
Abstract
Introduction
Coronary artery disease is a leading global cause of mortality, particularly from acute ST-elevation myocardial infarction (STEMI). The SYNTAX score helps assess coronary complexity and guides choosing treatment options. This study evaluates its prognostic utility in primary angioplasty for ST-elevation myocardial infarction and identifies determinants of in-hospital mortality and major adverse cardiovascular events during follow-up.
Methods
This retrospective study at a tertiary cardiology center in Central India assessed 589 ST-elevation myocardial infarction patients who underwent primary percutaneous coronary intervention from January 2018 to June 2023. The SYNTAX score was calculated from initial angiograms, categorizing patients into low-, intermediate-, and high-risk groups. Clinical outcomes, including major adverse cardiovascular events and in-hospital mortality, were analyzed over a median follow-up of 1,278 days.
Results
Of the 589 patients, 456 (77.4%) completed follow-up. The mean SYNTAX score was 15.2 ± 6.71, with 82.7% classified as low risk. Major adverse cardiovascular events occurred in 73 (16.0%) patients, with 50 (10.9%) experiencing cardiovascular death. Higher SYNTAX scores were significantly linked to worse outcomes, including in-hospital mortality rates: 1.6% (score <22), 7.4% (22-32), and 12.5% (>32) (P = .002). Multivariate analysis identified age, SYNTAX score as independent predictors of adverse outcomes, and females had more in-hospital mortality rates.
Conclusion
The SYNTAX score is a robust predictor of in-hospital death and short- to mid-term major adverse cardiovascular events in ST-elevation myocardial infarction patients undergoing primary angioplasty.
Introduction
Coronary artery disease (CAD) is a leading global cause of death, with a growing incidence in countries like India. Acute ST-elevation myocardial infarction (STEMI), the most severe CAD manifestation, carries a community mortality rate of 15%-20%. The CREATE 1 and Kerala acute coronary syndrome (ACS) 2 registries in India reported STEMI as comprising 60% and 37% ACS cases, respectively, with the highest mortality within the ACS spectrum. However, access to primary percutaneous coronary intervention (PCI)—the gold standard for STEMI—remains limited in India due to cost and availability. For example, only 12.9% of STEMI patients in the Kerala registry received primary PCI, underscoring the urgent need for expanded access to timely care.
The SYNTAX (Synergy Between PCI with Taxus and Cardiac Surgery) score was designed to assess CAD anatomical complexity, aiding decision-making between PCI and coronary artery bypass grafting (CABG). While SYNTAX has shown prognostic value in stable ischemic heart disease and multivessel CAD, its role in predicting long-term outcomes, such as major adverse cardiovascular events (MACE), in STEMI patients undergoing primary PCI is less studied. This single-center study in Central India aims to evaluate the SYNTAX score’s prognostic utility and determinants of MACE in STEMI patients post-primary angioplasty, aiming to enhance STEMI management and outcomes in a real-world, resource-limited setting.
Materials and Methods
This single-center, retrospective study was conducted at a tertiary cardiology center in Central India, including all STEMI patients who underwent primary PCI from January 2018 to June 2023. Patients with incomplete data or lost to follow-up were excluded. SYNTAX scores were calculated from the initial angiogram using an online tool, categorizing patients into low-, intermediate-, and high-risk groups.3, 4 SYNTAX scoring was done independently by two interventional cardiologists, and in cases of discrepancy, a third experienced interventional cardiologist was consulted to finalize the SYNTAX score by consensus. Primary outcomes were MACE events, including all-cause mortality, nonfatal myocardial infarction (MI), and stroke, defined by the Academic Research Consortium-2 guidelines. 5
Data collection followed the Declaration of Helsinki and local regulations, and the collected data included demographics, clinical profiles, comorbidities, lab values, 2D echocardiography, CABG findings, and procedural details. Follow-up for MACE and other outcomes was conducted via electronic records and phone calls, ranging from 1 to 5.5 years. Adult patients (≥18 years) with STEMI undergoing primary PCI (including those with left main (LM) involvement) were included, while patients with prior CABG, incomplete angiographic data were excluded from the cohort.
