
Abstract
Cardiovascular disease represents a significant and growing public health challenge in India, with a notably higher burden of premature deaths compared to global averages. Concurrently, influenza infections contribute substantially to this burden by triggering cardiovascular complications, particularly among high-risk individuals. Despite evidence supporting the cardioprotective benefits of influenza vaccination, its integration into standard cardiology practice remains inconsistent. This consensus aims to deliver a comprehensive and detailed summary of the impact of influenza infections on cardiovascular disease, particularly in the Indian context, and to advocate for the adoption of influenza immunization as a defense against cardiac distress. The findings emphasize the importance of influenza vaccination in reducing the incidence of acute coronary syndrome, myocardial infarction, and other severe cardiovascular complications. It also discusses expert opinions concerning the role of vaccination against influenza in cardiovascular disease patients, highlighting the necessity of broader implementation in high-risk populations.
Keywords
Introduction
The severity of the cardiovascular disease (CVD) epidemic in India reflects a significant global health challenge, characterized of diseased by higher relative risk (RR) load, earlier onset, increased case fatality, and a higher incidence of premature deaths. 1 The prevalence of influenza infections accounts for around 39 million cases each year globally. India manages a noteworthy yearly caseload because of its tropical climate and several lifestyle options. 2 Influenza infections can initiate processes that may impact cardiovascular health, especially in individuals at high risk of morbidity and mortality due to cardiovascular risk factors or established CVD. 3 Evidence from epidemiological studies and their systematic reviews and meta-analyses consistently demonstrates a significant relation between respiratory infections and acute coronary syndrome (ACS) incidence and CV mortality.4, 5
Influenza epidemics result in a substantial burden of mortality and CV complications, posing an elevated risk for patients with chronic CV conditions. A recent position statement issued by the Cardiology Society of India regarding COVID-19 and heart failure (HF) has underscored the profound relationship between respiratory infections and CVDs. 6 Over the past 15 years, the administration of influenza vaccine has proven to be a successful method to lower the incidence of respiratory infections and the associated CV complications in high-risk populations. Numerous studies analyzed the impact of influenza vaccination (IV) on the risk of cardiovascular events. The European Society of Cardiology, the American Heart Association, the American College of Cardiology, as well as the World Health Organization (WHO), have strongly recommended annual IV for CVD patients. Despite its effectiveness, the incorporation of IV into standard cardiology practice remains inconsistent, leading to varying vaccination rates among high-risk populations worldwide.7, 8
The primary objective of this consensus regarding influenza immunization as a CV prevention strategy is based on contemporary evidence and clinical expertise. This comprehensive review was crafted to underscore the impact of influenza on CVD, the importance of immunizing CVD patients against influenza, and the barriers to the implementation of IV to improve vaccination uptake among these patients in our region.
Method
An advisory meeting with four key Indian experts in the field of cardiology was planned to improve understanding of the importance of immunization against influenza for preventing CVD. The experts discussed the scientific evidence and clinical insights on the role of IV in patients with ACS, HF, and atrial fibrillation (AF). A thorough literature search was carried out using databases such as PubMed, Cochrane, and Google Scholar was conducted using the keywords “IV,” “myocardial infarction (MI), ACS,” “HF,” and “AF.” In addition, current guidelines on IV in CVD patients were critically reviewed to provide context and evidence-based recommendations. The experts participating in the advisory meeting were renowned cardiologists with extensive clinical experience of at least 25 years, multiple peer-reviewed publications, and active contributions to academic teaching, guideline development, or scientific advisory boards. They had also participated as speakers or panelists in national and international scientific conferences and held key positions in professional cardiology societies. Following the meeting, a descriptive analysis was performed, integrating the findings from the literature review with the insights and clinical perspectives of the experts, providing a comprehensive overview of the significance of IV in individuals with heart disorders.
