
Abstract
A thromboembolic event in nephrotic syndrome often develops over time. Cerebral venous thrombosis is a rare initial complication in adults with membranous nephropathy. Our 39-year-old male patient had prior cerebral and renal vein thrombosis and presented with right heart failure, hypotension, and tachycardia. He was found to have bilateral pulmonary artery thromboses and right ventricular dysfunction. After alteplase thrombolysis failed, a catheter thrombectomy was performed. Further testing, due to recurrent thrombosis and leg swelling, showed nephrotic proteinuria and positive anti-phospholipase A2 receptor antibodies, diagnosing primary membranous nephropathy. Treated with steroids and anticoagulants, he responded well, with reduced proteinuria, improved serum protein C and S, and no further thromboembolic events.
Keywords
Background
Nephrotic syndrome is a clinical spectrum involving a nephrotic range of proteinuria, hypoalbuminemia, peripheral edema, hyperlipidemia, and increased risk of venous thromboembolism (VTE). 1 Primary membranous nephropathy (MN) is known for its adult-onset nephrotic syndrome and its thrombotic complications. Renal vein thrombosis, deep vein thrombosis, and pulmonary embolism are frequent VTE complications in MN and typically develop over the course of the disease. 2 A thromboembolic phenomenon as an initial presentation of nephrotic syndrome is exceedingly rare. Here we present a rare case of recurrent thrombosis in a quadragenarian male with MN involving the cerebral vein, renal vein, and pulmonary arteries, presenting with congestive heart failure symptoms.
Case
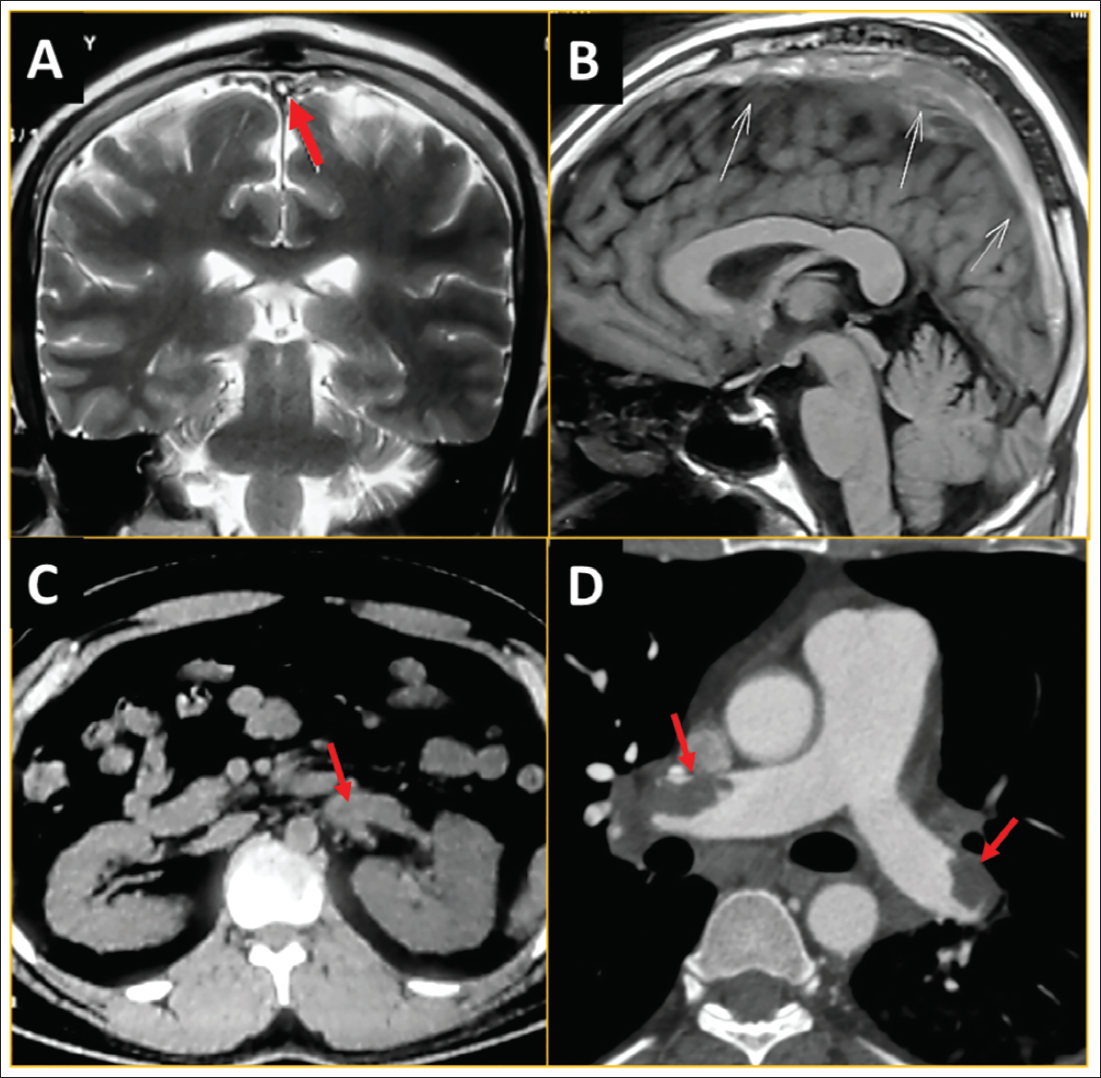
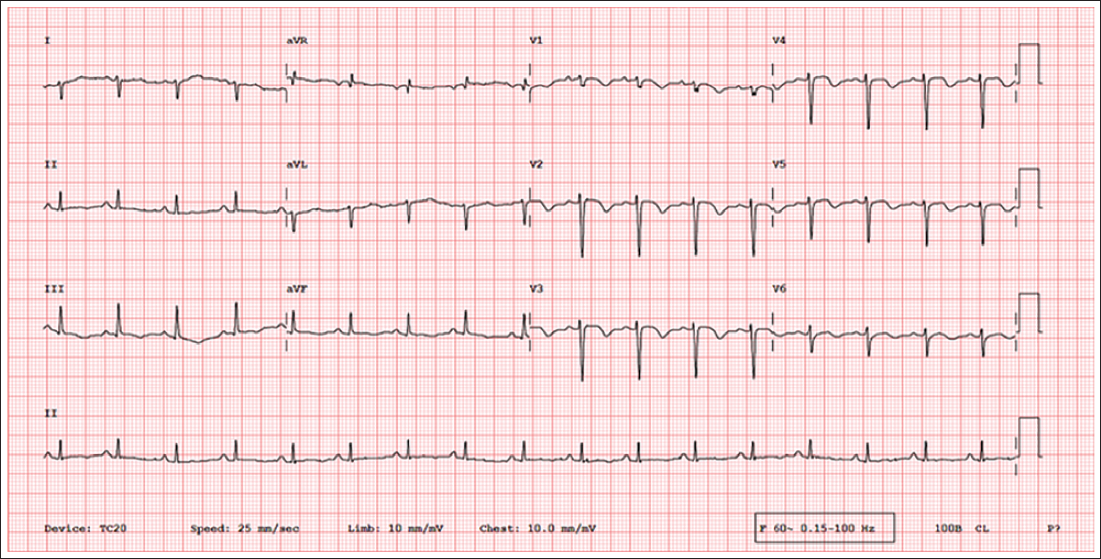
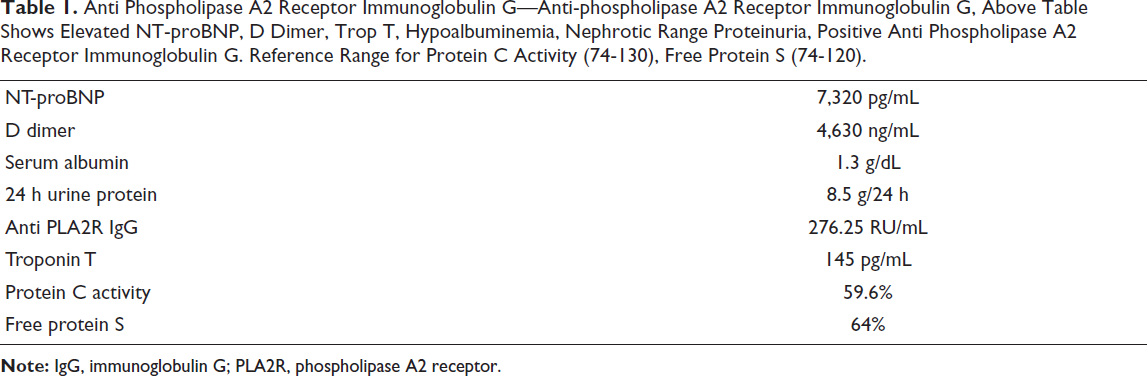
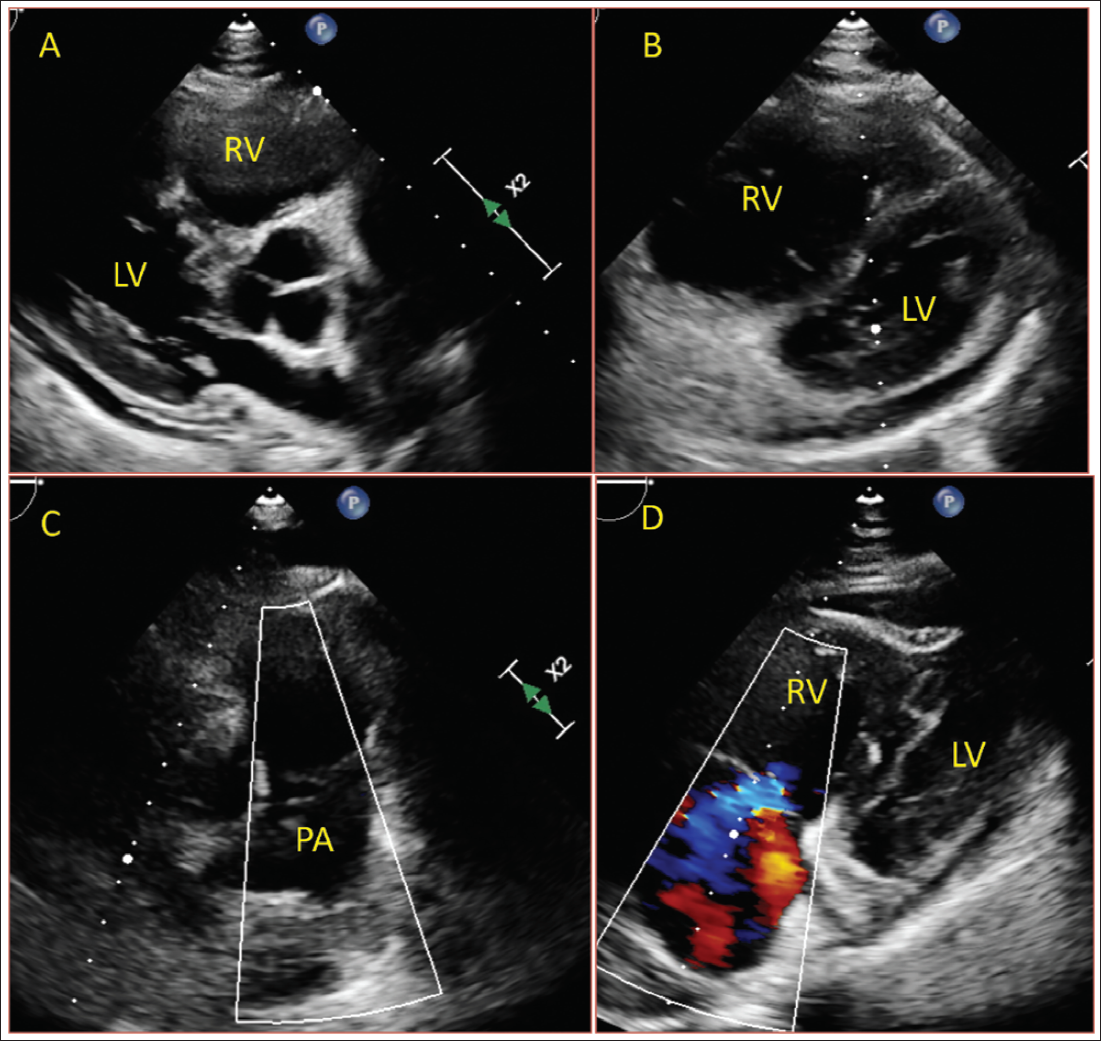
A 39-year-old male had a history of cerebral vein thrombosis (Figure 1A and 1B) a year ago, attributed to alcohol use, and was initiated on oral anticoagulants. Six months later, he was diagnosed with left renal vein thrombosis (Figure 1C). The cause of thrombosis was not evaluated during the course. He currently presented with worsening dyspnea on exertion for the past 2 weeks, associated with abdominal distention and swelling of the lower limbs. A diagnosis of congestive heart failure with a thrombotic complication was made. On clinical examination, he had desaturation in room air (88%), tachypnea, tachycardia, hypotension, elevated jugular venous pressure, and a loud pulmonary component of the second heart sound with narrow split and right ventricular S3. An electrocardiogram revealed sinus tachycardia with an S1Q3T3 pattern (Figure 2) and right ventricular strain. His D-dimer, NT-proBNP, and troponin T levels are shown in Table 