
Abstract
Objective
To investigate the prevalence and characteristics of coronary artery disease in a cohort of young adults (<45 years) using coronary computed tomography angiography and to integrate these local findings with the established literature.
Methods
We retrospectively analyzed 184 consecutive patients aged 18-45 years who underwent coronary computed tomography angiography for the investigation of chest pain or cardiovascular risk stratification. The cohort included both symptomatic individuals and asymptomatic patients with established risk factors. The data extracted included coronary artery calcium score, luminal stenosis, plaque morphology, and congenital anomalies.
Results
The mean age was 38 years; 79.3% were male. Normal coronary arteries were found in 72.3% (n = 133). Subclinical atherosclerosis was detected in 27.7% (n = 51), with obstructive coronary artery disease (≥50% stenosis) in 8.2% (n = 15). A non-zero coronary artery calcium score was present in 12.5% (n = 23), with values up to 549. High-risk, non-calcified plaques were observed even in patients with a zero coronary artery calcium score. Myocardial bridging was identified in 22% of the cohort.
Conclusion
Although the overall prevalence of obstructive coronary artery disease is low in young Indian adults, subclinical atherosclerosis and high-risk plaque features are not uncommon. Coronary computed tomography angiography enables early identification of these abnormalities and should be considered in the targeted evaluation of high-risk young patients in India.
Keywords
Introduction
Atherosclerotic cardiovascular disease remains a leading cause of mortality globally, yet current prevention strategies often fail to identify at-risk individuals, particularly those at a younger age. The paradigm of risk assessment is largely built on predictive algorithms, such as the Framingham Risk Score, which were developed using older populations and often overlook the early stages of disease development in young adults. This oversight is a critical gap, especially given the documented increase in the incidence of acute myocardial infarction (AMI) in younger populations (ages 35-54) over recent decades. 1 Identifying and intervening in these individuals early on offers the greatest potential for reducing lifetime cardiovascular disease (CVD) risk.
The development of subclinical atherosclerosis begins much earlier in life than previously thought. The Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study revealed that fatty streaks and fibrous plaques are already present in the coronary arteries of adolescents and young adults.2, 3 Traditional markers like coronary artery calcium (CAC), measured by non-contrast computed tomography (CT), provide a reliable indicator of established atherosclerosis.4, 5 While a CAC score of zero in an older patient portends a good prognosis, it is less reliable in younger individuals, as non-calcified plaques, which are precursors to calcified lesions, may be present and undetected.6, 7
Coronary computed tomography angiography addresses this limitation by providing a detailed anatomical visualization of the coronary arteries, allowing for the detection and characterization of both calcified and non-calcified plaques. Studies have shown that coronary computed tomography angiography (CCTA) can identify significant coronary abnormalities in up to 22% of young adults presenting with chest pain, yet obstructive stenosis (>50%) is rare, occurring in only about 2.8% of these cases. 8 A crucial finding from this research is that factors such as age and male sex are significant predictors of the presence of coronary artery disease (CAD) in this younger demographic. Furthermore, a family history of premature CAD has emerged as a particularly strong independent predictor of the presence of both non-calcified and calcified plaque in young patients. 9
This article combines a local cohort analysis of CCTA findings in young adults with a review of current literature to assess the role of CCTA in this population. We aim to highlight the value of CCTA beyond simple risk stratification, focusing on its ability to detect subclinical disease, characterize plaque morphology, and identify congenital anomalies that may be the true cause of a patient’s symptoms.
Methods
Patient Cohort
This was a retrospective analysis of CCTA reports from 184 consecutive patients aged 18-45 years. Patients were included if they were referred for CCTA due to clinical symptoms (e.g., chest pain, equivalent symptoms) or for risk assessment in the setting of established cardiovascular risk factors (e.g., hypertension, diabetes). Patients were categorized based on their primary indication for imaging as either “Symptomatic” or “Asymptomatic with Risk Factors.” The reports were retrieved from our Picture Archiving and Communication System (PACS) for CCTA studies conducted between September 2023 and September 2025.