The Burden of Influenza on Cardiovascular Diseases
Cardiovascular diseases, including conditions like heart disease and stroke, result in approximately 17.7 million deaths globally, with India accounting for a significant share, particularly among the younger population. The age-related CVD mortality rate in India is 272 per 100,000 individuals, exceeding the global average of 235 people. This condition manifests approximately a decade earlier compared to Western people. Key concerns for Indians include early onset, rapid progression, and elevated mortality rates associated with CVD. Despite conventional risk factors, the Indian population exhibits the world’s highest rates of coronary artery disease (CAD). 9
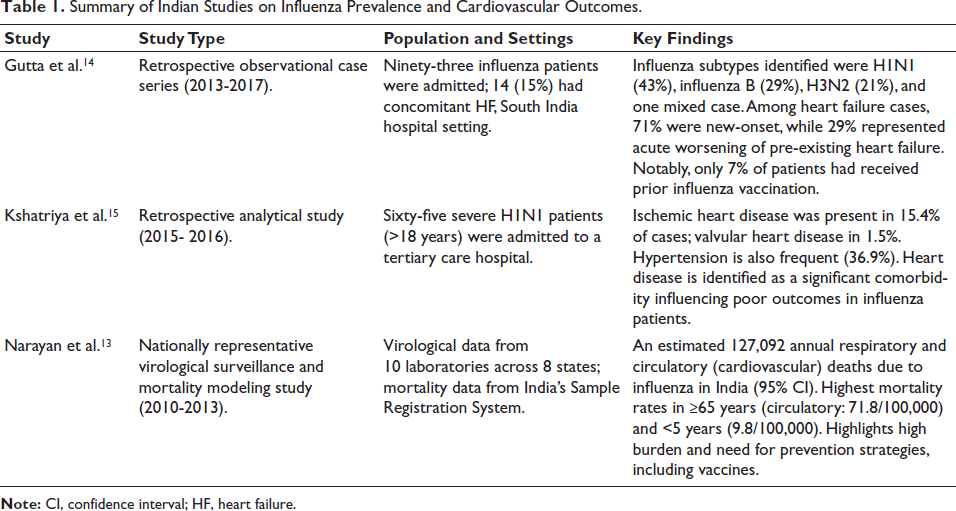
India experiences a significant prevalence of ischemic heart disease (IHD), resulting in 36.99 million disability adjusted life years and 1.54 million deaths. In 2017, the Global Burden of Disease (GBD) Study recorded 1.2 million ACS cases. 10 The common comorbidities in patients with ACS are AF and HF. In India, the estimated incidence of HF ranges from 0.5 to 1.7 cases per 1,000 person-years, resulting in 492,000 to 1.8 million new cases annually. 11 The prevalence of AF in India exhibits significant variability, ranging from 0.1% to 1.6% in several studies. 12 Cardiovascular disease patients are mostly susceptible to influenza complications, such as acute MI (AMI), stroke, myocarditis, decompensated HF, thrombosis, and death. These consequences might be the result of an increase in proinflammatory and prothrombotic alterations, atherosclerosis, and cardiac arrhythmias. This clinical evidence from an Indian hospital-based observational study illustrating the prevalence and cardiovascular impact of influenza infection is summarized in Table 1.13–15
Globally, respiratory illnesses due to seasonal influenza result in an estimated annual mortality rate ranging from 291,000 to 646,000 affected people, out of which 36% of these fatalities occur in developing countries like India. India experiences an increase in circulation of the influenza virus primarily during June-September (monsoon) and in November-February (winter). 13 From 2010 to July 2020, India reported 173,488 seasonal influenza cases, with major outbreaks in 2015 and 2017 resulting in over 40,000 cases and approximately 2,300-3,000 deaths annually. The highest burden was concentrated in Maharashtra, Gujarat, Rajasthan, and Delhi. 16 A cross-sectional study among HF patients revealed that only 4.4% had received an influenza vaccine in the past 5 years. The awareness of risks associated with influenza and the availability of the vaccine were recorded at 7.5% and 12.5%, respectively. Importantly, only 6.5% of patients had been prescribed the vaccine by their physicians. The study identified poor vaccine uptake largely due to a lack of physician recommendation and misperceptions regarding vaccine safety and efficacy. The authors underscored the urgent need for interventions to improve awareness, both among patients and healthcare providers, and to enhance vaccination rates. 17
Summary of Indian Studies on Influenza Prevalence and Cardiovascular Outcomes.
Role of Influenza Infection in Cardiovascular Disease in the Indian Clinical Setting: Expert Opinion
Respiratory infections, both viral (respiratory syncytial virus [RSV], adenovirus, influenza) and bacterial, are common triggers for exacerbating chronic HF.
