
Abstract
Drug-related pancreatitis is seen in only about 1.4%-2% of cases. Amiodarone is a commonly used medication for the treatment of different atrial and ventricular arrhythmias. Its common side effects include hepatotoxicity, thyroid dysfunction, and pulmonary fibrosis. Acute pancreatitis is a rare side effect of amiodarone. There are only a few cases reported worldwide of amiodarone causing acute pancreatitis as a side effect. We present a case of a 61-year-old female patient who, while receiving treatment for non-ST-elevation myocardial infarction with ventricular tachycardia and amiodarone, had abrupt nausea, vomiting, and epigastric soreness. A computed tomography scan of her abdomen revealed the classic features of acute pancreatitis, which led to the diagnosis. The common causes of pancreatitis were excluded by reviewing the patient’s medical history, lab results, and imaging. Since the pancreatitis symptoms started soon after beginning amiodarone, and no other cause was identified, we diagnosed the condition as amiodarone-induced pancreatitis. The patient’s symptoms completely disappeared within a week of stopping the medication. Given the high risk of complications and mortality from acute pancreatitis, and the simplicity of treating it by discontinuing amiodarone, this serious side effect should be identified promptly in appropriate clinical situations.
Introduction
Amiodarone, a class III antiarrhythmic agent under the Vaughan–Williams classification, is among the most widely used medications for managing a range of atrial and ventricular arrhythmias, primarily through its action of blocking potassium channels. Though amiodarone proves to be a powerful antiarrhythmic, its broad range of severe and sometimes fatal side effects has greatly constrained its role in modern medicine. Pulmonary fibrosis, liver damage, hypo- or hyperthyroidism, peripheral neuropathy, and other thyroid disorders are the most common and researched amiodarone adverse effects. 1 Although pancreatitis is an unusual and potentially fatal side effect of amiodarone, there have been very few reports of it in the global literature.2-6 Within 24 h of starting amiodarone treatment, one patient had acute pancreatitis, which is reported here.
Case Presentation
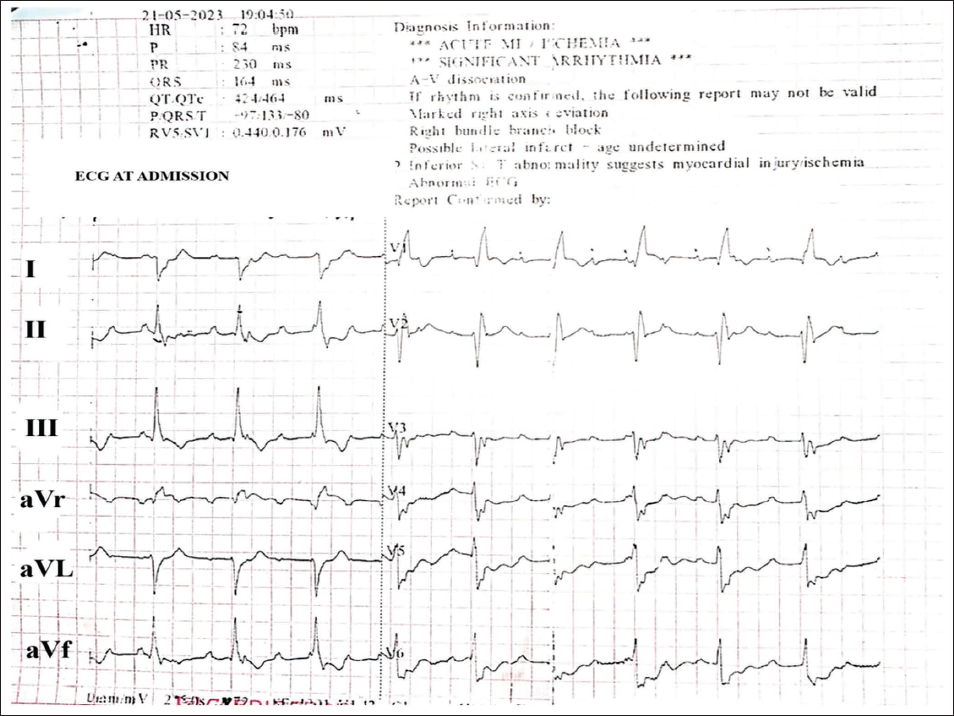
A 61-year-old female presented to the cardiology department after experiencing a single episode of syncope, which was followed by anginal pain and an insidious onset of dyspnea. She had no prior comorbidities or relevant cardiac history and denied substance abuse. The initial electrocardiogram revealed complete heart block with qRBBB, a ventricular rate of 50 beats/min, and changes suggestive of an evolved anterior wall myocardial infarction (Figure 1). On physical examination, vital parameters were blood pressure of 90/50 mmHg, heart rate of 50 beats/min, respiratory rate of 22 breaths/min, and oxygen saturation of 90% on room air. The patient was afebrile. Cardiorespiratory findings included normal heart sounds and bilateral basal crackles, while the examination of other systems was unremarkable. Troponin I levels were elevated at 5,490 ng/L upon admission, with all other blood parameters being normal, except for mildly elevated liver enzymes (Table 1). Echocardiography revealed grade II left ventricle (LV) diastolic dysfunction, mild global hypokinesia of the LV, and 45% left ventricular ejection fraction (LVEF), with the rest of the findings being normal.