Data Extraction and Categorization
From each report, the following data points were systematically extracted: patient demographics (age and gender), coronary artery calcium score (CACS), CAD findings (stenosis presence, location, and severity), plaque characteristics, and anatomical variants and congenital anomalies. Plaque morphology was assessed, with “high-risk features” defined as the presence of positive remodeling, low-attenuation plaque (<30 HU), or spotty calcification, consistent with established CCTA criteria.
Literature Review
A targeted literature search was performed using research articles on Google Scholar to contextualize our findings. The search focused on the role of CCTA in young adults, the prognostic value of CACS and plaque morphology, and the prevalence of subclinical atherosclerosis in this age group. Key studies identified include those from the Coronary Artery Risk Development in Young Adults (CARDIA) study and other multicenter registries.8, 9
Results
Patient Demographics
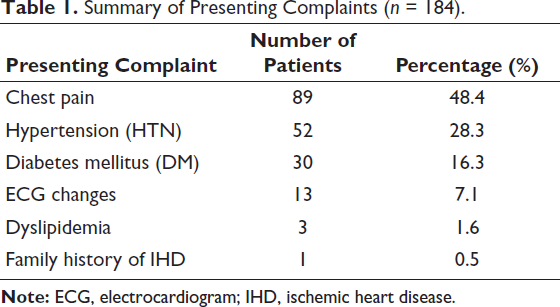
A total of 184 CCTA reports for patients aged 18-45 years were analyzed. The mean age of the cohort was approximately 38 years, and the population was predominantly male (146/184; 79.3%), with females comprising 20.7% (38/184). The clinical indications for CCTA are summarized in Table 1. The most common presenting complaint was chest pain, reported in nearly half of the patients (48.4%, n = 89). This was followed by established cardiovascular risk factors, including hypertension (28.3%, n = 52) and diabetes mellitus (16.3%, n = 30), underscoring the symptomatic and at-risk nature of this young adult cohort.
Summary of Presenting Complaints (n = 184).
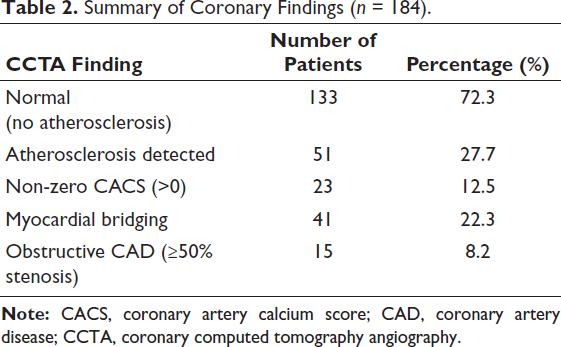
The principal CCTA findings for the 184-patient cohort are summarized in Table 2. While the majority of patients (72.3%, n = 133) had normal coronary arteries with no evidence of atherosclerosis, subclinical disease was detected in over a quarter of the cohort (27.7%, n = 51).
Summary of Coronary Findings (n = 184).
Coronary Artery Calcium Score Analysis
The analysis of this cohort revealed a pronounced bimodal distribution of CACS. The overwhelming majority of patients presented with a score of 0, indicating an absence of detectable coronary artery calcification. However, a small but clinically significant number of patients demonstrated elevated CACS, indicating established and often advanced atherosclerotic disease. In one extreme case, a CACS of 549 was observed. Other high coronary calcium scores were 278, 220, and 166.
Prevalence and Severity of Stenosis
Consistent with the CACS findings, the majority of the reports for this cohort indicated “no significant focal luminal stenosis.” For those patients with the disease, the spectrum of stenosis ranged from mild to moderate to severe. The most severe stenoses were observed in the patients with the highest CACS. For instance, a 44-year-old male had near-total occlusion in the mid left anterior descending (LAD) and severe stenoses of 70%-80% in the distal LAD and 75%-85% in the mid right coronary artery (RCA). Another patient had 80%-90% focal luminal stenosis of the ramus intermedius, a critically high degree of narrowing.
