
Abstract
Extrinsic compression of the left main coronary artery (LMCA) by a dilated main pulmonary artery (MPA) is an important condition, and it should be looked for in patients with pulmonary arterial hypertension (PAH) with anginal symptoms. Left main coronary artery compression is defined as LMCA stenosis >50% with downward displacement of the vessel seen in coronary angiography due to dilated pulmonary artery (PA). Patients with PAH, irrespective of etiology, start to develop significant dilatation of the MPA. This enlarged PA results in compression of the LMCA, causing angina, syncope, heart failure, or arrhythmias, and they are at times responsible for sudden cardiac death. Here we have four patients with PAH of different etiologies. After evaluation with cardiac catheterization study and coronary angiogram, they were found to have LMCA compression. Two of them underwent percutaneous coronary intervention (PCI) for the LMCA disease, one of them underwent surgery for chronic thromboembolic pulmonary hypertension with PA reduction, and the last patient is under medical management. With this case series, we would like to highlight the need for having a low threshold for coronary angiogram irrespective of the age of the patient when patients with long-standing PAH present with exertional chest pain. Though the prognosis of severe PAH patients is guarded, this is a correctable condition and can offer patients a better quality of life after the PCI or surgery.
Keywords
Introduction
Extrinsic compression of the left main coronary artery (LMCA) by a dilated main pulmonary artery (MPA) is an important yet an under-recognized complication in patients with pulmonary arterial hypertension (PAH) with anginal symptoms. Left main coronary artery compression is defined as LMCA stenosis >50% with downward displacement of the vessel seen in coronary angiography due to dilated pulmonary artery (PA). It was first described by Corday et al. in 1957. 1 Irrespective of its underlying etiology, PAH often leads to significant dilatation of the MPA. In susceptible patients, this enlarged PA results in compression of the LMCA, causing angina, syncope, heart failure, or arrhythmias, and they are at times responsible for sudden cardiac death (SCD). Left main coronary artery compression is documented across various forms of PAH, including idiopathic PAH and PAH associated with congenital heart disease (CHD), such as patent ductus arteriosus (PDA), ventricular septal defect, and atrial septal defect (ASD).2, 3 In PAH patients with anginal symptoms, long-term outcome was good following percutaneous coronary intervention (PCI) to the LMCA. 4
We report four cases of PAH of differing etiologies. These patients underwent further evaluation with cardiac catheterization studies and coronary angiogram, which revealed this concerning issue. Two patients were successfully treated with PCI, one patient with chronic thromboembolic pulmonary hypertension (CTEPH) underwent surgery with PA reduction, and the final patient remained under optimal medical management. This case series highlights the need for high clinical suspicion and the variability of therapeutic approaches for this rare but critical condition.
Case 1
A 47-year-old gentleman, with a long-standing history of primary PAH, managed on pulmonary vasodilators since 2008, presented with a history of exertional angina and exertional breathlessness with a decrease in effort tolerance of 3 months duration. He also had an acute episode of chest pain with left arm radiation and sweating 1 month prior to presenting here, and an electrocardiogram (ECG) was suggestive of a left main equivalent pattern. Troponins were elevated, confirming a non-ST elevation myocardial infarction. A subsequent coronary angiogram showed significant left main disease of 80%-90% severity, prompting referral to our hospital for further management.
On examination, his vitals were normal, systemic examination revealed loud P2, and an early diastolic murmur was heard in pulmonary area. Electrocardiogram showed sinus rhythm, right axis deviation (RAD) with right ventricular hypertrophy (RVH) (Figure 1B). On chest X-ray PA view, there was an enlarged PA with peripheral pruning (Figure 1A). Echocardiogram revealed dilated right atrium (RA), right ventricle (RV), and MPA with PAH (moderate pulmonary regurgitation [PR] with end diastolic gradient of 27 mmHg).