1. Echocardiography showed McConell’s sign, severe right ventricle (RV) dysfunction, with severe pulmonary hypertension (Figure 3, Supplementary video 1). A computed tomography (CT) pulmonary angiography showed right and left pulmonary artery thrombosis (Figure 1D). A Doppler of the lower limb ruled out deep vein thrombosis. Given failed systemic thrombolysis with alteplase, a catheter-directed thrombectomy using a Penumbra Lightning device was performed. This led to echocardiographic and clinical improvement over the next week. In view of long-standing leg swelling with a history of recurrent venous thrombosis and hypoalbuminemia, a 24-h urine protein was ordered, which indicated nephrotic range proteinuria (8.5 g/day). Anti-phospholipase A2 receptor (PLA2R) antibody was positive, and he was diagnosed with primary MN and treated with pulse steroids. Laboratory investigations, including antinuclear antibody, anti-double-stranded deoxyribonucleic acid (DNA), antiphospholipid, anticardiolipin, homocysteine, factor V Leiden mutation, hepatitis C, human immunodeficiency virus, and hepatitis B antigen, were negative. He is currently on a novel oral anticoagulant and steroids. His response to treatment was good, evidenced by a decrease in proteinuria and an increase in serum protein C and protein S activity during follow-up, with no further thromboembolic episodes.
