
Abstract
Amiodarone is a broad-spectrum antiarrhythmic agent used in day-to-day practice to treat ventricular tachycardia (VT) and supraventricular tachycardias like atrial flutter/atrial fibrillation. 1 It can cause QT prolongation and rarely precipitate life-threatening ventricular arrhythmias like Torsade de Pointes (TdP). 1 Torsades is characterized by prolonged ventricular repolarization with QT intervals generally exceeding 500 milliseconds.1, 2 Risk factors for drug-induced QT prolongation are female sex, congestive heart failure, and so on. 2 This case report describes a woman with stress cardiomyopathy 3 and atrial fibrillation who was treated with Amiodarone which precipitated Torsades. Therefore knowledge of side effects, monitoring for drug effects, and timely withdrawal of the offending drug is important. 2
Introduction
Amiodarone belongs to the Class 3 Vaughan-William classification of anti-arrhythmic drugs. 1 It is a broad-spectrum antiarrhythmic agent used in clinical practice to treat ventricular tachycardia (VT), and atrial flutter/fibrillation. 1 Mechanism of action is K+ channel blockade which increases cardiac action potential duration and effective repolarization period and prevents arrhythmias, also exhibiting beta blockade and calcium channel blockade. 1 It can cause QT prolongation and rarely precipitate life-threatening ventricular arrhythmias like Torsade de Pointes (TdP). 1 Torsades is characterized by prolonged ventricular repolarization with QT intervals generally exceeding 500 milliseconds.1, 2 Risk factors for drug-induced QT prolongation are female sex, congestive heart failure, and so on. 2 This case report describes a woman with stress cardiomyopathy3–8 and atrial fibrillation who was treated with Amiodarone which precipitated Torsades.
Case Report
Day of Admission
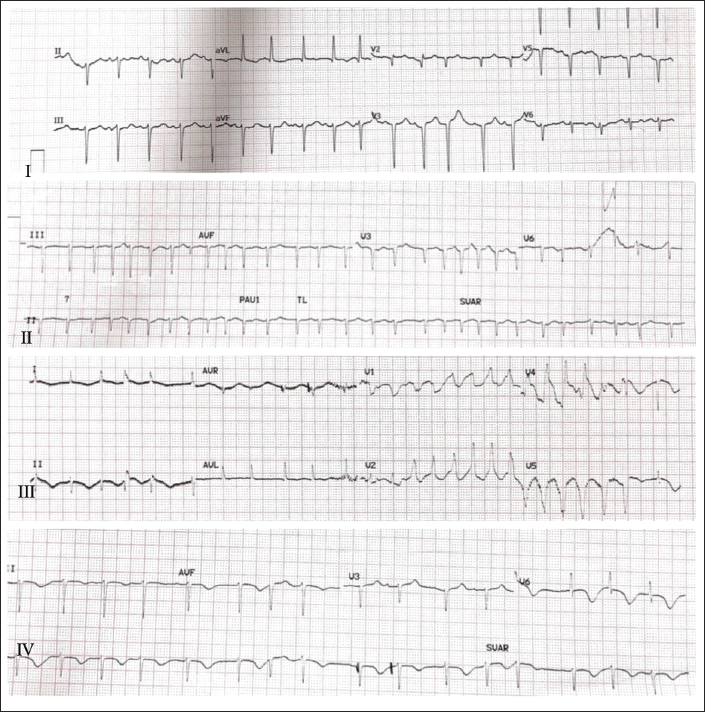
A 68-year-old female with a history of diabetes came to the hospital with complaints of dry cough for one week followed by uneasiness in chest 3 associated with shortness of breath3- Class 3 NYHA of one-day duration. She stays alone at home and has a history of anxiety disorder.3–8 On examination, she was slightly tachypnoeic at rest, pulse rate was 120 per min, BP was 110/80 Hg, Sats 92% on room air, bilateral basal crypts were heard at end inspiration. ECG showed ST elevation in lead aVR, and Q waves in anterior leads with no reciprocal changes with poor R wave progression.3, 4 QTc was 458 milliseconds.3, 4 CBP showed high total leukocyte count of 16,000 with serum electrolytes in normal range (K+ 3.7, Ca+ 9.4, Mg2+ 2.3). 2DECHO showed severe LV dysfunction (EF = 31%) and RWMA with akinetic apical and mid segments and well-contracting basal segments.3–8 CT chest showed B/L mild pleural effusion with mild pericardial effusion.