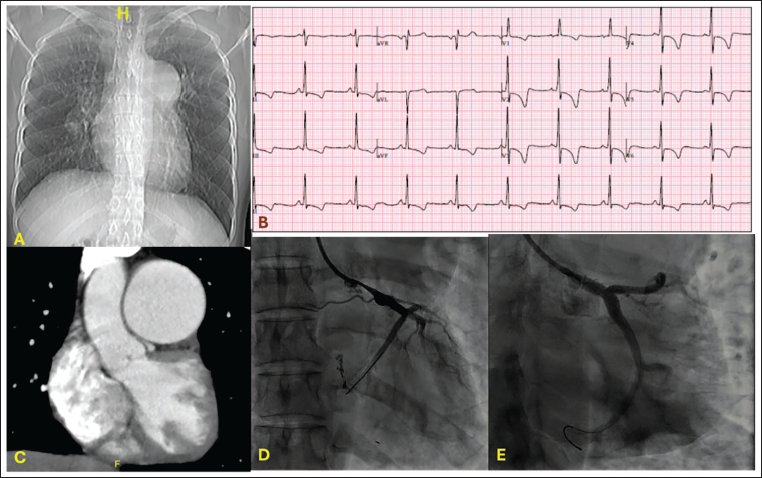
Cardiac computed tomography (CT) showed significant MPA enlargement, measuring 52 mm. Notably, the oblique coronal view revealed a slit-like configuration of the LMCA and a reduced LMCA takeoff angle, strongly suggesting extrinsic compression by the dilated MPA (Figure 1C).
In view of significant PAH, he was considered a high-risk candidate for surgery, and the LMCA lesion, being secondary to compression by dilated MPA, he was taken up for PCI. Left main coronary artery was stented from ostium into proximal left circumflex artery (LCx) with a 4.0 × 20 mm drug-eluting stent (DES) at 18 atm. Ostial flaring was done with the same stent balloon at 22 atm. Post-procedure angiogram showed good results with thrombolysis in myocardial infarction (TIMI) III flow (Figure 1E). The patient has remained asymptomatic and is currently doing well, continuing under regular follow-up for the past 3 years.
Case 2
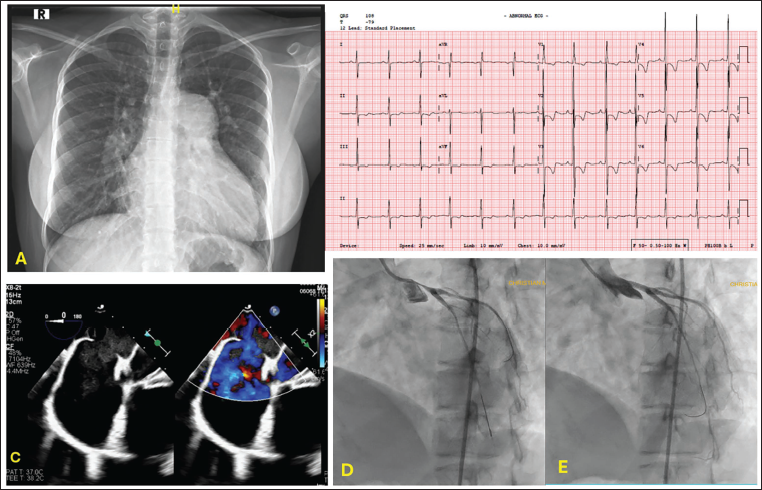
A 19-year-old girl presented with 2-year history of exertional breathlessness and intermittent chest pain. Her childhood history was uneventful. On presentation, she had mild conjunctival congestion, room air oxygen saturation of 93%, and auscultation revealed loud P2 with an ejection systolic murmur in the pulmonary area. Her ECG showed sinus rhythm, RAD, RV strain, and T-wave inversions in the lateral leads as well (Figure 2B). Her transthoracic echo (TTE) and transesophageal echo (TEE) confirmed dilated RA and RV with 25 mm ostium secundum ASD (OS-ASD) with bidirectional shunt and signs of pulmonary hypertension (PH), an estimated PA pressure of 80 mmHg, and moderate tricuspid and pulmonary regurgitation (Figure 2C).
