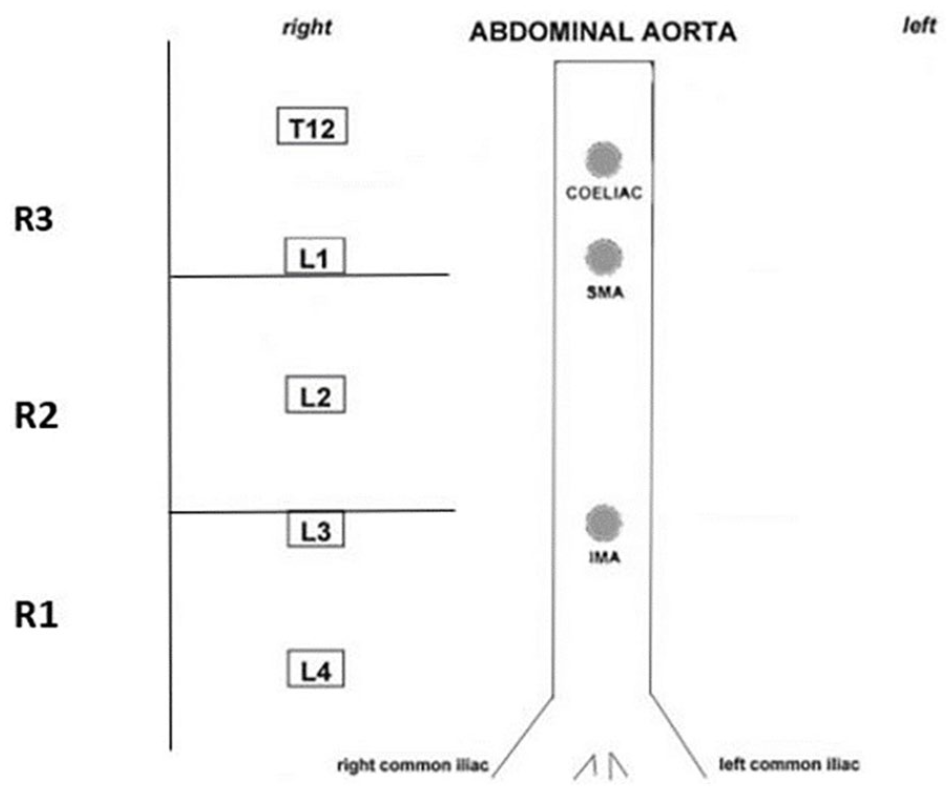
Adjusted abdominal aortic calcification scoring segregated into aortic regions and a graphic means of recording plaque locations.
A grade was assigned based on the above scoring system. After all regions were reviewed and scored, a total AAC grade was assigned. A grading sheet was used to record the data, and each image was evaluated by two researchers (KDE and IWB) for QC. If any discrepancies arose, an additional researcher (ANB) would make the final determination.
The a-IMT manual measurements were made multiple times to obtain the mean measure of the thickness of the aortic wall. Anterior and posterior measurements were attempted in each of the three segments of the aorta. The posterior wall of the aorta was the most consistently measured thickness across all patients, especially in regions 1 and 2. This method of recording a posterior a-IMT was most recently reported, and these analytics were replicated. 17 The posterior a-IMT measure was obtained in the following manner. Each region was evaluated and that portion of the abdominal aorta was measured in the center of the image, perpendicular to the incident beam. Although calcific, dense vessel walls were included in these measures, large deposits of plaque or an atheroma was never part of any measures.
Given the small size of this cohort, anticipated statistics were limited to frequency, means, and limited comparisons. The a priori P level for any inferential comparisons was set at an alpha level of .05.
Results
Descriptive Statistics
The participants consisted of six males (55%) and five females (45%). The age of participants in this study ranged from 40 to 56 years old, with a median of 46 years old. Forty-five percent of the participants were in the age range of 40–45 years old. In this cohort, there was one Asian male and one male who identified as being of Hispanic ethnicity. Based on the weight and height data collected from the participants, a BMI was calculated. According to the BMI interpretation standards listed by the Centers for Disease Control and Prevention, 18 among the 11 participants, 45% had a healthy weight, 18% were overweight, and 36% were obese (see Table 2).