Anti Phospholipase A2 Receptor Immunoglobulin G—Anti-phospholipase A2 Receptor Immunoglobulin G, Above Table Shows Elevated NT-proBNP, D Dimer, Trop T, Hypoalbuminemia, Nephrotic Range Proteinuria, Positive Anti Phospholipase A2 Receptor Immunoglobulin G. Reference Range for Protein C Activity (74-130), Free Protein S (74-120).
Discussion
Membranous nephropathy patients exhibit a significant risk of VTE events, with a reported incidence of 7.2%. 3 Venous thromboembolism is more prevalent than arterial thromboembolism in MN. The mean time to development of the first VTE from the initial assessment of proteinuria is approximately 3.8 months. 3 It is uncommon for VTE to precede the diagnosis of nephrotic syndrome.3, 4 The most frequent VTE sites in MN patients involve the renal vein, deep veins of the legs, and pulmonary embolism.1, 2, 4 Less common VTE sites include the splenic vein, portal vein, cerebral venous sinuses, internal jugular vein, and vena cava, primarily reported in pediatric cases. 1 Cerebral venous sinus thrombosis is a rare complication in adults with MN, with only one reported case associated with a factor V Leiden mutation, a known risk factor for venous thrombosis. 5 Nephrotic syndrome patients exhibit an increased propensity for VTE due to several interrelated factors. The excessive filtration of small proteins, including antithrombin III, plasminogen, protein C, and protein S, leads to a hypercoagulable state. Additionally, hypoalbuminemia, dyslipidemia, platelet dysfunction, increased platelet aggregation and adhesiveness, impaired fibrinolysis, and elevated hepatic production of coagulation factors, fibrinogen, and thrombin all contribute to thrombus formation.1-3, 5, 6 Serum albumin levels have been identified as a strong independent predictor of VTE risk in patients with nephrotic syndrome. 3 Individuals with serum albumin concentrations below 2.8 g/dL demonstrate a 2.5-fold increased risk of VTE compared to those with levels above 2.8 g/dL. This association is likely attributed to albumin’s role as a cofactor in the binding of plasminogen to fibrin and its interaction with tissue plasminogen activator. Consequently, hypoalbuminemia results in defective fibrinolysis. 3 While age, sex, race, serum creatinine, estimated glomerular filtration rate (eGFR), smoking exposure, and proteinuria have been evaluated as potential predictors of VTE risk, they have not been found to be significant factors.
Our patient presented initially with cerebral venous sinus thrombosis (CVT), which was attributed to alcohol use disorder, followed by renal vein thrombosis, and subsequently developed a pulmonary embolism. The initial presentation of venous thrombosis, particularly in rare territories, and a congestive heart failure mimicker in presentation, makes this case exceptional for an MN patient. The patient received a modified Ponticelli regimen, resulting in remission and a favorable clinical outcome.
Conclusion
Cerebral venous thrombosis can serve as the initial manifestation of MN. Leg swelling associated with pulmonary embolism may not exclusively be attributed to right ventricular dysfunction but could potentially be indicative of an underlying nephrotic syndrome.
Learning Points
Membranous nephropathy can have thrombotic complications.
Cerebral venous thrombosis is a potential complication and should be considered in the diagnosis.
Thrombosis in young patients warrants thorough cause evaluation, as it might be reversible.
Three thrombotic events in a patient highlight the disorder’s thrombotic burden.
Footnotes
Authors Contribution
SS: Conceptualization, formal analysis, writing—original draft, writing—review & editing. SM: Conceptualization, formal analysis, writing—original draft, writing—review & editing. JV: Writing—review & editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the relevant ethics committee or Institutional Review Board (IRB).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Obtained from the patient in line with COPE guidance.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.