Given the patient’s age and the severity of her PA pressures, which were disproportionate to the ASD size, a right heart catheterization (RHC) was performed to assess pulmonary vascular reactivity and resistance. Oximetry and pressure measurements revealed a pulmonary-to-systemic flow ratio (Qp/Qs) of less than 1 and a pulmonary vascular resistance index (PVRI) of 7 Wood units, consistent with irreversible PH. An aortic root angiography was performed to exclude co-existing anomalies, such as PDA, and unexpectedly revealed significant LMCA disease. So, a selective coronary angiogram was done. It showed almost 95%-99% LMCA stenosis with the left anterior descending (LAD) artery exhibiting competitive flow (Figure 2D). The patient was deemed to be at high risk for thoracic surgery in view of severe, irreversible PH. After thorough discussion and obtaining informed consent regarding the procedural risks, PCI was elected to address the critical LMCA stenosis. She underwent successful angioplasty with a single DES to LMCA, achieving an excellent post-procedural angiographic result (Figure 2E). Her immediate post-procedure stay was uneventful; she was subsequently started on pulmonary vasodilators, and the chronic nature of her disease was explained in detail to her family. Her clinical symptoms improved, and she remained under close follow-up.
Case 3
A 61-year-old gentleman presented with 2-3-month history of worsening breathlessness and swelling of legs. For the preceding 5-6 years, he was treated as a case of chronic obstructive lung disease elsewhere. Two weeks prior to presenting at our hospital, a CT pulmonary angiogram (CTPA) was performed, which revealed features suggestive of CTEPH. The scan showed subacute-to-chronic thrombosis in the main, right, and left pulmonary arteries, severe RV dilatation, and an MPA diameter of 42 mm. Emphysematous changes were also noted in both lungs.
Upon arrival, his saturation was 92%, he had pedal edema, and an elevated jugular venous pressure (JVP). On auscultation, he had an early diastolic murmur in pulmonary area and a pansystolic murmur in the tricuspid area. His ECG showed sinus tachycardia, RA enlargement, and RVH (Figure 3B). In echo, there was severe tricuspid regurgitation, dilated RA, and RV with an echogenic mass (thrombus) in the MPA. His PA pressure was high (90 mmHg). Further etiological evaluation of CTEPH was done, and it was negative. Given the strong evidence of CTEPH, the patient was scheduled for a pulmonary endarterectomy (PEA) by the thoracic surgery team, and a pre-operative catheterization study was done.
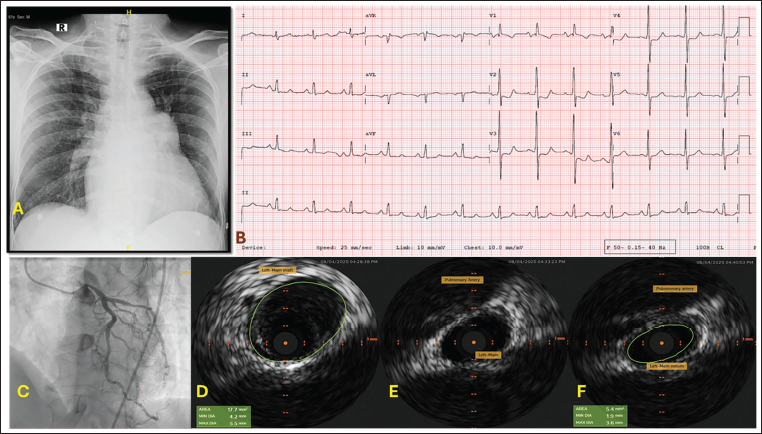
Right heart catheterization study confirmed precapillary PH, with a mean PA pressure of 48 mmHg and a pulmonary capillary wedge pressure (PCWP) of 7 mmHg. As part of the workup, coronary angiogram was done, and it showed significant LMCA stenosis (Figure 3C). Intravascular ultrasound (IVUS) revealed significant extrinsic compression of LMCA (minimal lumen area, MLA of 5.4 mm 2 during systole) (Figures 3D to F). As he was planned for PEA, he was advised PA reduction along with the same. He underwent the surgery—endarterectomy with significant improvement in his symptoms. He remained on regular follow-up and continued anticoagulation therapy.