Data analysis was done in Statistical Package for the Social Sciences (SPSS) (v12), with categorical variables presented as frequencies and continuous variables as means ± standard deviation (SD) or medians interquartile range (IQR). Categorical comparisons used chi-square or Fisher’s exact test, and continuous comparisons used Student’s t-test or Mann–Whitney U-test. Time to MACE was assessed by Kaplan–Meier analysis, with P < .05 as significant.
Results
A total of 589 patients presenting with STEMI underwent primary PCI. Baseline characteristics, angiography, and procedural details were examined for all 589 patients. However, out of these, 133 patients (22.6%) were lost to follow-up. Therefore, the final cohort for outcome analysis included 456 patients with a median follow-up duration of 1,278 days (IQR: 701-1,855 days).
Baseline Characteristics
Table 1 depicts baseline characteristics of the study population. The mean age of the cohort was 60.0 ± 11.96 years, with 49.1% (n = 289) of patients being older than 60 years. The majority of patients were male (82.3%, n = 485), while females comprised only 17.7% (n = 104) of the population.
Comorbidities were prevalent in this cohort, with 47.7% (n = 281) of patients having hypertension and 45.0% (n = 265) having diabetes mellitus. Left ventricular ejection fraction (LVEF) was significantly impaired across the study group, with a mean LVEF of 38.1% ± 8.5%. A substantial proportion of patients (69.5%, n = 317) had an LVEF ≤40%, reflecting a high-risk population with a considerable burden of left ventricular dysfunction.
Type of ST-elevation Myocardial Infarction
All patients presented with STEMI, with anterior wall infarctions being the most common, affecting 55.7% (n = 336) of cases. Inferior wall STEMI was observed in 37.9% (n = 231) of patients, while lateral and posterior wall infarctions occurred in 1.7% (n = 18) and 0.7% (n = 4) of cases, respectively.
Angiographic and Procedural Characteristics
Table 1 also illustrates the angiographic and procedural characteristics of the cohort. The mean SYNTAX score of the cohort was 15.2 ± 6.71, with 82.7% (n = 487) of patients having a SYNTAX score of <22, indicating relatively low anatomical complexity. In contrast, 16.0% (n = 94) had a moderate SYNTAX score of 22-32, and only 1.4% (n = 8) had a high SYNTAX score (>32), representing complex coronary disease.
Baseline Characteristics.
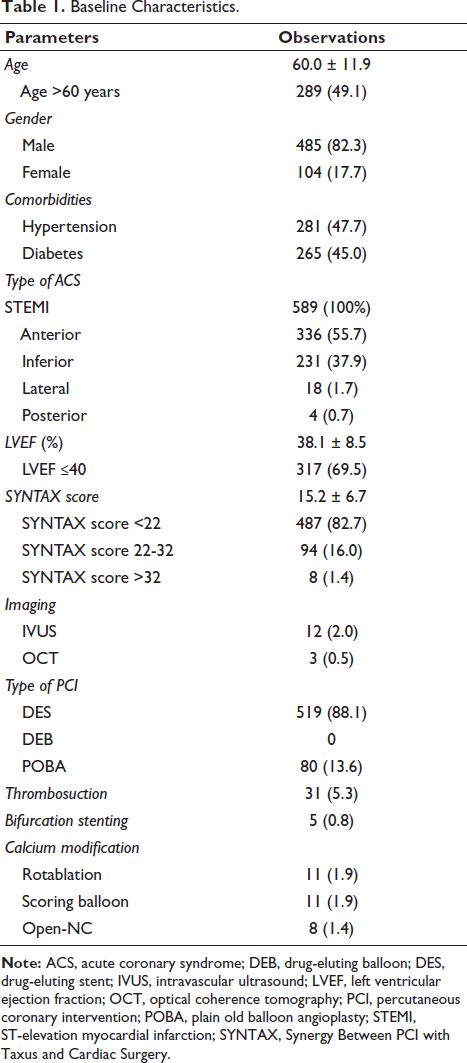
Intravascular ultrasound (IVUS) was used in 2.0% (n = 12) and optical coherence tomography (OCT) was used in 0.5% (n = 3) of cases. Drug-eluting stents (DESs) were employed in most cases (88.1%, n = 519), while plain old balloon angioplasty (POBA) was used in 13.6% (n = 80), with no cases of drug-eluting balloon (DEB) usage. Thrombosuction was performed in 5.3% (n = 31) of cases, and bifurcation stenting was performed in 0.8% (n = 5). Rotablation and scoring balloons were each used in 1.9% (n = 11) of cases, while Open-NC balloons were utilized in 1.4% (n = 8) for lesion modification.