Descriptive Statistics for the Gender, Age, and BMI Distribution of the Cohort.
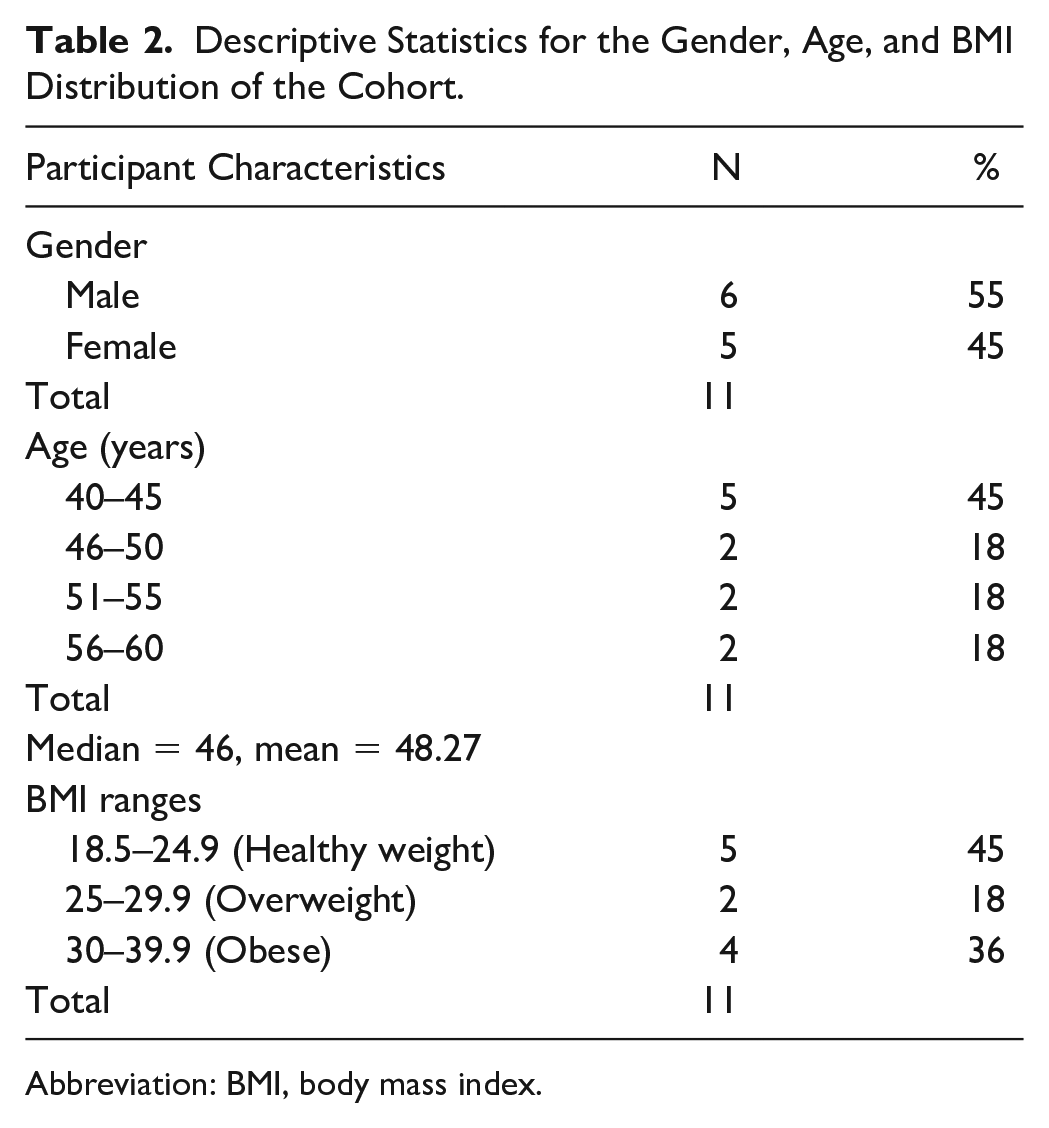
Abbreviation: BMI, body mass index.