Case 4
A 49-year-old gentleman presented with exertional dyspnea of 3 years duration. He otherwise did not have any traditional risk factors for atherosclerosis. On examination, he had a wide split S2 with an ejection systolic murmur in the pulmonary area. His ECG showed an RV strain pattern (Figure 4B). chest X-ray demonstrated an enlarged main and right PA with plethoric lung fields (Figure 4A). His echo revealed a large OS-ASD 34 mm in size with a left-to-right shunt. We advised a surgical closure as his defect was deemed unsuitable for a percutaneous device closure after TEE. Pre-operative workup included a coronary angiogram, which revealed LMCA compressed by the MPA (Figure 4C). To determine the significance of the stenosis, an IVUS was performed, which showed minimal atherosclerotic plaque in the LMCA, with an MLA of 17 mm 2 during diastole and 12 mm 2 during maximum compression (systole) (Figures 4D and E). We proceeded with a functional assessment of stenosis severity. Baseline distal-to-proximal pressure ratio (Pd/Pa) was 0.95, and a fractional flow reserve (FFR) in the proximal LAD was 0.94 after adenosine infusion. Hyperemia-free index at rest (resting full cycle ratio, RFR) was 0.89. Since the FFR and RFR values were above the established threshold of hemodynamic significance, the LMCA lesion was determined to be anatomically present but not functionally severe.
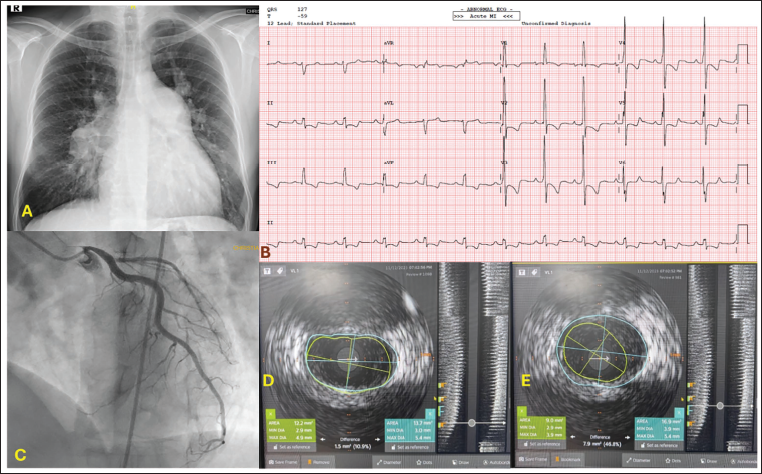
Based on these findings, the patient was advised to proceed with the surgical closure of the ASD as planned, and treatment for the minimal LMCA disease was limited to statin therapy. He remained under cardiology and surgical follow-up.
Discussion
Left main coronary artery compression by enlarged PA is a reversible cause of chest pain in patients with significant PAH. Classically, chest pain in patients with PH is predominantly due to elevated right-sided pressures resulting in RV strain, impairment of coronary perfusion, and RV ischemia. However, LMCA compression presents a distinct mechanism that requires specific diagnostic and therapeutic consideration. The ability of percutaneous therapy to relieve these symptoms in high-risk surgical patients underscores the importance of this diagnosis. 5
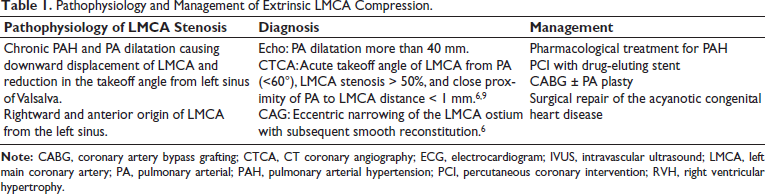
The mechanism (Table 1) involves the chronically enlarged PA causing a mechanical, downward displacement of the LMCA, resulting in a reduction of the vessel’s takeoff angle from the left sinus. 6 Anatomical risk factors, such as a rightward origin of the LMCA from the left sinus, further predispose the vessel to significant stenosis compared to a typical leftward origin.7, 8 The PA enlargement itself is a consequence of long-standing PH, which drives intimal thickening, medial hypertrophy, and arterial remodeling. Once sufficiently dilated, the PA impinges on the adjacent LMCA.
Pathophysiology and Management of Extrinsic LMCA Compression.
The entire spectrum of PH can develop this entity. It is most commonly noted in patients with idiopathic PAH. Next, it is commonly seen in patients with CHD (ASD) and PH, 10 Eisenmengerized PDA, followed by patients with CTEPH.