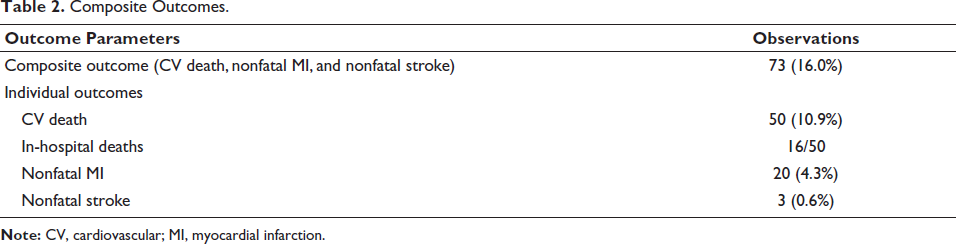
Composite Outcome
After excluding 133 (22.6%) patients who were lost to follow-up, in the remaining 456 cases, the composite outcome occurred in 73 (16.0%) cases as depicted in Table 2, over a median follow-up of 1,278 days (IQR: 25-75: 701-1,855 days).
Composite Outcomes.
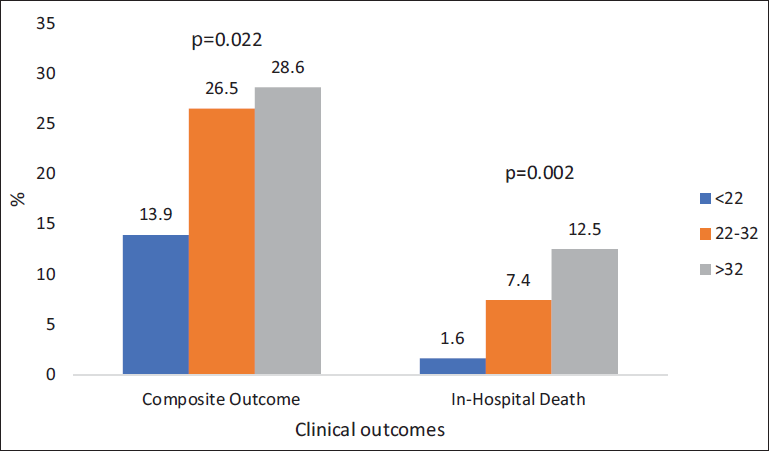
Survival Outcomes by SYNTAX Score (Figure 1)
The bar chart displays clinical outcomes—specifically the composite outcome and in-hospital death—across three groups with SYNTAX scores: <22, 22-32, and >32. The incidence of the composite outcome (cardiovascular death, nonfatal MI, and nonfatal stroke) significantly increases with higher SYNTAX scores, with rates of 13.9%, 26.5%, and 28.6%, respectively (P = .022). In-hospital death also shows a statistically significant trend, with rates of 1.6%, 7.4%, and 12.5% as SYNTAX scores increase (P = .002). This suggests that patients with higher SYNTAX scores experience worse clinical outcomes, both in-hospital and on follow-up.