All the patients had their blood pressure (BP) taken as part of the overall research procedure, and the systolic and diastolic measures were taken within 15 minutes of the sonographic assessment of each patient. The mean systolic BP was 128 mmHg, and the mean diastolic BP was 74 mmHg. Table 3 provides the BP measurements for all the participants in the study (N = 11). Three participants (27%) did report being on antihypertensive medication at the time of data collection. In addition, none of the participants self-reported a diagnosis of diabetes mellitus.
Systolic and Diastolic Endpoints for BP Recorded for Participants in This Cohort.
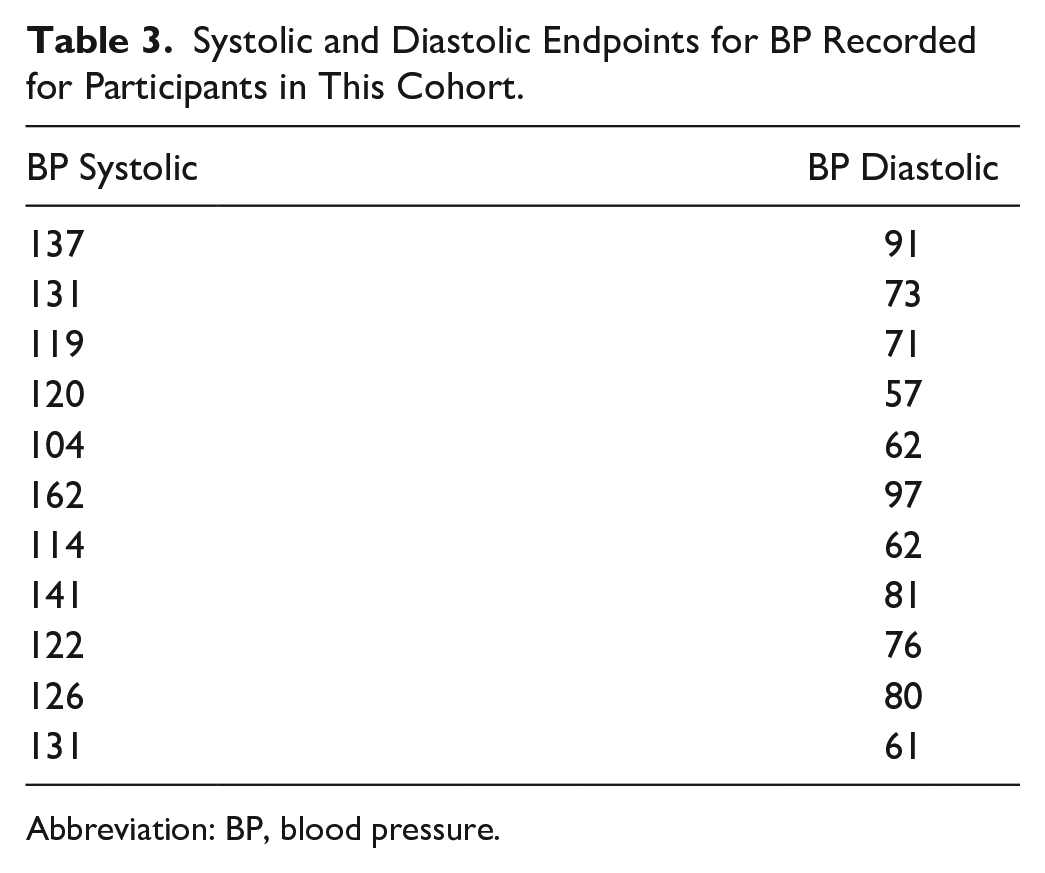
Abbreviation: BP, blood pressure.