Left main coronary artery compression should be strongly suspected in any patient with PH presenting with chest pain, especially when the MPA diameter exceeds 40 mm. Cardiac CT plays a critical role in non-invasive diagnosis, as most patients undergoing PH evaluation will have had a CTPA or chest CT. A diagnosis is highly suggested if the CT demonstrates an MPA with diameter of more than 40 mm, an acute takeoff angle of the LMCA, and a stenosis exceeding 50% visible in the oblique coronal view.
Coronary angiography (CAG) and IVUS remain the gold standards for confirmation. CAG typically shows the LMCA ostium “squeezed” between the PA and the left sinus, with a smooth distal tapering. Intravascular ultrasound further clarifies the pathology, demonstrating a slit-like narrowing of the ostium with a characteristic absence of atherosclerotic plaque.
Crucially, functional assessment is vital to guide treatment, particularly in dynamic compression. As demonstrated by Velázquez Martín et al., PCI is often reserved for cases where IVUS reveals an MLA of less than 6 mm 2 . 11 Similarly, in our Case 4, IVUS MLA was adequate, and functional evaluation using FFR and RFR showed values above the ischemic threshold, confirming that the anatomical compression was not hemodynamically significant, thereby supporting a strategy of medical management alone.
Treatment selection balances the high surgical risk of the patient population with the need for revascularization. Percutaneous coronary intervention is considered a feasible, lower-risk option for addressing LMCA stenosis. 12 Standard coronary artery bypass grafting (CABG) carries a high risk of mortality in patients with severe PH, primarily due to the exacerbation of pre-existing RV dysfunction post-operatively. Percutaneous coronary intervention has thus evolved as an effective primary management option. In one of the large studies by Galiè et al. in 2017, out of 765 patients with PAH (esp CHD), 48 patients (6%) had LMCA compression with angina, with coronary angiography showing >50% LMCA stenosis. Almost 45 patients underwent PCI, and three underwent PA plasty. Post-PCI, 91% patients had relief of anginal pain. 4 Though technically there is a chance of stent compression and fracture with PCI, among the 45 patients who underwent angioplasty in the study by Galiè et al., only one had mechanical recoil, and among 53 patients who underwent angioplasty in a study by Saia et al., only one had stent recoil in follow-up.4, 5 A meta-analysis by Badea et al. further supported this, reporting pooled mortality after stenting was 2.7% at 22 months of mean follow-up, with 83% of survivors having no angina at follow-up. 13
Surgical Management
In specific cases, a surgical approach that addresses the underlying PA dilatation is appropriate. In our Case 3 (CTEPH), PEA, the definitive treatment for CTEPH, was combined with PA reduction (arterioplasty) to anatomically relieve the compression, resulting in significant clinical improvement.
Our case series reinforces the diverse etiologies and management spectrum of this condition, including idiopathic PAH, ASD-associated PH, and CTEPH. All four patients presented with anginal symptoms, where CT coronary angiography (CTCA) was highly helpful, and CAG was confirmatory. Our favorable outcomes across different management arms—two patients successfully treated with PCI, one with surgical PA reduction (PEA), and one with functionally non-significant disease managed medically—demonstrate that a tailored approach, guided by advanced imaging (IVUS) and functional assessment (FFR/RFR), is essential. There have been multiple case reports of this condition managed by PCI or surgery in other countries. Given the few studies reported in India addressing this entity,14, 15 our series provides valuable local evidence regarding the diagnosis and successful management of this critical complication.
Conclusion
When PAH patients present with angina, syncope, or exertional fatigue, it is important to have a low threshold for CTCA, CAG ± IVUS imaging, and functional assessment, irrespective of the age of the patient and etiology of the PH. Currently, this entity of extrinsic compression of LMCA by dilated MPA is increasingly recognized, and there is significant relief of symptoms with PCI. There is a need for larger studies on its prevalence and long-term outcome in India. Though the overall prognosis of severe PAH patients is guarded, this is a correctable condition and can offer patients a better quality of life with survival benefit.
Footnotes
Declaration of Conflicting Interests
The authors declare no conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
The authors received approval from the Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written consent was taken from the patient concerned for the publication of this manuscript.