Composite and In-hospital Outcomes by SYNTAX Score Groups.
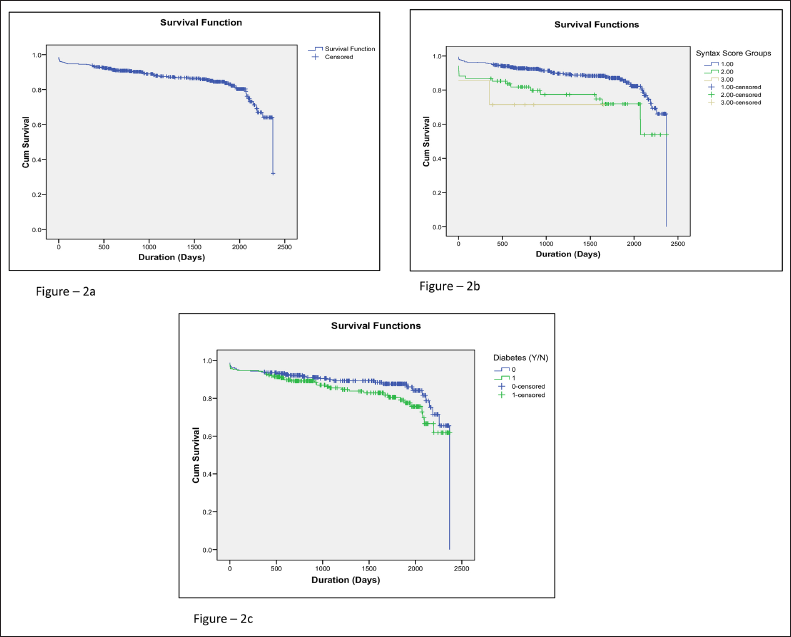
Results Based on Kaplan–Meier Survival Analysis (Figure 2)
Overall survival: The Kaplan–Meier curve illustrates survival trends among study participants, with a median follow-up of 1,278 days, indicating long-term outcomes after primary PCI in STEMI patients.
Survival based on SYNTAX score groups: Significant differences in survival were noted among SYNTAX score categories (<22, 22-32, and >32). Mean survival was 2,094.6 days for scores <22, 1,804 days for scores 22-32, and 1,228 days for scores >32, with a statistically significant difference (χ2 = 11.034, P = .004), highlighting the impact of higher SYNTAX scores on survival.
Survival in patients with and without diabetes: Kaplan–Meier curves for diabetic and nondiabetic patients revealed no significant survival difference (mean survival: 1,988.6 days for diabetics versus 2,091.6 days for nondiabetics, χ2 = 2.156, P = .142), suggesting diabetes did not significantly affect survival in this cohort.
(a) Kaplan–Meier (K–M) Curves for Overall Survival in Study Participants. (b) K–M Curves for Survival in Different SYNTAX Score Groups. (c) K–M Curves for Survival in Patients With and Without Diabetes.
Results of Composite Outcome Analysis (Table 3)
Table 3 depicts the relation of clinical parameters and their odds and significance with the composite adverse outcomes. With each additional year increased, the odds of complications increased by 6% (adjusted OR: 1.06, P = .002), while higher SYNTAX scores similarly elevated the risk, also adding 6% to the odds per unit (adjusted OR: 1.06, P = .002). Although male sex was initially associated with lower odds of adverse outcomes, it became nonsignificant in multivariate analysis, and while low (LVEF <40%) was more frequent in adverse cases, it did not reach statistical significance.
Relationship between Clinical Parameters and Their Odds with Composite Adverse Outcomes.