Plaque Morphology and High-risk Features
The CCTA reports provided valuable detail on plaque composition. The presence of “high-risk plaques” was noted in reports of patients with severe disease, such as a 44-year-old male patient in the study. These plaques were characterized as soft or mixed, carrying a higher risk of rupture.6, 10 The data from our cohort reinforce that non-calcified and low-attenuation plaques are present even in young adults with non-obstructive CAD, highlighting the limitations of relying solely on CACS for risk assessment.
Non-atherosclerotic Findings
Coronary computed tomography angiography’s utility in this young cohort extends beyond atherosclerosis to the detection of anatomical variants and congenital anomalies. Myocardial bridging was a particularly common finding, present in 22.3% of the young patients, often in the mid-to-distal LAD. In some cases, rare and clinically significant congenital anomalies were identified, such as anomalous left coronary artery from the pulmonary artery (ALCAPA) and anomalous origins of other coronary arteries.
Discussion
The findings from this single-center cohort, in conjunction with the provided research, underscore the evolving role of CCTA in evaluating young adults. The high prevalence of normal coronary arteries in our cohort aligns with expectations for this age group. However, the presence of subclinical atherosclerosis in a substantial minority of these patients (27.7%) challenges the notion that young age alone is a guarantee of a disease-free coronary tree. A previous study corroborates this, with 22% of young adults having a coronary abnormality on CCTA. 8
The CARDIA study established that any measurable CAC in adults aged 32-46 years is associated with a significantly increased risk of incident coronary heart disease (CHD) and all-cause mortality over a 12.5-year follow-up. 11 Our finding of patients with non-zero CACS, including some with very high scores, suggests that these individuals are at a similarly elevated risk and may benefit from aggressive risk-factor modification and lifestyle changes.
The CCTA reports in our cohort provided valuable information on plaque morphology, with some cases explicitly flagging “high-risk plaques” despite a low CACS. This supports the argument that CCTA offers a more complete picture of atherosclerotic burden than CACS alone. Non-calcified plaques and low-attenuation plaques, which are rarely associated with calcification, are strong predictors of future myocardial infarction and are more prevalent in patients with obstructive CAD.9, 12
Our analysis of myocardial bridging and congenital anomalies highlights another significant advantage of CCTA. For symptomatic patients, particularly young ones with a low likelihood of traditional CAD, identifying a myocardial bridge can provide a definitive diagnosis for their chest pain. 13
Limitations
This study has several limitations inherent to its retrospective single-center design. First, while CCTA provides detailed anatomical information, data regarding functional ischemia testing (such as treadmill testing or stress echocardiography) were not available for correlation in this dataset. Consequently, the hemodynamic significance of the intermediate stenoses identified remains to be fully characterized.
Second, while traditional risk factors like hypertension and diabetes were recorded, comprehensive lipid profiles—specifically Lipoprotein(a) [Lp(a)] and Apolipoprotein B levels—were not available for analysis. Given the emerging importance of Lp(a) as a residual risk factor in young adults, future prospective studies in this population should include these biomarkers to better define the metabolic risk profile. Finally, the definition of “high-risk” patients in this cohort was based on clinical referral patterns for CCTA rather than a pre-specified prospective risk score, which may introduce selection bias.