The overall AAC grade was determined by the subscores that were assigned to abdominal aortic regions 1–3. The overall AAC grade was determined by the highest grade awarded to a region and largely determined by abdominal aortic regions 2–3. Ten participants (91%) were categorized with a summative grade II (increased intimal echo density without thickening), and 1 (9%) participant was given an overall grade IIIA (increased intimal echo density with single atheromatous plaque ≤3 mm; see Table 4). As indicated, although the aorta was divided into three regions, region 1 was consistently imaged but not enough to definitively measure or grade. This lack of ability to image, the suprarenal portion of the aorta, may have been due to the propensity for this region to be obscured by intestinal gas.
Summative AAC Grading for the Aorta Segments Evaluated in This Cohort.
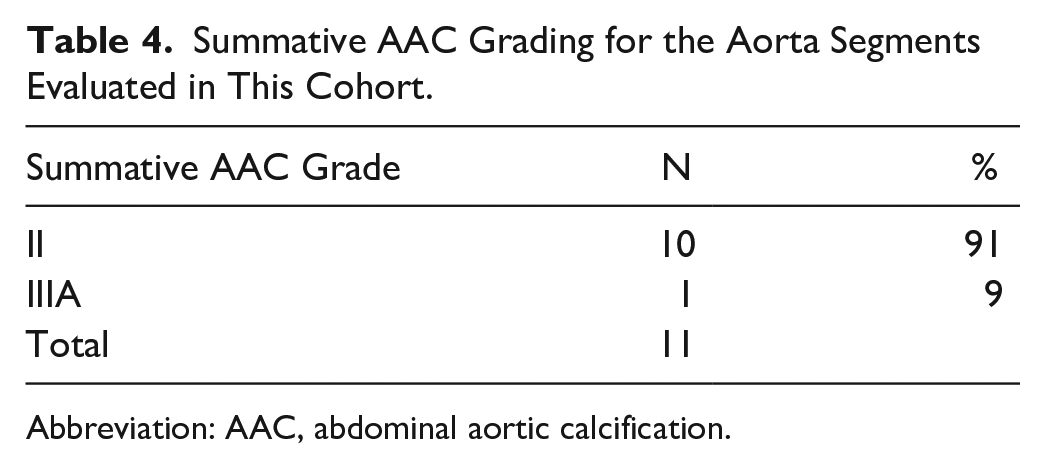
Abbreviation: AAC, abdominal aortic calcification.
As mentioned in the previous sections, a posterior a-IMT measurement was taken in regions 2 and 3. Region 1 was not consistently visualized with enough spatial resolution to consistently obtain a posterior a-IMT measurement. For the cohort, the mean posterior a-IMT for region 1 was 0.30 cm and the mean posterior a-IMT for region 2 was 0.31 cm. See Table 5 for individual a-IMT measures. Two participants had the greatest a-IMT measures (0.45 cm), and these were both located in region 1. These two participants were over the mean age and BMI.
Posterior a-IMT Measured Manually for Those Segments Visualized, in This Cohort.