Electrocardiogram at Admission Showing a Regular Ventricular Rate of Approximately 70 Beats/min. The Atrial P Waves (^ ) and Ventricular QRS (*) Complexes are Not Temporally Related, Consistent with Complete Heart Block. A qR Pattern with Broad QRS Complexes in Leads V1 and V2 is Suggestive of Right Bundle Branch Block Morphology, Indicating an Evolved Anterior Wall Myocardial Infarction. Corrected QT Interval is Prolonged.
She was treated conservatively with inotropes, dual antiplatelet therapy (DAPT) including aspirin with clopidogrel, atorvastatin, therapeutic enoxaparin, and oxygen support. Shortly after initiating treatment, she experienced two episodes of monomorphic ventricular tachycardia in the context of complete heart block (CHB). A stat dose of intravenous amiodarone (150 mg) was promptly administered, followed by the implantation of a temporary pacemaker set to a high output rate of 100 beats/min.
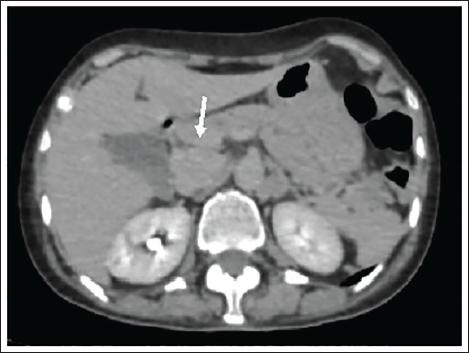
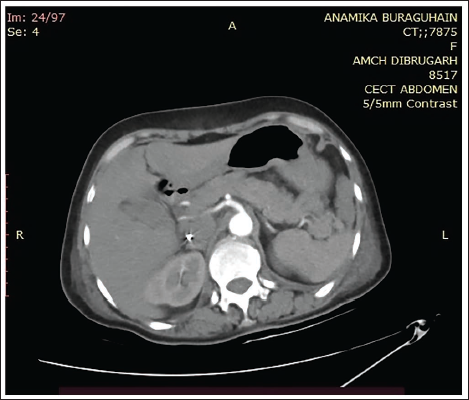
The following day, the patient developed acute abdominal pain, vomiting, epigastric tenderness, and hematuria. Dual antiplatelet therapy and enoxaparin were promptly discontinued. A clinical suspicion of acute pancreatitis was raised. Notably, there was no reported history of gallbladder stones, dyslipidemia, prior hospitalizations, or recent pharmacological interventions. The diagnosis was further substantiated by a contrast-enhanced computed tomography (CECT) scan of the abdomen, which demonstrated diffuse parenchymal enlargement and peripancreatic fat stranding, with no signs of obstruction or dilation of the biliary ducts (Figure 2). The patient was treated conservatively with intravenous fluids and pain management. Her symptoms resolved within the next 8-10 days, supported by normalization on repeat CECT abdomen (Figure 3).
The Contrast Enhanced Computed Tomography of the Abdomen (Taken at 3rd Day of Admission) Showing Edematous Head of Pancreas and Peripancreatic Fat Stranding (White Arrow).
The Contrast Enhanced Computed Tomography of Abdomen (Taken at Time of Discharge) Showing Normal Pancreatic Parenchyma.
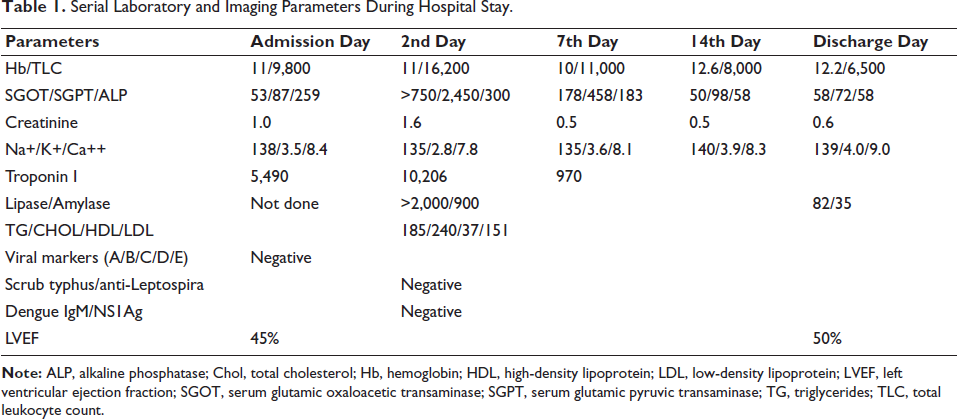
Serial Laboratory and Imaging Parameters During Hospital Stay.