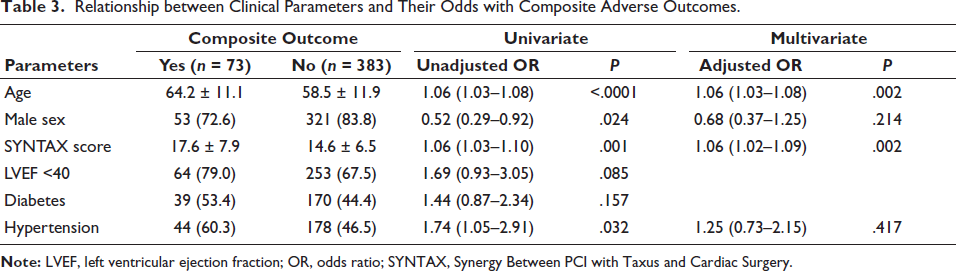
Composite Outcome Predictors (Table 3)
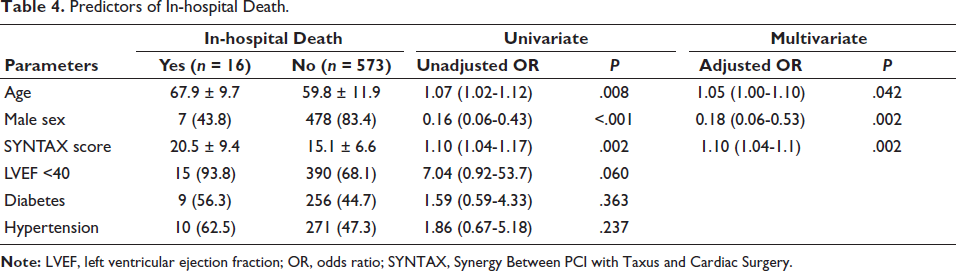
Predictors of In-hospital Mortality (Table 4)
Patients who died in the hospital were notably older than those who survived (67.9 vs. 59.8 years). In univariate analysis, each 1-year increase in age was associated with a 7% higher odds of in-hospital death (OR: 1.07, P = .008). This association remained significant in multivariate analysis, with a 5% increased risk per year (OR: 1.05, P = .042). Interestingly, male sex appeared protective: only 43.8% of those who died were male compared to 83.4% among survivors. In univariate analysis, being male was associated with an 84% lower odds of death (OR: 0.16, P < .001), and this protective effect persisted even after adjusting for other factors (OR: 0.18, P = .002). Patients who died also had higher SYNTAX scores on average (20.5 vs. 15.1), with each 1-point increase in the score associated with a 10% higher risk of death in both univariate and multivariate analyses (OR: 1.10, P = .002 for both).
Low LVEF (<40%) was highly prevalent among those who died (93.8% vs. 68.1%), showing a strong association with mortality in univariate analysis (OR: 7.04), though this did not reach statistical significance (P = .060), and it was not included in the multivariate model, possibly due to a borderline P value or collinearity. Diabetes was slightly more common in those who died (56.3% vs. 44.7%), but this difference was not statistically significant (OR: 1.59, P = .363). Similarly, hypertension was more prevalent among non-survivors (62.5% vs. 47.3%) but was not a significant predictor of in-hospital mortality (OR: 1.86, P = .237).
Predictors of In-hospital Death.
Discussion
This study assessed the prognostic utility of the SYNTAX score in primary PCI for STEMI patients, focusing on in-hospital mortality and short- to mid-term adverse cardiovascular events in a high-risk cohort from Central India. The SYNTAX score, typically used to gauge CAD complexity and guide treatment choices, is less established as a predictor of outcomes in primary PCI cases. While only two Western studies have explored this link, no research from the Asian subcontinent has examined the SYNTAX score’s predictive value for primary PCI outcomes. Our study, featuring one of India’s largest primary PCI datasets, provides essential insights, especially given the rising cardiovascular event rates in the Indian population.