The panel underscored the difficulty in consistently obtaining a thorough history of recent respiratory infections, especially in areas with high levels of air pollution. They highlighted the importance of a standardized history, particularly about worsening HF and AF, as some patients may not volunteer this information willingly.
Viral infections were acknowledged as potential triggers for heart block and bradycardia.
Vaccination emerged as a crucial preventive measure against influenza-related complications, especially in highly susceptible populations, including diabetes, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), and HF patients.
Experts highlighted the importance of recognizing the impact of influenza on CVD and emphasized the potential effectiveness of vaccination in reducing associated complications.
Impact of Influenza Infection on Cardiovascular Diseases
A relationship involving influenza spread and major adverse cardiovascular events (MACE) has been continuously recorded from the early twentieth century. 18
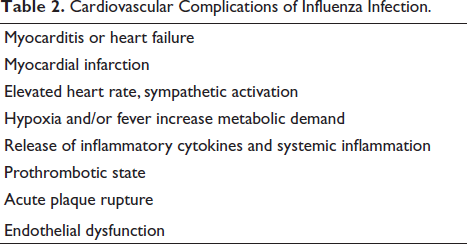
Multiple epidemiological findings related to influenza-associated cardiovascular complications are listed in Table 2. 19
Cardiovascular Complications of Influenza Infection.
Vascular Complications18, 20–24
Myocardial infarction: Several analyzes have revealed potential associations between influenza and subsequent MI and stroke.
Stroke: Studies have also reported an association between influenza and stroke.
Myocardial Complications19, 23, 25–29
Acute HF: Influenza is associated with a temporarily elevated risk of acute HF, and it may be the most common cardiovascular complication.
Myocardial injury: Elevated troponin levels (myocardial injury) are common among hospitalized influenza patients.
Myocarditis: The occurrence of clinically diagnosed myocarditis associated with influenza varies, with a higher prevalence observed in fatal influenza cases. The risk of ACS occurring after influenza is highest shortly following the infection; however, it persists at a higher level for a few months. 23 In a case series by Kwong et al., it was observed that among individuals hospitalized for AMI, the frequency of inpatient stays occurring within 7 days post-influenza infection (20 admissions/week) was six times greater than the total number of admissions in the year preceding and the year following influenza infection (3.3 admissions/week). 27 Subgroup analyzes among people >65 years revealed an increased chance of AMI following influenza diagnosis, who had never been hospitalized for AMI. 25
It has been suggested that influenza can induce cardiovascular complications by triggering a robust acute inflammatory response, which, in turn, might subsequently result in the acute rupture of plaque.5, 30, 31 Influenza can also worsen pre-existing CVD by increasing metabolic demand, activating the sympathetic autonomic nervous system, and reducing blood circulation to the coronary arteries due to pyrexia and tachycardia. 32 It can also lead to cardiovascular ailments such as myocarditis, pericarditis, HF, and arrhythmias. It can make patients more susceptible to opportunistic infections such as bacterial pneumonia, which can lead to a diminished oxygen supply to the heart muscle and a high vulnerability to cardiac complications. 33 A study conducted in more than 11,000 influenza patients reported an 18% rise in AF. 34 Furthermore, hospitalization rates for HF increased by 24%. 35 People who had HF hospitalizations with associated influenza illness had increased risks of death, respiratory, and renal failure. 3
Expert Suggestions
In complicated cases, prolonged hospitalization may predispose patients to pneumonia, especially in those with poor immunity due to chronic comorbidities like chronic HF, kidney, and liver diseases.
Influenza infection is not directly responsible for plaque deposition in ACS, but the inflammation resulting from the infection may trigger plaque rupture, leading to type I MI.
Type II MI, characterized by oxygen supply-demand mismatch, could result from influenza-induced acute febrile syndrome.
Patients with multiple risk factors, including diabetes mellitus and hypertension, are more prone to type I MI during influenza infection.
Those with diabetes mellitus, diabetic patients with CKD, morbid obesity, myocarditis, COPD, patients on chemotherapy, immunocompromised patients, chronic active smokers, and elderly individuals are highly susceptible to experiencing pneumonia and its complications.
In the Indian context, reducing cardiovascular events through IV is expected to result in a corresponding fall in mortality and morbidity, advocating for administering the vaccine to all patients deemed at high risk, regardless of age or risk status.