Conclusion
The data from our cohort analysis, supported by a synthesis of major research articles, show that while obstructive CAD is rare in young adults, subclinical atherosclerosis and other cardiac abnormalities are not. Coronary computed tomography angiography is uniquely positioned to identify these early-stage pathologies, which are often missed by traditional risk scores and CACS alone. The low prevalence of significant disease in this group makes a universal CCTA screening program currently unwarranted. However, a targeted approach for young adults with a strong family history of premature CAD or multiple conventional risk factors could significantly improve long-term cardiovascular outcomes. 14
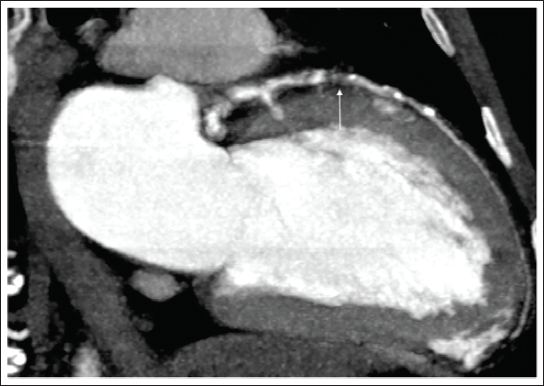
Coronary Computed Tomography Angiography Maximum Intensity Projection (MIP) Image Showing Total Occlusion in mid-Left Anterior Descending (LAD) Artery for Approximately 20 mm Marked as White Arrow.
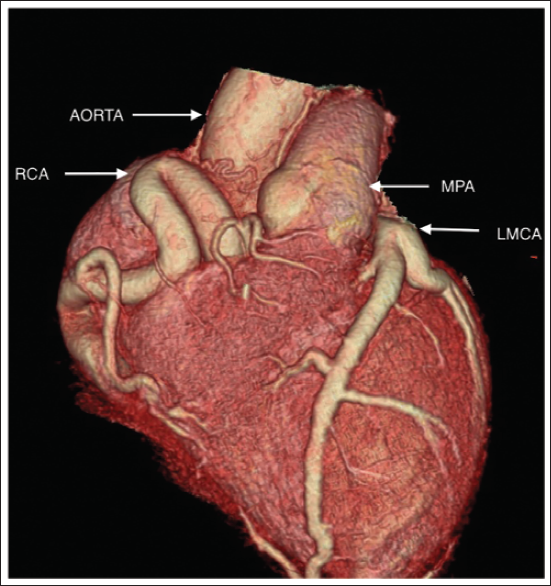
Volume Rendering Image Showing Anomalous Origin of Aneurysmal Left Main Coronary Artery (LMCA) from Main Pulmonary Artery (MPA). Also Shown Aorta and Aneurysmal Left Coronary Artery (LCA).
Footnotes
Acknowledgment
The authors would like to thank the Department of Radiology, Cardiology and Emergency Medicine at Kailash Hospital and Heart Institute, Noida, for their support and assistance in the facilitation of this research.
Authors Contribution
Manoj Kumar Sharma: Conceptualization, methodology, writing—original draft, supervision.
Ashish Manohar: Data curation, investigation, writing—review & editing.
Kanchan Varma: Data curation, formal analysis, writing—review & editing.
Consent to Participate
Not applicable. The requirement for informed consent to participate was waived by the Institutional Ethics Committee for this retrospective study.
Consent for Publication
Not applicable. All patient data and images (e.g., Figures 1 and ![]() ) included in this manuscript have been fully de-identified, and all potentially identifying details have been omitted to ensure patient anonymity.
) included in this manuscript have been fully de-identified, and all potentially identifying details have been omitted to ensure patient anonymity.
Data Availability Statement
The data that support the findings of this study are derived from patient medical records and are therefore not publicly available due to privacy and ethical restrictions. Anonymized data may be available from the corresponding author upon reasonable request and with the permission of the Institutional Ethics Committee of Kailash Hospital and Heart Institute.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Patient Consent
This study is a retrospective analysis of existing medical reports and images. The study protocol was reviewed and approved by the Institutional Ethics Committee of Kailash Hospital and Heart Institute, Noida. The committee waived the requirement for individual patient consent due to the retrospective and anonymized nature of the data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.