We attempted to wean her off the temporary pacemaker, but she became pacemaker-dependent as her CHB did not resolve over the course of the illness. Due to acute pancreatitis, we were also unable to perform a coronary angiogram during hospitalization. In the end, we implanted a permanent pacemaker, set at 100 beats/min. We reintroduced atorvastatin at the lowest dose of 10 mg under strict supervision, gradually up-titrating the dose while monitoring both clinical and hematological profiles. There was no adverse event seen. Given the strong suspicion of amiodarone, we concluded that it was the likely cause of the acute pancreatitis.
She was eventually discharged on DAPT, atorvastatin (80 mg), metoprolol, diuretics, ramipril, dapagliflozin, and an antibiotic. Coronary angiography was advised during follow-up, but was not performed due to personal reasons.
Amiodarone can rarely precipitate acute pancreatitis, even within 24 h of initiation, and should be suspected once common causes are excluded. Early recognition and prompt withdrawal of the offending drug can result in complete clinical recovery and prevent further complications. Acute coronary syndrome complicated by complete heart block and ventricular arrhythmias may necessitate temporary pacing, with some patients requiring permanent pacemaker implantation due to non-reversible conduction abnormalities.
Discussion
Anyone with acute pancreatitis should seek immediate medical attention. Acute pancreatitis ranges from cases requiring conservative treatment to illnesses that are life threatening. The updated Atlanta Classification is used for the diagnosis of drug-induced pancreatitis (DIP), 7 just as it is for other types of acute pancreatitis. Two of the following must be present for a diagnosis to be made: typical imaging features, serum amylase or lipase values more than three times the upper limit of normal, or abdominal discomfort indicating pancreatitis. In order to diagnose the illness and rule out possible causes, a complete medical history is required.
The patient’s history, physical examination, and biochemical panel were all in agreement that the patient had acute pancreatitis, and the CT scan of the abdomen confirmed the diagnosis. In addition to not having a history of pancreatitis, our patient also did not display any of the typical risk indicators, including substance misuse. No gallstones or ductal dilatation were seen on CT scans, and there was no indication of a recent endoscopy, trauma, infection, or laboratory abnormalities that would indicate cholestasis or substantial hypertriglyceridemia in her medical history or investigations. At first, we suspected that atorvastatin and/or amiodarone could be contributing factors, given that there have been a few reported cases of both drugs causing acute pancreatitis within 24 h of initiation of therapy. But after resolution of signs and symptoms, we gave the lowest dose of statin, 10 mg and up-titrated the dose slowly to 80 mg (maximum dose at discharge) under continuous monitoring. There was no undesired event seen. So, it was most probably a case of amiodarone-induced acute pancreatitis.
Drug-induced acute pancreatitis presents similarly to pancreatitis from other causes, so it is not easily distinguishable. To make the diagnosis, at least two diagnostic criteria must be met, common causes must be ruled out, and there should be a clear connection to a medication known to trigger the condition. 8 Although the exact cause of DIP is still unclear, several theories have been proposed. 8 These include a weakened immune response, direct damage to pancreatic cells, narrowing of the pancreatic ducts, or the formation of blood clots in nearby arteries. Regardless of which mechanism is at play, the treatment approach remains the same. The primary focus is on removing the medication that triggered the condition, as this is the most crucial step in managing pancreatitis effectively.
Conclusion
Drug-induced acute pancreatitis is rare, but clinicians should consider it when a patient has pancreatitis without a clear cause. Being aware of medications that can trigger this condition can help in making the diagnosis. While many cases of DIP tend to have good outcomes, there can still be severe complications, so it is important not to ignore them.
This case discusses a patient who developed DIP after taking amiodarone, especially after other common causes of pancreatitis were ruled out. We want to emphasize how important it is to recognize and report cases of DIP to help raise awareness among healthcare providers. We also encourage researchers to study how drug-induced acute pancreatitis develops, so we can understand it better.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the relevant ethics committee or Institutional Review Board (IRB).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
All necessary patient permission documents have been received, as the authors attest. The patient or patients have indicated their approval for the publication of their photos and other clinical data in the journal on this form. Patients are informed that their identities will be kept confidential and that every effort would be taken to avoid publication of their names and initials; nevertheless, complete anonymity cannot be guaranteed.