The baseline demographics of our cohort revealed a mean age of 60.0 ± 11.96 years, with high rates of hypertension (47.7%) and diabetes (45%), consistent with Dubey et al.’s findings on STEMI patients undergoing primary PCI in India. 6 The elevated prevalence of these conditions reflects an increasing cardiovascular risk profile in the country.
Our results align with Gao et al.’s study, showing a strong correlation between higher SYNTAX scores and adverse outcomes. 7 Patients with SYNTAX scores >22 had significantly higher in-hospital mortality (7.4% for scores of 22-32 and 12.5% for scores >32), confirming the SYNTAX score’s effectiveness in predicting procedural complexity and CAD burden. The long-term MACE rate in our study was 16% over a median follow-up of 1,278 days, similar to findings by Garg et al., which also indicated that higher SYNTAX scores correlated with increased adverse events in STEMI patients.
Age emerged as a strong predictor of both in-hospital mortality and MACE, with each additional year increasing the risk by 5%-6%. This supports Dubey et al.’s conclusion that age is a critical factor in Indian STEMI outcomes, warranting its inclusion in risk stratification. Interestingly, male sex appeared to be independently protective against in-hospital mortality, with significantly lower odds of death in both univariate (OR: 0.16, P < .001) and multivariate analyses (OR: 0.18, P = .002), as only 43.8% of non-survivors were male compared to 83.4% among survivors. Female patients showed higher in-hospital mortality than males, likely due to delayed presentation and higher baseline risk, although gender did not independently predict MACE, emphasizing the need for age- and gender-specific considerations in treatments.
Additionally, each unit increase in the SYNTAX score raised the in-hospital mortality risk by about 10%, reaffirming its reliability as a prognostic marker, as noted by Gao et al. and Garg et al.7, 8 While low LVEF (<40%) was associated with increased mortality, it was not statistically significant, potentially due to a smaller sample size. Also, SYNTAX scores can appear skewed in cases involving LMCA lesions or diffusely diseased vessels. This is because the scoring system assigns higher baseline points to LMCA involvement (five for right dominance, six for left), and additional points for long lesion length and multi-segment disease.
Unlike previous findings of primary PCI in the Indian population, diabetes and hypertension, however, were not independent predictors of adverse outcomes, possibly because of short follow-up periods, and a sizable patients (22.6%) who lost to follow-up and were omitted from outcome analysis could have influenced these outcomes.
Limitations
This study’s single-center design may limit the generalizability of the findings, and the 22.6% follow-up loss may affect the accuracy of MACE estimates and influence the identification of outcome determinants. The short- to mid-term follow-up period also limits insights into long-term prognostic trends, necessitating further studies with extended follow-up durations. Additionally, the use of telephonic follow-up methods may have introduced variability in the data quality. The correlation of our variables, like Window period, Syntax II, could not be used because other variables could not be completely gauged in the cohort, as the study was retrospective in nature.
Conclusion
This study confirms the SYNTAX score’s value in predicting both in-hospital and long-term adverse outcomes in STEMI patients treated with primary PCI. Age, sex, and higher SYNTAX scores were key predictors of mortality, highlighting the SYNTAX score’s role in stratifying patient risk effectively. These findings may help inform risk-based management strategies for STEMI patients in India, aiding patient care in resource-limited settings like ours and potentially improving patient outcomes.
Key Message
What is already known: The SYNTAX score assesses CAD complexity and guides treatment decisions.
What the study adds: It confirms SYNTAX score’s robustness in predicting in-hospital and short- to mid-term adverse outcomes in patients with STEMI undergoing primary PCI.
Footnotes
Acknowledgment
The authors thank Ms. Ankita Jivtode and Karuna Gajbhiye for their contribution to data assimilation.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted as per the Principles of the Declaration of Helsinki. The data collection was started after approval from the local institutional ethics committee, that is, Criticare Hospital and Research Institute—EC/CHRI/24/65 on July 22, 2024.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
As this was a retrospective evaluation of existing data, informed consent was not required.