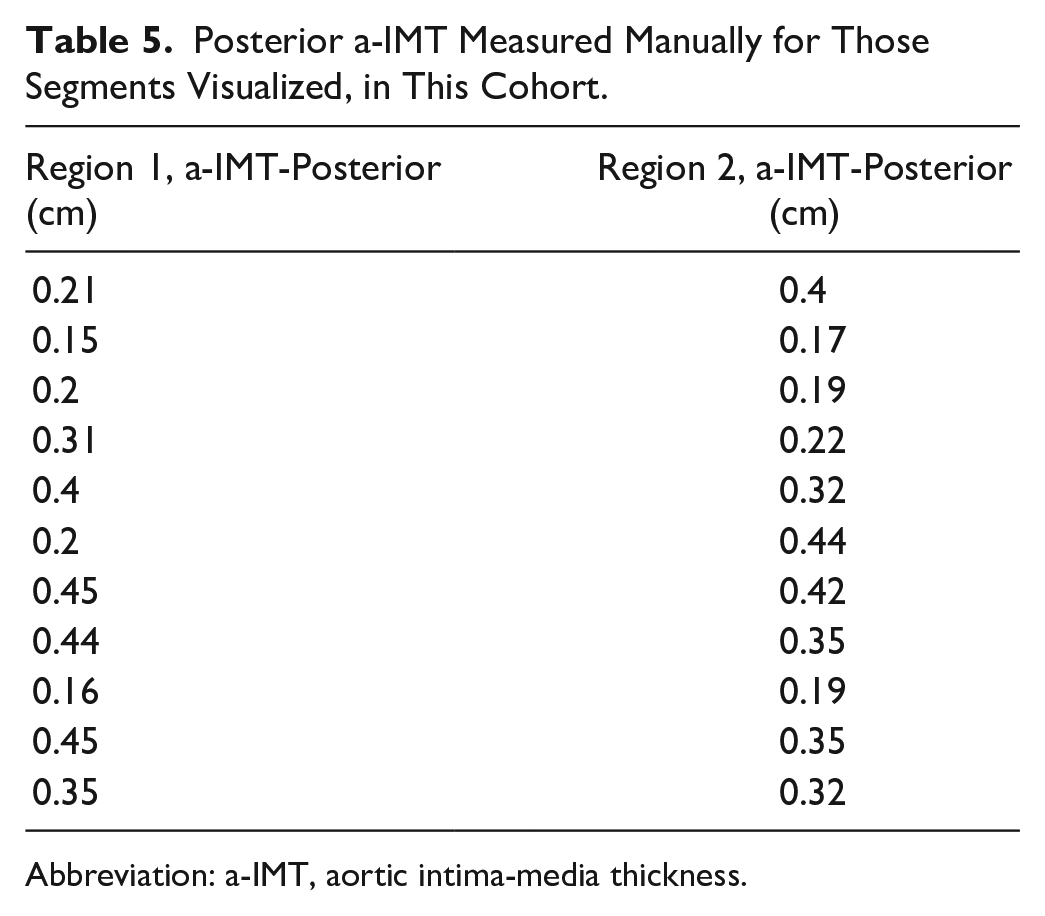
Abbreviation: a-IMT, aortic intima-media thickness.
UUD With the Novel Handheld Ultrasound System
Only three patients consented to be repeated for an additional aorta sonogram on the handheld ultrasound system. Those completed studies were analyzed postexamination and not concurrently with the bulk of images taken from the laptop ultrasound system. To complete a product assessment of the handheld ultrasound system as a diagnostic imaging tool for the aorta, the main user experience topics were utilized. These three main topics were presented by the Nielsen Norman Group in 2008: Utility, Usability, and Desirability (UUD) 19 The utility of the novel handheld ultrasound system was gauged by determining whether the product solves an established problem the user was looking to solve. 19 In the study, the researchers were trying to complete a sonographic assessment of a volunteer’s aorta in a confined space. The novel device was judged to determine whether it solved these confining issues, without compromising diagnostic quality. The recovery area adjacent to the CT examination suite was where the consenting, biomarkers, and sonography examinations were completed. Given the confined space, the novel handheld device was a more efficient and user-friendly method to working on the recovery cart (see Figure 4). In addition, the researchers had to determine the usability of the imaging system to record all the views needed to be able to grade the aorta, in all three regions. In this case, the product has to be easy and intuitive to use when completing the case. When completing the duplicate aorta cases for those consented patients, the handheld device was very easy to use and was quick to utilize for this research study. It also allowed for easy access to the images for postexamination measurements for easy image assessment and uploading. The last dimension explored with this product was desirability. This evaluative step requires that the user has been able to properly determine whether the experience has left a lasting impression. In this prepiloting of the handheld ultrasound system, the impression of our users (ANW, KDE, and IWB) was that we all looked forward to using the system for a quick and easy assessment. It also made the image assessment quite easy as uploading images to the DICOM viewer for measurement and grading was a simple process. The research team acknowledges that this UUD is qualitative in nature and only applies to the utilization that these researchers were able to conduct.
Researcher using the Philips Lumify Ultrasound system for an aortic risk assessment.
Given the size of the cohort, the power and effect of this analysis was very limited.