Influenza Vaccines for Reducing Cardiovascular Events: Clinical Efficacy and Effectiveness
Coronary Artery Disease
Clinical Potency of Influenza Vaccines in Coronary Artery Disease.
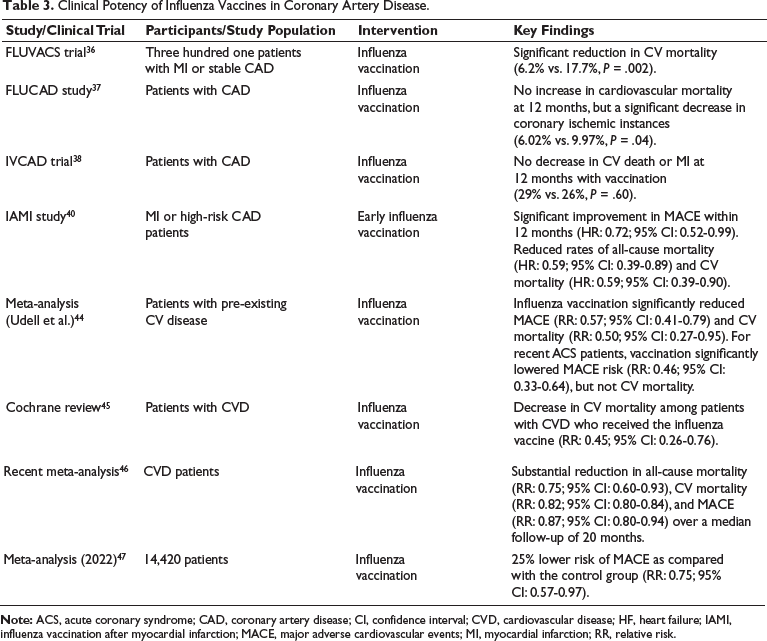
Influenza vaccination is considered a potential practice for decreasing CV events in individuals with CVD. Table 3 provides information on studies assessing the role of IV in minimizing CV risk in CAD. Multiple randomized controlled trials (RCTs) have yielded varying outcomes, emphasizing the importance of IV in CVD patients. The FLUVACS trial involving 301 patients who suffered MI or stable CAD demonstrated a significant reduction in CV death with vaccination (6.2% vs. 17.7%, P = .002). 36 Conversely, the FLUCAD study and IVCAD trial (patients with CAD) reported unchanged conditions in CV death or MI at 12 months but a significant decrease in coronary ischemic events.37, 38 A prospective open-label trial by Phrommintikul et al. revealed a diminished risk of significant cardiovascular problems (unadjusted HR: 0.70, 95% CI: 0.57-0.86), although no decrease in cardiovascular mortality. 39
A double-blind, randomized clinical trial, IAMI (IV after MI) aiming to assess the impact of early IV following admission for MI or high-risk CAD on reducing MACE within 12 months of the index event, demonstrated a significant improvement in the primary outcome in the vaccine group compared to the control group (HR: 0.72 (95% CI: 0.52-0.99)). Additionally, the vaccinated group exhibited reduced rates of secondary outcomes, including all-cause mortality (HR: 0.59 (95% CI: 0.39-0.89)) and cardiac mortality (HR: 0.59 (95% CI: 0.39-0.90)). 40 The investigators then combined their findings with those from the FLUCAD, FLUVACS, and Phrommintikul et al.’s study, revealing a remarkable 49% RR decrease in CV death (HR: 0.51 (0.36-0.71)).36–39
A self-controlled case-series study (SCSS)41 and an analysis of the UK General Practice Research Database (2001–2007) both demonstrated a reduced risk of acute myocardial infarction (MI) following vaccination. In the SCSS, the risk of MI was significantly lower during days 1–14 post-vaccination (relative risk [RR] 0.68; 95% confidence interval [CI] 0.60–0.78) compared with the baseline period, and this protective effect persisted during days 29–59 (RR 0.82; 95% CI 0.75–0.90). Importantly, both studies further indicated that regular immunisation was associated with a sustained reduction in MI risk.2, 41
A population-centered case-control investigation indicated that IV was linked to a reduced risk of primary cardiac arrest, which was out of hospital (OR: 0.51, 95% CI: 0.33-0.79). 42 This reduction was more significant among the older population (>65 years) in the 1998-1999 and 1999-2000 influenza seasons. Vaccination leads to decreased cases of hospitalization for heart disease (OR: 0.81, 95% CI: 0.73-0.89) and cerebrovascular disease (OR: 0.84, 95% CI: 0.72-0.97) across both seasons. Additionally, there was a notable decrease in all-cause mortality risk during these seasons, with odds ratios (ORs) of 0.52 (95% CI: 0.47-0.57) for 1998-1999 and 0.50 (95% CI: 0.46-0.55) for 1999-2000. 43
Udell et al. conducted a meta-analysis in which the primary endpoint was prolonged MACE, which includes cardiac mortality or hospitalization for unstable angina, AMI, HF, stroke, or emergency coronary revascularization. In their investigation involving patients suffering from CV disease, IV potentially decreased both MACE (RR: 0.57, 95% CI: 0.41-0.79) and CV death (RR: 0.50, 95% CI: 0.27-0.95). For those who experienced recent ACS within a year (n = 815), IV potentially lowered MACE risk (RR: 0.46, 95% CI: 0.33-0.64, I2 = 0%) but did not significantly affect CV fatality (RR: 0.44, 95% CI: 0.17-1.15; I2 = 38%) or overall mortality. Notably, no differences in MACE or CV death in patients with stable CAD was observed (n = 840). 