Troponin I was 0.16 (normal 0−0.12 ng/mL)3, 4 and repeat Troponin I after 3 h was 0.25 which showed Troponin elevation of 1 to 2 times upper limit of normal. NTpro BNP was 1,498 (normal 0−125 pg/mL).3, 4 InterTAK score was 78.3, 4 Patient was provisionally diagnosed with stress cardiomyopathy and treated with oxygen support, IV diuretics, IV anticoagulation, and other supportive care. 9
After a few hours of hospitalization, there was a worsening of SOB requiring BIPAP support. ECG showed atrial ectopics and short runs of atrial tachyarrhythmia which progressed soon to atrial fibrillation with fast ventricular rate. BP was 90/60 requiring mild Ionotropic support. 1 Amiodarone was given. A bolus dose of 150 mg stat followed by Amiodarone infusion at 1 mg/kg/h. There was a slowing of ventricular rate from 160 to 130 beats per min. 1
Day 2
On the successive day, the patient had repeated brief episodes of seizure-like activity with unresponsiveness during which the ECG monitor showed a short run of ill-sustained VT.1, 10, 11 12 lead ECG showed QT prolongation with QTc of 695 with R on T phenomenon leading to run of ill-sustained VT.1, 10
Considering the possibility of Amiodarone-induced VT, Amiodarone infusion was stopped immediately. Inj. Lignocaine 30 mg IV bolus and Inj. Magnesium Sulphate 2 g IV was given. Serum electrolytes were sent and found to be in the normal range (Na+ 144, K+ 3.5, Cl 104).
Day 3
Pt did not have a recurrence of VT after withholding amiodarone infusion. QTc came down to 613 milliseconds.
Day 4
Subsequently, the patient was treated with GDMT for heart failure and showed clinical improvement. There was no recurrence of VT episodes during further hospital course. CAG was done for risk stratification which showed no significant CAD.
Day 7
QTc was 574 milliseconds at discharge
Discussion
Stress cardiomyopathy3–8 is a common clinical entity in today’s practice in various clinical settings. A variety of triggers, physical and emotional, have been described to cause Stress cardiomyopathy.3, 4 In this patient, Stress Cardiomyopathy was entertained as a working diagnosis on grounds of history (past history of anxiety disorder),3, 4 age, and sex category (post-menopausal woman).3, 4 ECG findings described in Stress cardiomyopathy like ST segment elevation in lead aVR and absence of reciprocal ST segment depressions are seen in this patient.3, 4 2D Echocardiography showed Severe left ventricular dysfunction and apical ballooning and well-contracting basal segments.3–8 InterTAK diagnostic score was 78 (>70 indicates stress cardiomyopathy). 4 Other corroborative findings include mild Trop I elevation and raised NTproBNP levels.3, 4 Atrial fibrillation is the most common arrhythmia in Takotsubo Syndrome and has been reported in about 5% to 15% of patients.11, 12 This is a poor prognostic sign and is associated with lower left ventricular ejection fraction higher incidence of cardiogenic shock, and cardio-embolic events.11, 12
For the atrial fibrillation, the patient was started on rate, rhythm control, and thromboprophylaxis. 1 Beta Blockers could have been ideal in this situation except for hypotension. 1 Therefore, Amiodarone with less hemodynamic impact was chosen. 1 There was initial clinical improvement. However, the later clinical course was complicated by the occurrence of ill-sustained VT leading to hemodynamic compromise. There was a marked prolongation of QT interval noticed following Amiodarone administration which probably precipitated Torsades. 2 Other possible causes (dyselectrolytemia and ischemia) were ruled out. The clinical course stabilized after the withdrawal of Amiodarone with no further episodes of VT. Moreover, a slow reduction of QT interval duration was observed in the following days. 1 Additionally, QT interval prolongation has been reported in 4%−9%3, 4 of cases of Stress Cardiomyopathy. Therefore, after all the above observations, we believe that the event of ventricular tachyarrhythmia was precipitated due to combined QT prolonging effects of Amiodarone and stress cardiomyopathy (as it is independently known to cause QT prolongation).
Amiodarone is used extensively in clinical practice although QT prolongation is well-known to occur. This is due to its least pro-arrhythmic potential. However, Amiodarone is prophylactically withdrawn when QTc is greater than 550 milliseconds. Stress cardiomyopathy is a common clinical condition requiring ICU medical care, it is debatable if amiodarone is safe in these cases considering our experience. Does this warrant a lower threshold for drug withdrawal that is, at a lower QTc in cases of stress cardiomyopathy? Whether or not additional diagnostics should be sought before administering Amiodarone in stress cardiomyopathy?
Conclusion
The patient suffered a life-threatening cardiac arrhythmia because of an interplay of factors such as stress cardiomyopathy and QT-prolonging drugs (Amiodarone in this case). This case report has brought to light once again that although amiodarone has the least pro-arrhythmic properties, it is not devoid of it especially when another arrhythmogenic factor co-exists.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance is not required as this is a retrospective case study and it is not a human or animal study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Consent is not applicable as this is a retrospective case report and there is no disclosure of identity.