Discussion
Utilization of the Modified Grading System for AACs in the Adult Aorta
The modified grading system, translated from radiography and DXA, allowed for the researchers to assess AACs and the presence of atherosclerotic disease, in this convenient cohort of participants. The need to adjust the imaging presets and protocol, to include the vertebral bodies, was a change from the sponsoring hospital’s clinical scanning protocol. This was done to make sure that the aorta could be consistently segmented for each examination and also synchronize the grading process. The Multiethnic Study of Atherosclerosis used CT to determine the extent of AACs in adults and graded them with an Agatston score. Interestingly, this imaging technique and scoring system classified this age group to be at low risk. 20 The researchers found that AAC prevalence ranged from 34% in those aged 45–54 years to 94% (P < .0001) and was higher in Caucasians (79%) and lower in African Americans (62%; P < .0001). 20 Certainly, this is a much more rigorous study with greater statistical power and effect, but the use of CT and the Agatston score for this age group differed from the data collected in the present study. The value of having the entire length of the aorta on a CT image is advantageous; however, the slice thickness of the CT must be carefully selected to avoid missing the tiny calcific deposits in the arterial wall. The use of ionizing radiation techniques like CT, DXA, and radiography would not be supported for screening of asymptomatic patients in the 40- to 60-year age range. The present cohort pilot results are promising, and the grading system could be easily applied to all segments of the aorta imaged in an outpatient or primary care setting.
Quantitatively Assessing a-IMT in the Adult Aorta for Risk Assessment
In a study conducted by Koc & Sumbul, they found that a-IMT was increased in adults with diabetes mellitus (DM) and also increased with age. 21 They used sonography to image 114 adults with type II DM compared with 100 healthy controls and found that a-IMT values were strongly and positively correlated with age, systolic BP, blood urea nitrogen, DM onset time, and HbA1c levels (P < .05). 21 This study is much larger than the present study, but the presence of DM was not a factor in these results. However, age and BP were positively associated with a-IMT in this cohort. This is something that is not that surprising but needs to be further investigated as part of the next step in this line of inquiry.
Gauging the UUD to Expand on Documenting the User Experience With Handheld Sonographic Devices
The further use of laptop ultrasound units and the integration of handheld sonographic devices change many of the traditional ways of approaching screening populations for atherosclerotic disease. The use of handheld sonographic devices holds promise of making physicians front and center for screening their patients. The handheld sonographic device could potentially be used to assess AACs in underserved and remote populations, when they may otherwise not have accessibility to such assessments. When both the handheld unit and laptop ultrasound system were used to image the same patients, it was possible to compare the image quality of both systems. After both types of equipment and imaging sets were scrutinized, no significant differences were subjectively noted, regarding image quality. The limited assessment that was nested, as a product evaluation of the handheld sonographic device, is promising for this clinical application and needs UUD from a variety of other clinical users.
Limitations
Given the small size of this cohort, anticipated statistics were limited to frequency, means, and limited comparisons. In addition, IMT measurements were not electrocardiographically gated and measured manually by the ultrasonographer.
Conclusions
Further use of the modified grading system to assess the AAC and measurement of a-IMT is needed to better understand the clinical use of the discussed technique. In this particular cohort, it is possible to adequately visualize and assess plaque grade based on a modified scoring system. Although we were able to sufficiently visualize and evaluate plaque grade in our participants, further research is warranted with larger cohort size and comparison with clinical biomarkers, to assist in risk assessment and asymptomatic screening of 40- to 60-year-olds. Furthermore, more UUD data are needed to evaluate novel handheld sonographic devices within a clinical setting.
Footnotes
Acknowledgements
The authors would like to thank the collaborative working relationship with Nicholas T. Funderburg, PhD, and his virology laboratory.
Editor’s Note
The JDMS follows a scholarly, double-blinded peer review process. The peer review of this manuscript was managed by members of the JDMS Editorial Board and excluded the Editor listed as an author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are supported by funding by the ASRT Educational Foundation for this study and Dr Funderburg’s recruitment arm funded by the National Heart, Lung, and Blood Institute.