44 A Cochrane review revealed a decrease in CV mortality among patients with CVD who received the influenza vaccine (RR: 0.45 (95% CI: 0.26-0.76)). 45 A recent meta-analysis, encompassing 4 randomized clinical trials and 12 observational studies in CVD patients, demonstrated a substantial reduction in all-cause mortality (RR: 0.75 (95% CI: 0.60-0.93)), cardiovascular deaths (RR: 0.82 (95% CI: 0.80-0.84)), and MACE (RR: 0.87 (95% CI: 0.80-0.94)) during a 20 months follow-up. 46 Additionally, another recent meta-analysis of eight trials involving more than 14,000 patients identified that IV was linked with a 25% diminished risk of MACE (RR: 0.75 (95% CI: 0.57-0.97)). 47 In relative terms, these risk decreases are similar in magnitude to therapy for CVD as advised in the guidelines.
Heart Failure
In a comprehensive review utilizing data available in the Danish national patient registry from 2003 to 2015, Modin et al. investigated the correlation between IV and the survival of recently diagnosed HF patients. There was 18% decrease in both total mortality (HR = 0.82, 95% CI: 0.81-0.84, P < .001) and CV death (HR = 0.82, 95% CI: 0.81-0.84, P < .001) associated with IV. Furthermore, the study highlighted that an annual, timely, and sustained vaccination regimen resulted in a significant decrease in the incidence of mortality compared to intermittent vaccination. 48 Similar findings were observed in a clinical trial based on HF, including six cohort studies by Rodrigues et al., reported a substantial decrease in HF hospitalizations (HR = 0.69, 95% CI: 0.55-0.86). 49
A study by Mohseni et al. used a primary care database linked to England’s hospitalization registry from 1990 to 2013, which included 52,202 patients. In this study, IV was linked to reduced chances of CV hospitalization (HR = 0.73, 95% CI: 0.71-0.76) and all-cause hospitalization (HR = 0.90, 95% CI: 0.95-0.98), with a more pronounced effect in younger patients. 50
Atrial Fibrillation
In a recent meta-analysis, a reduced risk of arrhythmia associated with vaccination (OR: 0.82, 95% CI: 0.70-0.97; P = .02; I2 = 76%) was markedly observed. Furthermore, subgroup analysis demonstrated a lowered AF chances (OR: 0.94, 95% CI: 0.90-0.98; P = .006; I2 = 0%) and, although not statistically significant, a positive trend regarding ventricular arrhythmias (VAs) (OR: 0.68, 95% CI: 0.42-1.11; P = .12; I2 = 85%) following IV. 51
Primary Prevention of Acute Cardiovascular Events
Limited studies have been conducted to study the primary prevention of acute cardiovascular events with IV. Davidson et al. conducted an observational study and reported a noteworthy reduction in the season-adjusted occurrence of initial acute CV complications within the 120-day risk window following flu vaccination. This reduction in the incidence ratio was particularly pronounced for MIs compared with other cardiovascular incidents. Interestingly, the timing of these events centered around the vaccination, with a significant portion happening before vaccination, especially in individuals aged 40-64 years. 52
A prospective cohort analysis by Nichol et al. involving patients aged 65 years or older during the 1999-2000 flu season revealed significant reductions in hospitalizations for various conditions, including influenza-pneumonia (29% decrease), HF (27% decrease), CVD (23% decrease), all-cause hospitalizations (24% decrease), and a 36% decrease in all-cause mortality. Even in low-risk groups without specific health conditions, IV was associated with significant reductions in cardiovascular and cerebrovascular events, all-cause mortality, and hospitalizations during follow-up.42, 52–55
Experts’ Recommendation
Expert recommendations highlight the advantages of IV for patients with pre-existing CVD.
High-risk groups, including those with a high atherosclerotic CVD (ASCVD) score, hypertension, diabetes mellitus, CKD, obesity, dyslipidemia, and those predisposed to HF, should receive IV for both primary and secondary prevention.
Timely vaccination, aligned with the WHO’s recommendations for the latest vaccine strains, is crucial for optimal protection against influenza. Annual IV is essential.
Priority for primary prevention should be given to high-risk groups, such as patients with hypertension, dyslipidemia, obesity, pulmonary hypertension, young MI patients, heavy smokers, COPD, and stroke patients.
Further research is needed on the use of the influenza vaccine for preventing CVD in healthy individuals.
Professionals strongly advocate for IV among patients with HF within the Indian setting.
Barriers to Influenza Vaccine Uptake
The comprehensive addressing of barriers across doctors, patients, and health systems is essential to improve IV rates. Key determinants of successful intervention implementation include medical knowledge, clear regulations, and an understanding of risk–benefit ratios. Notably, the experiences of physicians and healthcare workers with influenza immunization significantly impact patient recommendations, as endorsements from doctors have been shown to increase vaccination rates by 50%-93% across various studies. 56 Despite this, specialized practitioners may demonstrate reluctance regarding primary prevention interventions. Behavioral aspects of patients, such as complacency, inconvenience, lack of confidence, and calculation, also play crucial roles in vaccination decisions. Furthermore, sociocultural factors, including economic status, education, religion, and demographics, influence vaccination uptake. Overcoming these challenges requires strategic approaches, such as cautious dissemination of scientific information, expert review, social media campaigns, and public commitments by healthcare professionals.57–59
Experts’ Recommendation
Suggested development of a hospital checklist at discharge in cardiac units, emphasizing immediate vaccination for HF and AF patients, and encouraging prompt vaccination for ACS patients post-discharge.
Identified low IV rates in India are attributed to physician inertia, necessitating reminders for doctors to recommend vaccination.
Ensuring widespread availability of the influenza vaccine is recognized as crucial for improving vaccination rates.
Increased awareness among healthcare professionals, especially general physicians, regarding IV benefits is deemed necessary.
Proposed prioritization for vaccine eligibility includes patients with ACS, HF, and AF, followed by those with comorbidities or risk factors predisposed to heart disease.
Greater emphasis is needed on the importance of annual IV for all healthcare workers.
Conclusion
In conclusion, the article highlights the significant burden of CVDs in India, emphasizing the earlier onset, increased case fatality, and higher incidence of premature deaths. It underscores the well-established association between respiratory infections, particularly influenza, and adverse cardiovascular events, including ACS and cardiovascular mortality. Despite robust evidence supporting the cardioprotective benefits of IV, its integration into standard cardiology practice remains inconsistent globally. The consensus emphasizes the urgent need for widespread IV, especially among high-risk populations, to mitigate the substantial morbidity and mortality associated with cardiovascular complications. The experts recommend prioritizing vaccination for individuals with established CVDs, such as ACS, HF, and AF, while addressing barriers to uptake, including physician inertia and patient hesitancy. There is a pressing need to increase awareness and implement comprehensive strategies for regular vaccination and enhance the IV coverage in patients with CVD in India.
Footnotes
Acknowledgments
The authors acknowledge Parv Enterprise’s medical writing support and editorial assistance.
The expert group discussion was conducted in association with Abbott India Ltd. This article is based on the views expressed during the expert group discussion. The views expressed and discussed in the meetings and stated in this article are the independent views of the authors and not of Abbott India Ltd.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The expert group discussion was funded by Abbott India Ltd.
Patient Consent
This manuscript does not include individual patient data or identifiable information.